Fifth stage
SurgeryLec-
د. أسامة
6/4/2017
Neonatal Intestinal Obstruction(N.I.O)Presentation of neonatal intestinal obstruction(N.I.O)
Bilious vomiting(Always N.I.O until prove otherwise)
Abdominal distention (Depend on the level of I.O)
Failure to pass meconuim
COMMON CAUSES OF NEWBORN BOWEL OBSTRUCTION:
1-Mechanical:Intestinal atresia
Malrotation with midgut volvulus
Meconium ileus (mostly due to cystic fibrosis)
Meconium plug
Small left colon syndrome (diabetic mothers)
Segmental volvulus (without malrotation)
Meconium peritonitis (with perforation, adhesions, and pseudocyst formation)
Incarcerated hernia (inguinal, diaphragmatic, internal)
Necrotizing enterocolitis
Duplication
Anorectal malformation
2-Functional:
Hirschsprung's disease (congenital megacolon)
Paralytic ileus (usually secondary to sepsis,Peritonitis, Hypokalemia and uremia)
Maternal drugs - magnesium, Valium, heroin .
Doudenal Atresia :
Etiology:
Due to failure of recanalization .
Associated anomalies:
Low birth weight - (50%)
Down's syndrome - (30%)
Malrotation - (50%)
Symptoms:
Maternal polyhydramnios, Bilious vomiting, noabdominal distention .
X-rays :

X-ray show double bubble appearanceDifferential diagnosis:-1-Doudenal atresia2-Malrotation with volvulus
Management
Pre-op:
1) NG decompression
2) IV hydration
3) Antibiotic
Surgery: transverse supraumbilical incision, duodenoduodenostomy Diamond shape anastomosis .
SMALL BOWEL ATRESIAS :
Etiology :
Vascular occlusion of the vessel which supply this involved part of the bowel with aseptic necrosis and resorption.
This occlusion probably due to defect in mesenteric arcade or due to intrauterine volvulus.
Associated Anomalies:
Low incidence of other anomalies
Low birth weight
Meconium ileus
Symptoms
Maternal polyhydramnios
bilious vomiting,
abdominal distension
X-rays
Multiple dilated loops, air-fluid levels
Barium enema: microcolon
Management
Pre-op:
IV hydration (fluid bolus)
NG decompression
Antibiotics
Surgery: Transverse supraumbilical incision, resection with reanastomosis.
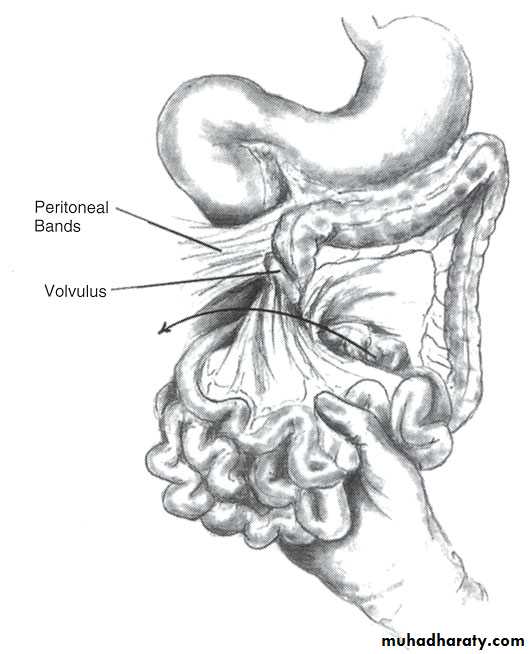
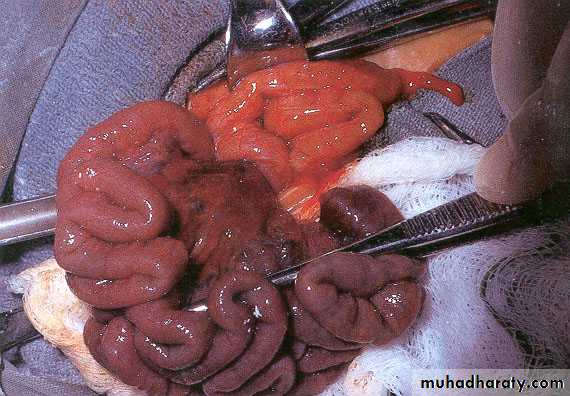
MALROTATION AND MIDGUT VOLVULUS
Lack of retroperitoneal fixation of bowel and presence of Ladd’s bands
partial or complete duodenal obstruction .
bowel may twist around SMA axis = volvulus .
