بسم الله الرحمن الرحيم
Infectious Diseases
Dr.Kassim Seed IBRAHIM
Department of Pathology
College Of Medicine
University of Mosul
Aim of studying infections
1. Infections are important group of diseases.2.To study these diseases in a scientific way.i e to know the types, eatiology, histogenesis , gross& microscopical apearance of each disease so that you can understand the signs & symptom ,
3, plan therapy, assess prognosis & plan prevention
Infections Diseases
General aspects of infectious diseasesInfection is defined as the invasion of living tissue by m.o. or its products (commensals or pathogenic) followed by local reaction which may be associated with general reaction.
Following invasion, the m.o. may be eliminated without causing obvious disease ( Sub clinical infection ) or clinical disease of any grade of severity.
The outcome depends on the complex balance between the aggressive mechanisms of the m.o. & the defense mechanisms of the host.
** Numerous microorganisms can infect human body some are present normally & harmless called commensals, others cause diseases called pathogens
** commensal microorganisms cause diseases and called at that time opportunistic infections.
Factors influencing the infection:
1- Microorganism factors1. Access: entry of m.o to the body cells & tissues, most m.o.
enter via inhalation, ingestion, sexual .parentral.
2. Dose & virulence: number of m.o entering the body
& their capacity to cause diseases.
3. Invasiveness: ability of m.o to multiply & spread in the body through the use of endotoxin & exotoxin
4. Transmission: ability of m.o to pass to another suitable host.
2-Host Factors:1. Mechanical barriers: Intact skin, keratin, mucous
membrane & their secretary products .
2. Physical Forces: movement of cilia, mucus, flow of urine & saliva. Diarrhea .
3. Chemical: Acidic ph in the stomach which are lethal for many GIT pathogens.
4. Phagocytosis: by macrophages & neutrophils.
5. Immune responce: by cell-mediated &humeral immunity.6. Local factors: e.g. ischemia & foreign body promote infection.
7. Systemic factors: e.g., malnutrition, diabetes mellitus, chronic alcoholism & malignancy.8. Age: both very young & very old have increasing risk of infection.
9. Drugs: appropriate antimicrobial drugs eradicate many susceptible microorganism.Results of infection:
1. Eradication: most infections end by total eradication at the site of entry.2. Persistence of infection: either in form of carrier state or mild chronic forms e.g. typhoid fever, hepatitis infection.
3. Spread: to other parts of the body.e.g. Direct spread as in cellulitis, lymphatic spread as in lymphangitis & lymphadenitis , blood spread as in bactermia, septicemia & pyaemia.
4. Host death: in severe infection e.g. tetanus & diphtheria.
How do infections spread inside the body?
1- Local spread: by the action of lytic enzyme.e.g Streptococci secrete hyaluronidase enzyme which degrades the extra cellular matrix between host cells.2-Lymphatic spread: to the Lymph nodes.
3-Hematogenous spread: causing:-Bacteremia: Presence of m.o in the blood.
