Fifth stage
Ophthalmologyعملي
2017/4/16
1-Congenital failure of canalization of right nasolacrimal ductWhat is the presentation of this child? Lacrimation on right side(epiphora) or conjunctivitis
What is the proper management?
1-reassurance of parents
2-topical AB with massage till the end of the 6months
3-if not opend (after 6months, most open spontaneously during the 6months) probing and irrigation with antiseptic solution
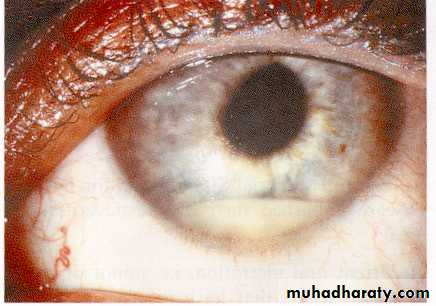
2-Ptergyium
Describe this lesion: Localized redness located at nasal corner of the eye, triangular in shape with the apex extend to involve cornea due to fibrovascular ingrowths ((patchy redness with fleshy lesion reach the limbus ))
Causes?
Causes of patchy redness1-subconjectival hemorrhage 2- nodular episcleritis 3-nodular scleritis
Causes of fleshy mass on limbus conjectival navus 2-papilloma 3-SCC
What are the indications of surgery in this patient?
1-affect visual axis. 2-severe discomfort. 3- cosmetic.
4- poor vision. 5- dryness of cornea. 6-astigmatism.
DDX1-pinecula 2-episcleritis 3-secleritis
3-Subconjuctival hemorrhage (spontaneous or traumatic)
Homogenous redness (patchy haemmorage )
What will you ask in the Hx? 1-history of trauma, straining conditions (vomiting, constipation, cough)
2-history of hypertension. 3-bleeding tendency.
4-history of drugs: anticoagulants and NSAIDs, aspirin
Management: assurance of patient, resolved after 10- 14 days, it is simple condition put if the patient want treatment you can give artificial tear or lubricants.
4- Membranous conjunctivitis,, purulent discharge
What are the possible causes?
1-true membrane(remove cause bleeding): diphtheria ,steven jonson syn
2-pseudomembrane(remove without bleeding): most bacteria like staph + adenoviral infection.
NOTE :discharge :mucous allergy, watery viral, purulentbacterial mucopurulant clamedia
5-Facial palsy on R. side with lagophthalmos & Bell's phenomenon (LMNL)
^canot close her eyes –lage opthalmus-paralytic ectroption ^

