TB TransmissionWhat is TB?
TB is a disease caused by infection with a bacteria called Mycobacterium tuberculosis.TB Infection and Disease
The lungs are the most common place for TB. This is known as pulmonary TB.TB of the voice box is the second most common and is usually called laryngeal TB.
TB Infection and DiseaseCan the TB bacteria affect other areas of my body other than the lungs?
TB can infect the brain, kidneys, bones, and other areas.
TB can also spread through the blood to other organs; this is called miliary TB.
TB Infection vs. TB DiseaseThere is a difference between TB “infection” and TB “disease”
TB infection: TB germs stay in your lungs, but they do not multiply or make you sick
You cannot pass TB germs to othersTB disease: TB germs stay in your lungs or move to other parts of your body, multiply, and make you sick
You can pass the TB germs to other people
Natural History of TB Infection
Exposure to TBNo infection
(70-90%)
Infection
(10-30%)
Latent TB
(90%)
Active TB
(10%)
Untreated
Die within 2 yearsSurvive
Treated
Die
Cured

Never develop
Active disease
TB Infection & DiseaseThere are 2 Categories of TB: Latent & Active
TB infection of the lungs can fall into 2 categories of disease: Latent TB or Active TB.Latent TB means a person is infected by TB bacteria, but cannot infect others, and is not coughing or appearing sick.
Latent TB means the body’s immune system has contained the infection.
TB - Infection & Disease Categories of TB - Latent
Persons with latent TB are identified by a positive skin test (PPD).
Persons who are not infected with Mycobacterium tuberculosis have a negative skin test (PPD).
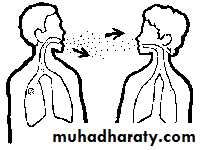
How Are TB Germs Spread?
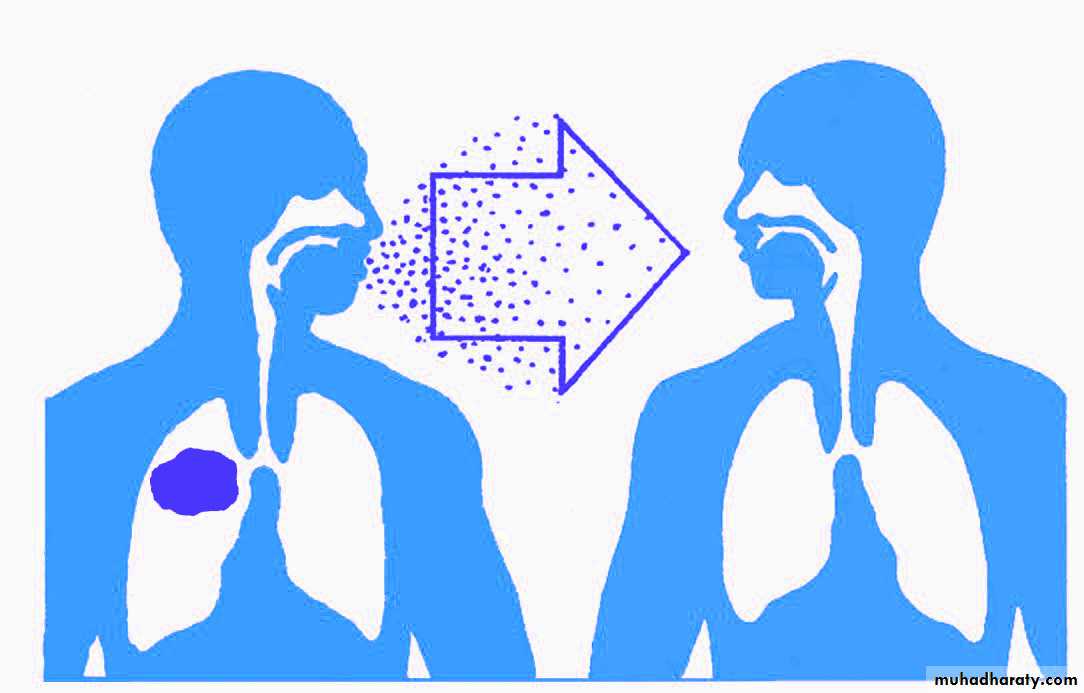
TB TransmissionHow can you catch TB?
TB is spread through tiny drops sprayed into the air when an infected person coughs, sneezes, or speaks, or another person breathes the air into their lungs containing the TB bacteria.Transmission of M.tb
CASECONTACT
Site of TB
CoughBacillary load
Treatment
Closeness and duration of contact
Immune status
Previous infection
Ventilation
Filtration
U.V. light
Environment
Droplet nuclei
Tuberculosis Infection & Disease
Homeless persons are at increased risk for catching TB.
TB cases are rising in the prison population due to the increased number of HIV infected inmates, crowded environment, and IV drug abusers.