-Septicemia: actively multiplying m.o in the blood.
4-Through body fluids: e.g., sexual transmitted disease
(gonococcus).5-Through excretions: e.g., from kidney to lower urinary tract.
6-Through nerves ; e.g. rabies virus, varicella zoster virus.7-Through placental- fetal route.
The common signs of infection
*Depending on the type of M.O and the tissue affected you may have:Cardiovascular manifestations: tachycardia, hypotension, HF.
* Hematological manifestations: leukocytosis, Leukopenia, lymphocytosis, eosinophilia...
* Respiratory manifestations: cough ,hyperventilation, dyspnea, RF.
* Urinary manifestations: proteinuria, oliguria, dysuria, frequency, RF.
* Hepatic manifestations: abnormal liver function test , cholestatic jaundice, nausea, vomiting.
Tissue response ( microsopical ) responses to infections
There are 5 major histological patterns of tissue reaction in infections:
1-Suppurative ( polymorph nuclear ) inflammation characterized by production of pus .
2-Mononuclear & Granulomatous characterized by interstitial inflammation & formation of granuloma
3-Cytopathic- Cytoproliferative inflammation. These reactions are usually produced by viruses.
4-Necrotizing inflammation caused by powerful toxins e.g. Cl. Perfringens lead to gangrene .
5-Chronic inflammation & scarring, is the final common pathway of many infections, e.g. HBV lead to cirrhosis,Schistosomal eggs lead to fibrosis of U.B.wall.
Bacterial infections
Classification of BacteriaBacteria are classified on several criteria:
Gram stain: bacteria are either gram (-) or gram(+)
Shape: bacteria are classified as cocci, bacilli (rods), vibrios, spirochetes.Growth requirements: bacteria are classified as:
AerobicAnaerobic
• Bacteria damage the tissue through several mechanisms,
1- Release toxins that kill cells.(exotoxin&Endotoxin)
2- Release lytic enzymes,
includes proteases,hyaluronidase,coagulase & fibrinolysins that destroy the tissue & facilitate the spread of bacteria
3- Elicit an inflammatory reaction that may destroy not only the bacteria but also the infected tissue.
4-Elicit an immune reaction that may damage the tissues carrying the same antigen as the bacterium (“cross reactivity”).
Bacterial infection is divided into:
1- Acute.2- Chronic.
Acute Bacterial Infection1-Catarrhal .affect mucus membrane,e,g viral infection.
2-Pseudomembranous. Characterized by formation of peudomembrane as in diphtheria.
3-Serous . Affect serous cavities and produce serous fluid
4-Pyogenic or suppurative .Pus producing . e.g. Abscess
.
Suppurative Infection (cont)
Characterised by production of pus
Pus is a creamy fluid consist of neutrophil, pus cell (Dead neutrophil) necrotic tissue, bact, & fluid.
Collection of pus in tuissue is called abscess
M.O secreat IL 1 &TNF which stimulate complement ,This attract neutrophil which secreat lytic enzyme , distroy tissue & form abscess
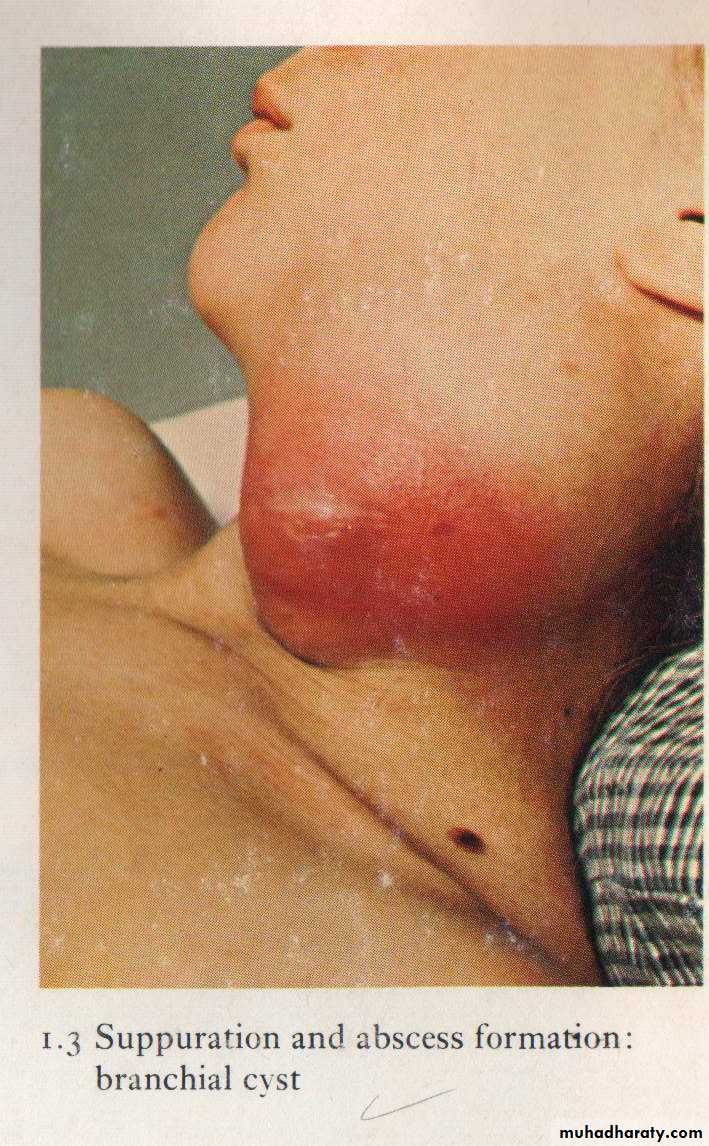
Localization of pus leads to abscess formation which appear here as red congested Swelling at the side of the neck