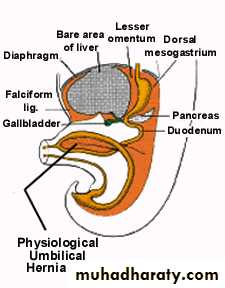
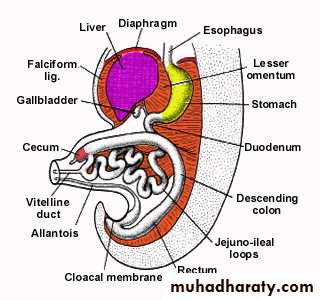
Week 6 Physiological Umbilical Herniation
As a result of rapid growth and expansion of the liver, the abdominal cavity temporarily becomes too small to contain all the intestinal loops.
The intestinal loops enter the extraembyronic cavity within the umbilical cord during the sixth week of development.
As herniation occurs, the loop undergoes a 90 degree counterclockwise rotation around the superior mesenteric artery.
Week 10 Return to Abdominal Cavity
During 10th week of development, herniated intestinal loops begin to return to the abdominal cavity.Undergoes additional 180 degree counterclockwise rotation about the superior mesenteric artery.
Symptoms
Acute:bilious vomiting often with a scaphoid abdomen
75% onset symptoms in first week of life (usually first three days),
volvulus present in 85%
Chronic: (due to Ladd's bands or intermittent volvulus)
cyclic abdominal pain .
bilious vomiting
malabsorption
Radiography
Abdominal X-ray: duodenal obstruction - dilated stomach, gasless abdomen or paucity of gasbeyond duodenum
Ba.meal and follow through shows duodenojejunal junction to the Right of midline, more cephalic
Barium enema - cecum in left iliac fossa (helps confirm, but not diagnostic)
Malrotation :
Management
Pre-op:1) IV hydration; 120-150 ml/kg per day
2) NG decompression
3) Antibiotics
Surgery:Emergency laparotomy when unable to rule out volvulus
Principles of the operation:-1-Do derotation ,counterclockwise.
2-Straightening of the doudenum
3-Excision of ladds band.
4-Widining of the mesentery.
5-Appendescectomy.
MECONIUM ILEUS :
Neonatal intestinal obstruction due to inspisated abnormal thick meconium in terminal ileum.Etiology:
Occurs in 10-15% of patients with cystic fibrosis. Very rarely occurs in the absence of cystic fibrosis (pancreatic enzyme deficiency).
Types:
1-50% simple or "uncomplicated"
2-50% are complicated and associated with volvulus, atresia, Intestinal perforation causing meconium peritonitis .
Symptoms:
1-Abdominal distension with bilious aspirates through the NGT.
2-Abdominal palpation shows doughy feeling with palpable intestinal loops
3-PR. no meconium in rectum.
Diagnosis
X-rays:
Multiple dilated loops and coarse granular appearance (“groundglass”), no air fluid levels, calcifications .
Barium Enema:Microcolon
Positive sweat test:
Na > 60 mEq
Cl > 60 mEq
Genetic testing .
Management:
Simple Meconium Ileus
40-60% can be handled non-operatively therapy
1) IV hydration (fluid bolus prior to enema)
2) antibiotics
3) NG decompression
4) Gastrografin enema (hyperosmolar)
monitor urine output and hemodynamics since the hyperosmolar enema can lead to severe hypovolemia.
must reflux back into dilated loops to be successful repeat in 12-24 hours if necessary
5) N-acetyl-cysteine enema if gastrograffin unsuccessful inproviding full Evacuation
6) begin oral feedings (Pregestimil)
Surgery:
if enema fails, proceed to surgery1) Supraumbilical transverse incision
2) Enterotomy with evacuation of meconium and pellets
3) Irrigate intestine with 1% N-acetyl cysteine
4) Primary closure of enterotomy if bowel healthy or consider ileostomy if health of bowel questionable .