Presentation: Mouth deviated to the left side, cannot close right eye, eye pulled upward (bell's phenomina).
Significance? Exposure keratopathy
How do you treat the eye of this patient?
1-artificial tears in days
2-closure of eye at sleep (taping)
3-If chronic do surgery (lateral tarsorraphy)
4-shield glasses
Complication :ectropion ,,dryness of eye
6-What is this sign? Papillae on the inner surface of upper lid (giant cobblestones papillae)
What are its causes? 1-vernal keratoconjunctivitis, 2-allergic conjunctivitis: atopic, seasonal, giant papillary conjunctivitis.3-contact lenses 4-retention of suture material
Treatment:
Avoiding exposure to the causative allergen, topical steroids, mast cell stabilizers, antihistamine, dark glasses & cold compresses.
7-
Corneal topography(name of test )
Color coded map used for studying the shape, curvature, refractive power of cornea(thikness) in every point with details.
Use for early dx of ceratoconous ,use jest prior to refractive surgery
Staphyloma
-Occur in high myopia as the globe is large.
-Thinning of retina, bulging, exposed sclera.
-chorioretinal attenuation pathological myopia
US in high myopia
B-scan of eye posterior bulging with axial myopia
8-
Leukocoria & pseudosquint
Describe the lesion? Right white opacity in RT pupil.
Enumerate the most common causes according to their frequency?
1-congenital cataract.
2-retinoplastoma.
3-retinal fibrosis.
4-persistent hyperplastic primary vitreous.
5-retinopathy of prematurity.
Cause of pseudosquint: Epicanthal fold.
9-Methods of tonometry
slit lamp measure of IOPother method of tonometersperkins tonometer *electrical indentation *impression tonometer
#Goldmans applanation
tonometryPut florescence stain to the tear film then press the external surface of eye by the tonometer and when it become flat it means equalization of the pressure inside and outside the eye, and the semi-circles will meet each other, so take this point as IOP.
Schiotz tonometry
There are 3 things here:
1- Weight (g).
2- Degree of corneal indentation (mm).
3- Table of pressure measurement.
Pressure reversely related with the indentation
10-
By using which test we can get this view?
1- Gonioscopy (visualization of the angle of the anterior chamber = irido-corneal angle)
2- With goniolens (for detecting glaucoma).
Describe the aqueous circulation:
It is produced by the ciliary process of ciliary body >posterior chamber >pupil> anterior chamber >trabecular meshwork> Canal of Schlemm>episcleral venous plexus ciliary vien opthalmic vien SVC
11-Measurement of AC depth
Comment on the AC depth: Shallow anterior chamber depth.
If this patient is asymptomatic, how you treat him?
Treat even if asymptomatic
1-Medical Tx: mitotic agents ,alpha agonist, b-blocker, carbone anhydrase inhibitor, prostaglandin analogs
2-peripheral laser iridotomy (YAG laser)
*it consider pre-glaucoma so it is urgent.
3- hypermetropia: convex lenses.
4- Treatment of glaucoma: pylocarpin, iridotomy
12-
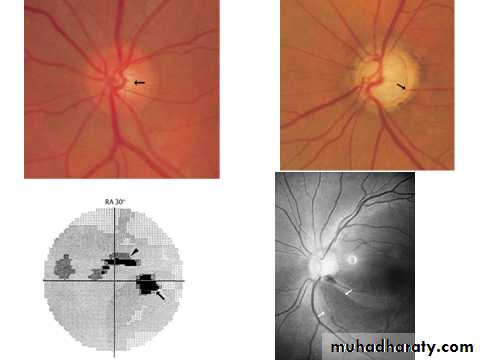
Abnormal cupping of the optic disk (CD ratio > 0.3)
Normal cup:disk ratio 0.3 – 0.4
If CD ratio increase it means there is large cup.
Cause: primary open angle glaucoma
Criteria of cupping:
1-cup:disk ratio > 0.3.
2-progressive enlargement
3- asymmetrical between the two eyes.
Criteria to diagnose glaucoma:
1) Increased IOP. Normally 15±6 mmHg.
2) Abnormal cupping.
3) Changes in visual field.
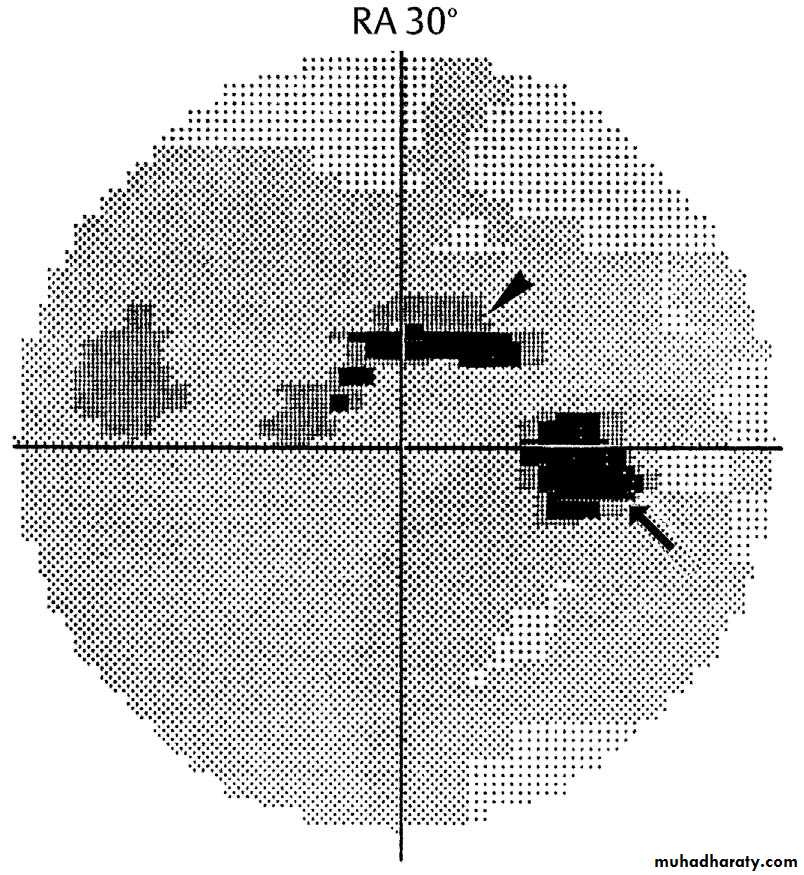
12-lower right
Automated static perimetry (visual filed)
perimetry graph showing paracentral scotoma in open angle glaucoma
-No patient complain
-Diagnosed by chance
Upper paracentral arcate scotoma
13-RT :upper black spot act as laser iridotomy
Peripheral laser iridotomy
Indication:
Shallow anterior chamber (angle closure glaucoma) so we do it to make direct shunt between anterior and posterior chambers.
13-LT
Dx: Red congested eye (acute angle closure glaucoma) with corneal edema, ciliary flash and dilated pupil.Features:
Painful red eye.
Achy, abdominal pain.
Misty vision.
Go from light into dark.
Small eye, shallow anterior chamber.
Pupil mild dilated.
Iris lens contact.
Push the iris forward.
Eye feels hard.
هذي الحاله تصير اذا ما عملنا iridoctomy
14-
Measuring corneal diameter by caliber
Why?
To detect and follow up congenital glaucoma ( buphthalmos)
Rx: goniotomy ,trabiclotomy