This is an example of pseudo membranous .

Pseudo membranous colitis
1- Bacterial infection of the blood* Classified into:
-Bacteraemia-Septicaemia
-Pyaemia-Toxaemia : presence of toxin in blood e.g. Diphtheria.
Bacteraemia* Presence of small numbers of bacteria in the blood without multiplication.
* Patients have sub clinical or minor symptoms & lesion.
* E.g., Strept. viridans in blood after vigorous brushing of teeth with dental sepsis.
In typhoid fever ,pneumococcal pneumonia,E.coli infection of urinary tract & brucellosis.* These bacteria are destroyed rapidly in blood because of antibodies, complement, & circulating macrophages.
* It is important because it may settle in various parts of the body & cause localized lesion e.g., endocarditis by Strep. Viridans.
Septicemia
*Multiplication of bacteria in the blood of highly pathogenic bacteria e.g., pyogenic cocci, endotoxin secreting gram –ve bacilli.* Serious infection with profound toxemia in which bacteria have overwhelmed the host defenses.
* It results in serious consequences which may end in death.
Multiple small hemorrhages due to capillary endothelial damage multiple minute metastatic foci of bacterial growth.Tachycardia. Hypotension. Splenomegaly.shock
Pyaemia (pus in the blood)
* Bacteria invade & multiply in a thrombus which then becomes heavily infiltrated by neutrophils & broken down by their digestive enzymes* Small fragments of the soften septic thrombus may then break away & be carried off in the blood
* Results in the developing of pyaemic abscesses in various organs:
Pyaemia (cont)
1-In venous circulation as in deep vein thombosis of legs resulting in pyaemic abscesses in lung.
2-In arterial circulation as in infective endocarditis resulting in pyaemic abscesses in systemic arterial distribution.
3-In portal venous tributary as in acute appendicitis results in portal pyaemia with multiple liver abscess.
Pyaemic abscess consist of:
Central zone of necrosis with huge numbers of bacteria surrounded by zone of acutely inflamed hemorrhagic tissue.
Resulting in multiple & wide spread abscesses.
Gangrene
GangreneDigestion of dead tissue by saprophytic bacteria in living body ( necrosis with putrefaction ) .
Types of gangrene :
Primary
Secondary
The difference lies in the cause of the tissue necrosis of each type.
1) Primary GangreneIt is brought about by infection with pathogenic bacteria which both kill the tissue by secreting potent exotoxins & then invade & digest the dead tissue.
Gas gangrene : the causative m.o. are
Cl. (perfringens ) welchii
Cl. oedematiens
Cl. Septicum
(all are anaerobic ).
These organisms are intestinal commensals in man and animals and because they are anaerobic they can’t multiply in oxygenated environment , so they need dead tissue in dirty wound or lacerated wounds in order to multiply and cause gas gangrene. .
Pathogenesis
Cl. produce different strong types of exotoxins like :1- Lecithinase------causing cell wall damage by lyses of phospholipids .
2- Collagenase &hyaluronidase-----digest extracellular matrix protein and collagen .
Cl. welchii ferments sugar producing H2 & CO2 which collect as bubbles in the dead tissue and can easily be detected by palpation (crepitant ).