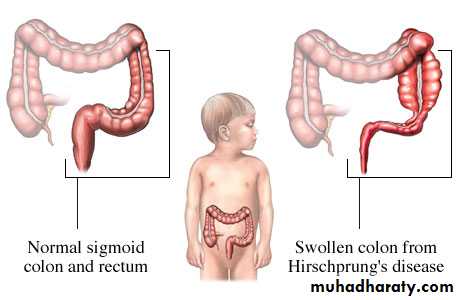
Hirschprung’s Disease
Aim:-
What is Hirschprungs disease
How to diagnose Hirschprungs disease
What is hirschprubgs enterocolitis
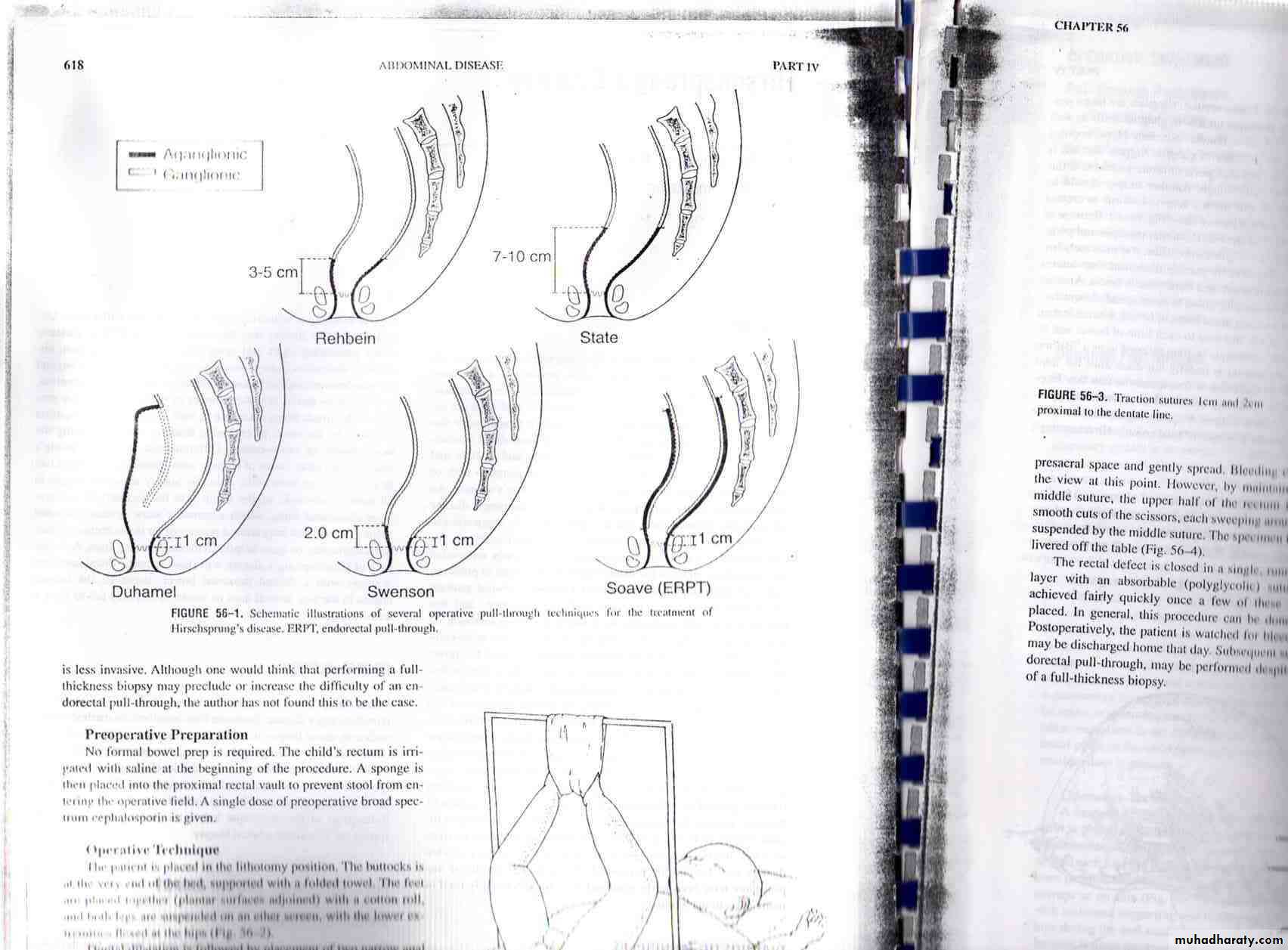
Out line for surgical treatment
More than 50 years old since the discovery of the cause and the treatment for Hirschprung disease.