Assessing Infectiousness
High degree of infectiousnessSputum smear-positive pulmonary TB
Symptomatic with cough
Cavitation on chest radiograph (correlates with positive smear)
Lesser degree of infectiousness
Sputum smear-negative, culture positive pulmonary TB
Minimal if any cough
Lesser radiographic extent of disease
Extrapulmonary TB
Common Symptoms of TB Disease
Cough (2-3 weeks or more)Coughing up blood
Chest pains
Fever
Night sweats
Feeling weak and tired
Losing weight without trying
Decreased or no appetite
If you have TB outside the lungs, you may have other symptoms
Diagnosis and Treatment for Latent & Active TBTools for Diagnosing TB Infection
Mantoux skin test (PPD)
Chest x-raySputum cultures
Diagnosis and Treatment for Latent & Active TBTools for Diagnosing TB InfectionMantoux Skin Test(PPD)
Mantoux tuberculin skin test (PPD) is a skin test for identifying exposure to the TB bacteria, Mycobacterium tuberculosis (latent infection)
The Mantoux test is recommended because it provides the most consistent and reliable result.
The Mantoux test is read 48-72 hours after administration. Induration or “knot-like” swelling at the test site is significant and the reaction is measured in millimeter units. Redness at the test site is not measured.
Diagnosis and Treatment for Latent & Active TBTools for Diagnosing TB InfectionChest X-Ray
A chest x-ray is ordered when a person presents a recent skin test conversion and is suspected of having TB.
If a chest x-ray is normal, further diagnostic testing may not be necessary.
Diagnosis and Treatment for Latent & Active TBTools for Diagnosing TB InfectionChest X-Ray
If the chest x-ray shows signs of disease, further diagnostic testing will be needed to confirm TB disease.
Diagnosis and Treatment for Latent & Active TBTools for Diagnosing TB InfectionSputum
A sputum specimen is necessary to confirm that the TB bacteria is present in the lung.The sputum specimens should:
-come from deep within the lungs;
-be obtained from the first coughed up sputum of the day, for 3 consecutive days
-may be obtained through special respiratory therapy procedures.
Latent TB vs. Active TB
Latent TB (LTBI) (Goal = prevent future active disease)
= TB Infection
= No Disease
= NOT SICK
= NOT INFECTIOUS
Active TB (Goal = treat to cure, prevent transmission)
= TB Infection which hasprogressed to TB Disease
= SICK (usually)
= INFECTIOUS if PULMONARY (usually)
= NOT INFECTIOUS if not PULMONARY (usually)



Treatment
Most TB is curable, but…Four or more drugs required for the simplest regimen
6-9 or more months of treatment required
Person must be isolated until non-infectious
Directly observed therapy to assure adherence/completion recommended
Side effects and toxicity common
May prolong treatment
May prolong infectiousness
Other medical and psychosocial conditions complicate therapy
TB may be more severe
Drug-drug interactions common
Effect of Therapy on M.tb
Log cfuEffective multi-drug therapy reduces bacillary load
Weeks
0 2 4 6 8 10 12 14 16 18 20 22 24
Evaluating Contacts & Determining Priorities
Priorities in Contact Evaluation• At greatest risk of acquiring infection
• At greatest risk of active TB
• Persons with other immunocompromising conditions or therapies
Initial Assessments of Contacts
Assessment depends on local circumstances,resources, and policies.
Minimal evaluation: Question contacts about symptoms and evaluate if symptoms are present
Tuberculin skin test followed by chest radiographs for all positives (either > 5 mm or > 10mm, depending on local policies)
Chest radiographs for all children < 5 years of age
Sputum examinations for all symptomatic contacts and all with radiographic abnormalities
Children < 5 years of age
Persons with HIV infectionPersons with other immunocompromising conditions
Close contacts of highly infectious index case
Persons with other conditions that increase risk (example: silicosis)
Isoniazid Preventive Therapy: Priorities
Fundamentals of TBInfection Control Practices
Identify persons with active TB early.
Initiate effective and appropriate isolation of known or suspected TB cases.
Initiate effective anti-TB treatment promptly..
.
Fundamentals of TBInfection Control Practices
Identify and evaluate persons and health care workers exposed to infectious TB.Screen health care workers for skin test conversions.
Conduct surveillance for TB cases among patients and healthcare workers.
Patient Education
Patient education is an essential component to prevent the spread of TB.TB patients should be taught to use tissues to cover coughs and sneezes.
Tissues should be disposed appropriately and not left on counter tops.
Patient Education
A surgical mask must be worn by a TB patient whenever they leave the isolation room.Visitors of a TB patient must wear a respirator but are not required to be tested.
Even if a Skin Test is Negative…..
ChicllsFFever
THINK TB!
Chills
Fatigue
Difficulty
in
Breathing
Anorexia
Loss
of Appetite
Night sweats
Coughing
up Blood