These lead to specific changes in the tissue affected by gangrene. On microscopic examination, there is severe myonecrosis, extensive hemolysis & marked vascular injury with thrombosis
Black discoloration and bad odor at the affected site like the skin and subcutaneous tissue , intestine ,appendix and uterus (puerperal period )
Clinical features
Patient looks toxic, there is high fever, acute hemolysis and features of septic shock, which may lead to death of patient if not treated quickly .Gas gangrene of the uterus, note the gas within the necrotic tissue produced by clostridia species.
2) Secondary Gangrene
This type of gangrene is characterized by necrosis due to some other causes, usually loss of blood supply from vascular obstruction or tissue laceration &saprophytic bacteria then digest the dead tissue.Types of secondary gangrene
1) Wet gangrene :
The infected tissues are edematous due to presence of large amount of fluid and large amount of subcutaneous fat . This type occurs rapidly . The line of demarcation between dead and living tissue is indistinct. The gangrene may extend proximally beyond the site of infective.
Wet gangrene –D.M.
2) Dry gangrene :This type occurs in leg due to gradual cut of blood supply either due to atherosclerosis or vasculitis in the lower limbs. The line of demarcation between dead and living tissue is clear .
The lesion remains localized .
Blackish discoloration of the finger- dry gangrene
Chronic Bacterial infectionTuberculosis
* Caused by Mycobacterium tuberculosis & Mmycobacterium bovis.Gm +ve bacilli* It infects about 1.7 billion individuals world wide & kills about 1.7 million patients each year & so is the single most important infectious cause of death on earth after HIV.
* Because mycobacterium grows 20-100 times slower than other bacteria it takes 4-6 weeks to obtain a colony of mycobacterium tuberculosis.
Transmission
Four possible entry sites exist: -
(1) Respiratory tract by inhalation ,from open TB lesion.
(2) Alimentary tract by ingestion of infected milk ,food.
(3) Skin by inoculation.
(4) Congenital infection followed by intrauterine through placenta (it is very rare).
Tissue Reaction to T.B. bacilli
T.B. at first cause minimal inflammatory response in the tissue at the site of infectionSpecifically primed T-Lymphocytes appear at the site of infection within two weeks and secreat lymphokines
Lymphokines responsible for type IV hypersensitivity reaction.
Arrival of macrophages by chemo taxis.
Arrest of macrophages by migratinn inhibition factor.
Transformation of the macrophages into epitheliod cells by macrophage activating factor.
Destruction of phagocytes contain T.B. bacilli by macrophages arming factor.
Gaseous necrosis by T- cell cytotoxic factors.
Tissue reaction (cont)
*So the final lesion of TB consist of central area of amorphous, a cellular caseous necrosis , surrounded by macrophages, referred to as epithelioid cells, some macrophages fuse to from multinucleated giant cells, the nuclei of which may be distributed peripherally ( Langhans giant cells) these are surrounded by rim of chronic inflammatory cells rich in lymphocytes & at the periphery there is fibrosis.
This lesion is called tubercle which is the characteristic lesion of TB.
It usually affects the lungs but may involve any organ or tissue in the body.