Incidence : 1 in 5000 live birth
Male to Female is 4-1 .
The primary defect is the absence of the intramural ganglion cells of the submucosal and myenteric plexuses as the result of a defective migration of ganglion cell precursors of the neural crest into the hind gut.
This absence of normal parasympathatic innervation prevents gut peristalsis, leading to functional constipation.
The proximal colon hypertrophied by trying to overcome functional obstruction.
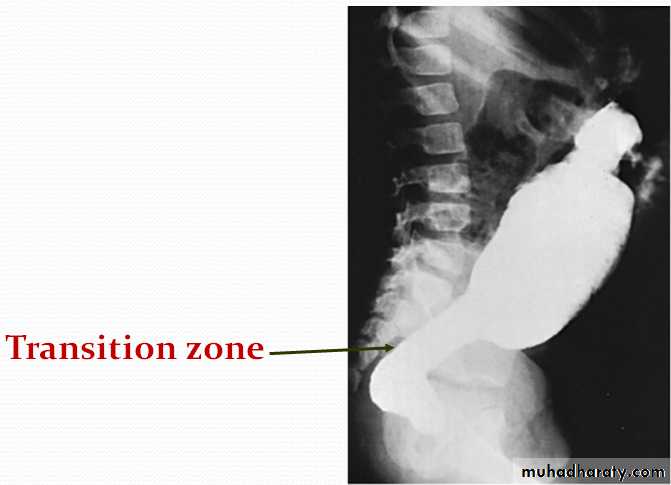
Transitional zone exists between normal and abnormal aganglionic intestine.
Visible transitional zone :

To rectosigmoid in 75%
Short segment (rectum)Ultra short (part of the rectum)
Long segment
Total aganglionosis (large intestine, sometimes a part of small intestine) up to 10%
Segmental .
Presentation :
varies from patient to patient depending on the length of the involved segment.Infant:-
95% - failure to pass meconium in first 24 hours life . Chronic contipation and abdominal distentionOlder children :–
Chronic constipation, failure to thrive
Hirschsprung’s enterocolitis:-
10-15% will have severe diarrhea and billious vomiting alternating with constipation.
“Neonatal bilious emesis is a surgical emergencyuntil proven otherwise”
Diagnosis:Barium enema will reveal a transition zone with narrow segment and dilated proximal portion. Late films will show retention of barium at 24- 48 hours.
Rectal biopsy is the most reliable diagnostic measure
HistopathologyAbsence of ganglionic cells
Hypertrophic cholinergic nerve trunks
Limited number of adrenergic fiber
Anorectal manometry
Absent rectoanal inhibitory reflexLack of internal anal sphincter relaxation in response to rectal stretch
Complicatons :
intestinal perforation (particularly at the appendix)enterocolitis,
malnutrition, failure to thrive, and anemia.
Water intoxication from frequent tape water enema .
Pathophysiology of enterocolitis :
Colonic stasisovergrowth of bacteria(Clostridium deficile)Invasion of bacteria to the epithelium(Translocation)inflammation (entercollitis)septiceamia.PRESENTATION OF ENTEROCOLITIS :
Abdominal distension .
Explosive foul-smelling diarrhea .
Bilious vomiting .
Fever .
Lethargy .
Colonic perforation / shock .
DIAGNOSIS OF HD ENTEROCOLITIS :
Diffusely tender, distended abdomen .Digital rectal exam results in explosive gas and stool .
Errect abdominal x-ray :-Air fluid levels .
Contrast enemas is contraindicated due to the risk of perforation .
TREATMENT OF HD ENTEROCOLITIS :
Prompt recognition ESSENTIALRectal tube decompression
Aggressive IV fluid resuscitation
Broad spectrum antibiotics
Vancomycine and metronidazole.
Occasional emergent colostomy.
Can be life-threatening if unrecognized.