Tissue reaction ( cont)
The caseous materials may be infiltrated by heavy neutrophilis result in cold abscess. It is called that because there are no signs of acute inflammation (hotness, redness, …..etc)* Healing when present is by progressive fibrosis.
* Organisms may remain viable in apparently healed lesions only to be reactivated years later if host resistance decreases.Spread
Organisms may spread from the site of entry in the usual ways:Locally: into adjacent tissues
lymphatic to regional lymph nodesNatural passages e.g. (respiratory, alimentary, urinary & genital tract.)
Blood veins & arteries) to produce either:
1- Miliary tuberculosis with multiple tubercles in numerous organs & tissues.
2- Isolated metastatic organ lesions e.g., in kidney, bone, vertebra, joint &epididymis.

Immunology
TB bacilli Produce no Exotoxin or Endotoxin .The Lesion of T.B is mainly due to the delayed hypersensitivity reaction type IV to an antigenic protein component of the organism (e.g cord factor, Sulfatides &LAM polysacharides).
This immunity provide the basis for skin test of T.B
Immunity to T.B. can be induced artificially by intra dermal injection of attenuated mycobacterial strains of bovine type (e.g. BCG vaccine).Skin test in TB ( Mantoux test ) Tuberculin test
It is an intradermal injection of tuberculoprotein . The test become positive in about 2-4 weeks after infection by T.B.bacilliA positive skin test appear within 12-24 hours & peaks in 48- 72 hours after intradermal injection of tuberculoprotein as a firm indurated nodule with surrounding redness.
A positive result indicate hypersensitivity to T.B. (i.e.recent or old infection)
Mantoux test
Primary tuberculosis
* It follows initial exposure to TB bacilli in non immunized individuals of any age.* Macroscopical: it forms a small sub pleural parenchymal lesion in the mid zone of the lung (Ghon focus) and spread to the hilar lymph nodes. Both lesions are called Primary complex
* Microscopical: consist of epitheloid granuloma with central caseous necrosis.
*Most of the cases (95%) after treatment heal by fibrosis some may enter into dormant state &few may spread into the body forming progressive primary T.B.
Ghon focus of primary T.B.

Secondary T.B.
* Either occurs as a reinfection by mycobacterium tuberculous or reactivation of primary infection when there is impairment in the immunity of the patient.* Macroscopical: usually occurs at the apex of the lung with minimal lymph node involvement. There is marked damage in the lung parenchyma with cavity formation
* Microscopical: pitheloid granulomatous with central caseous necrosis & cavity.
* Healing by fibrosis or may spread forming progressive secondary T.B.

Cavitations of secondary T.B
Progressive T.B.* Either from primary or secondary T.B.
* T.B. bacilli can be coughed into the larynx forming laryngeal T.B.
* or swallowed into the G.I.T causing intestinal T.B.
* or enter through bronchial tree leading to tuberculous bronchopneumonia or spread into the pleural cavity leading to pleural effusion.
* or enter through the lymphatic channel or blood stream causing Miliary T.B. or isolated organ T.B.
The natural history of tuberculosis
Clinical FeaturesFever
Weight loss
Night sweating
Cough
Heamoptysis
Diagnosis
I- History.
II- Clinical Examination.
III- Investigation include : X- ray, detection of the m.o in the specimen (sputum. urine, in biopsy) by the use of Ziehl-Neelsen staining ,culture or guinea pig inoculation.
Biopsy of the infected tissue.
PCR amplification of T.B. bacilli DNA allows for even more rapid diagnosis.* Positive skin test (Mantoux) indicates hypersensitivity to tuberculoprotein but not an active disease.
.
This is an acid fast stain of Mycobacterium tuberculosis (MTB). Note the red rods--hence the terminology for MTB in histological sections or smears: acid fast bacilli.

Treatment
Adequate & appropriate antituberculous drugs used for months.LEPROSY
(Hansen ,S Disease)
Eatiology and mode of infection
Leprosy is caused by mycobacterium lepraeInfection require long period of close contact with patients.
Mode of infection is not clear probably by inhalation.
Spread by blood stream localise in periferal nerves
Pathogenesis of leprosy
Lepra bacilli produce no exotoxin or endotoxin the lesion is produced by :By distructive granuloma
By interferance with metabolism of schwann cells
Coarse of the disease
Most of the pateint get rid of the bacilli by natural resistanceIndeterminate leprosy : the bacilli multiply in the dermal nerves produce hyposensitive macule
Tuberculoid leprosy : develop in pateint with high cell mediated immunity, The lesion consist of asymetrical anasthetic macule and palpable thickened nerve,deformity & ulceration
Borderline leprosy: In between lepromatous and tuberculoid leprosy
Coarse of leprosy (cont)
Lepromatous leprosy: Nodular type develop in patients with low immunity. The lesion consist of symetrical nodules of the skin , thickening of skin & nerves, (leonin face), deformity & ulceration
Involvment of eye, larynx , testis etc
Amyloidosis may complicate lepromatous leprosy
Microscopically:The skin and nerve infiltrated by macrophages full of lepra bacilli, Lymphocytes are few,No granuloma
.

Microscopically:Tuberculoid leprosy Non caseating epitheloid granuloma
Lymphocytes, Bacilli are scanty

Diagnosis of leprosy
History of contact with pateintExamination: Anasthesia, deformity ulceration
Lepromin skin test: Intradermal injection of heat killed L-bacilli gives in 4 Wks nodule in tuberculoid leprosy and indeterminate leprosy
Finding lepra bacilli
Demonstration of Lepra bacilli
Slit skin testNasal swab
Biopsy
Modefied Zeihl neelsen stain on these sample show lepra bacilli

Actinomycosis
Actinomycosis* Caused by Actinomyces israellii
* Virtually anaerobic, gram-positive, long filamentous bacteria.
* Closely related to mycobacteria with some similarity to fungi.It can be found as a commensal m.o. in the mouth , G.I.T., female genital tract. Only occasionally they invade the tissues it produce infection.
1- Cervicofacial lesion (70%).
2- Abdomial lesion (around iliocecal region or appendix) (15% ).3- Pulmonary lesion (10%).
4- Subcutaneous lesion (5%).
5- Gynecological infection in female with IUCD.
Pathology:
Infection produces firm masses containing numerous abscesses ( honeycomb abscesses) bearing colonies as yellowish granules (sulfur granules) with sinuses & fistulae.Histology:
Chronic granulomatous inflammation with suppuration, bacterial colonies, granulation tissue & thick walled capsule & septae.
Diagnosis:
Yellow granules, gram stain (+Ve), PAS (+Ve).Treatment: -
Antibiotic +/- surgical.

Actinomycosis is a chronic granulomatous bacterial infection
Note the colony of the micro organism floats in a pool of pusThe colony of actinomycosis at high magnification.The micro organism is filamentous & the filaments project
as red specular deposits at the periphery of the colony which is surrounded by neutrophils (mycetoma).
Spirochetes
Spirochetes* Are activity motile, Gram negative, coiled, unicellular spiral shaped m.o.
* Produce usually interstitial chronic inflammation with perivascular plasma cell & lymphocytic aggregates.
Syphilis
* Caused by spirochete treponema pallidum. It is a chronic venereal disease with multiple clinical presentations.Transmission:
It needs close physical sexual contact for transmission.It penetrates the mucosa through a minor or microscopic abrasion.
There is transplacental transmission .

Stage of the disease
Primary syphilis: -* Lesion (chancre) develops few days or approximately 3 weeks after infection on the glans penis or vulva (90%), anus, lips, fingers & breast in (10%).
* Chancre is a solitary, slowly enlarging, hard, painless nodule with superficial ulceration associated with enlarged regional lymph nodes.
* Healing occurs in 3-6 weeks either spontaneously or after treatment.
Secondary syphilis: -
Usually develops 1-3 months after infection. It is due to spread & proliferation of the spirochetes within the skin & mucocutaneous tissues.
Secondary syphilis occurs in approximately 75%of untreated patients.
* Lesions appear as flat or slightly elevated papules on external genitalia called condylomata lata , generalized macular skin rash, shallow buccal , lingual & pharyngeal ulceration , and generalized lymphadenophathy.
* Healing may occur spontaneously or after treatment.
* Some cases progress to tertiary syphilis.
Tertiary syphilis: -
* It appears several years after primary infection (5-30) years.
* Tertiary syphilis has 3 main manifestations:
1-CVS syphilis : ( aortic aneurysmal dilatation , aortic incompetence , aortic regurgitation & coronary ostial narrowing).
2-CNS neurosyphilis : (meningovascular disease, general paralysis , tabes dorsalis ,dementia & personality changes).
3-Gumma: formation (firm, rubbery, multiple, nodular masses) most commonly found in the liver (hepar lobatum) ,bones & testes.
Gumma are now very rare because of the use of the effective antibiotics.
* These may occur alone or in combinations.
Histology of gumma:Granuloma with central coagulative necrosis surrounded by granulation tissue containing numerous chronic inflammatory cells rich in plasma cells with end arteritis obliterans & periarteritis.
The endarteritis , which is seen in all stages of syphilis, starts with endothelial hypertrophy & proliferation followed by intimal fibrosis.
The regional L.N. are usually enlarged & may show non specific acute or chronic lymphadenitis, plasma cells infiltration, or focal epitheliod granuloma.
Treatment:
By adequate antibiotic ( penicillin).

Congenital syphilis
* It is due to transplacental spread, which occurs most frequently during primary & secondary syphilis, when the spirochetes are most numerous.* May cause:
1- Stillbirth, neonatal death or disease present in infancy, childhood or even adult life.
2- Desquamating skin rash, particularly of the hands , feet , around the mouth & anus.
3- Osteochondritis (saddle deformity of the nose).
4- Epiphysitis (irregular ossification & bone deformities).
5- Diffuse hepatic fibrosis &interstitial pulmonary fibrosis.6- Characteristic deformity of the incisor teeth, which is peg-shaped with notched edges (Hutchinson’s teeth) with pitting of the first permanent molars.
7- Later interstitial keratitis produce corneal opacity & blindness.
Diagnosis of syphilis:-
I- History. II- Clinical examinationIII- Investigations include two types of serologcal tests: non-treponemal a.b. test & anti treponema a.b. test:
1) VDRL (venereal disease research laboratory) test.
2) FTA-ABS (Fluorescent treponemal antibody absorption)Test.
Smear from the ulcer or discharge
To demonstrate the spirochetes by:1- Silver stains e.g. Warthin- Starry stain.
2-Dark- Field Examination.3-Immunofluorecence technique.
PCR test for syphilis.
Long, spiraling spirochetes are seen with a Warthin-Starry silver stain.

Viral Infections
Viral infectionViruses are relatively simple, small, obligatory intracellular parasite which replicates within cells by synthesis and assembly of separate components.
Viruses are classified by their nucleic acid genomes into
DNA virusesRNA viruses .
Routs of infection
Inhalation ;e.g influenza virusesIngestion : polio viruses
Parentral : AIDs,
Mechanisms of viral injury
1- Inhibits host cell DNA, RNA or protein synthesis e.g. Poliovirus.2- Direct cell killing by damaging host cell membrane or DNA e.g. Rhinoviruses.
3- Induce Immune reaction e.g type III &VI hypersensitivity reaction in resp cyncytial viruses, arbovirus encephalitis.Mechanism of viral injury (cont)
4- Damage host defence mechansm e.g. respiratory epithelium predisposes to the pneumonia by Staph. Pneumoniae &Haemophilus influenza. Immune system in AID
5-Induce cell proliferation & transformation result in neoplasia e.g. HBV, EBV.
Microscopical picture of viral infection
Mononuclear infiltrationTissue necrosis
Giant cell formation
Inclusion body formation.(intranuclear or intracytoplasmic)
Viral inclusion bodies
viral particles aggregate within the cells they infect & form characteristic ( Inclusion bodies)nuclear inclusion surrounded by a clear halo as in Herpes virus
cytoplasmic inclusions as in small pox and rabies virusMany V. do not give rise to inclusions e.g. EBV.
This is cytomegalovirus (CMV) infection in the lung. Note the very large cells that have large violet intranuclear inclusions with a small clear halo. Basophilic stippling can be seen in the cytoplasm.

Lymphocytosis
Production of interferonProduction of neutralizing antibody
Cell mediated immunity plays a role in controling viral infection
Body response to viral infection
Types of viral infection
AbortedLattent : Virus is synthesised continously without altered cell e.g.HBV
Persistant: Integrated in the cells Reactivated with depressed immunity
Slow viral infection take very long incubation period as in cruetz feldt jacob disease