15-
16-
Describe this corneal lesion: Dendritic corneal lesion
What is the most likely diagnosis? HSV type 1
How would you treat? Antiviral drugs (acyclovir , topical
trifluoridine and idoxuridine) // avoid steroids.
DDX:1HS 2healing corneal abrasion
17-
subhyaloid hemorrhage Hemorrhage between retina & vitreous
Level of heamorrhage in the retina according to the shape1-اذا كل الصورة حمراء وماتبين ال retinal hazy --< this vitrous
2-اذا level boot shaped --< subhyaloid hemorrhageالنزف تحت الزجاجية
3-fethary appearance --<Crvo
18-
19-
Central retinal venous occlusion (CRVO)
Congested dilated blood vessels.
History (ask about):
Hypertension, hyperlipidemia, DM, smoking, obesity, life style, psychological problems, stress.
Causes:
1) Extraluminal causes: hypertension & tumor.
2) In the wall: vasculitis.
3) Intraluminal: thrombus.
Complications:
1) Neovascular glaucoma.
2) Chronic macular edema.
مثل الفرشه وعدلطخ فوقه
Central retinal arterial occlusion (CRAO)
Attenuation & constriction of the arteries (cattle track appearance), the whole retina is pale except the fovea (cherry red spot) due to double blood supply.
Causes: Usually embolic.
History: ask same questions in venous occlusion.
Could lead to neovascular glaucoma (due to occlusion of iris root by new vessels).
DDx For cherry red spot:
-Commotio retinae
-Quinine poisoning
-Macular hole surrounded by RD
-Amauratic family idiocy
20-
21-
22-
23-
Retinitis pigmentosaBone spicules, waxy disc & attenuated blood vessels.
Patient complains:
1-night blindness (nyctalopia).
2-visual loss
3-seeing flashes of light (photopsia).
Mention 2 syndromes associated with it.
1-bardet biedl syndrome
2-refsum syndrome
3- Autosomal dominant / recessive
24-
25-مكرر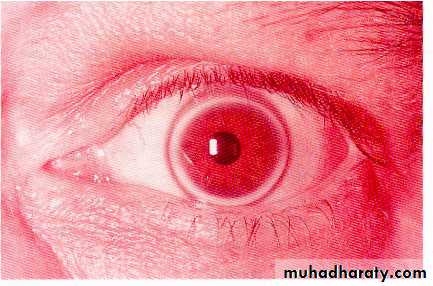
26-
Corneal arcus (lipidis) or arcus senilis
What is the clinical significance? It indicate hyperlipidemia in young people which may causes systemic diseases.
What is the visual prognosis? It never affect vision(never reach cornea)
27-
Lower lt \\\Hypopium
It is pus in the anterior chamber
Causes:
1- Infected: endophthalmitis (pneumococcus).
2- Sterile: severe iritis.
3- keratitis.
4-any inflammation or infection

Lower rt \\
Filamentray keratitis
Stain: rose bengal stain
Causes : 1-dry eye 2-sjogren syndrome
3- facial palsy 4-blepharoptosis
Presentation: patient with dry eye and the mucin become thick and adhere to the cornea and give sensation of F.B.

Upper rt
Ameboid ulcer
Cause:
Mistreatment of dendritic ulcer by steroid.
Upper lt

Episcleritis
Symptoms/Signs: Often asymptomatic, Mild tearing/ irritation, Tender to touch, Self-limiting (may last for months).Treatment: Lubricants, NSAIDS, Rarely low dose steroids.
28-
Describe this lesion?
Nodulo-ulcerative lesion Oval, elevated, ulcerated, congested, dirty lesion on the lower lid with telengectasia on the surface
Differential diagnosis?
1-basal cell carcinoma(most)
2-sequamous cell carcinoma
3-sebaeous cell carcinoma
4-keratoacanthoma
5-malignant melanoma
29-
Chalazion DDX :lipoma,dermoid cyst
Describe this lesion Localized swelling in the upper lid with normal skin over it
Enumerate four causes
1-chalazion 2-stye 3-sebaceous cell carcinoma
4-haemangioma 5-blockage of tarsal glands
6-Seborrhea 7-Chronic blepharitis 8-Acne rosacea.
How would you treat it?
1-conservative: massage, hot compress, AB ointment, local steroid.
2-surgery: surgical incision and curettage of the gland.
30-
Ectropion of the right lower lid(outward eversion of eye lid)What is the complaint of this patient?
Lacrimation due to poor drainage , congested red conjunctiva, repeated infections, painful lid margin .
What are the possible causes?
1-aging 2-congenital 3-lower lid scar 4-faiacl palsy 5-neurofibromas 6- mechanical cause
31-
Entropion of the lower lid with trichiasis
What are the possible causes?
1-aging
2-congenital
3-palpebral conjunctival scaring
4- trachoma, trauma, infection, inflammation
ملاحظة :
32-
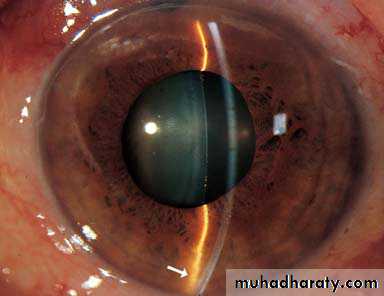
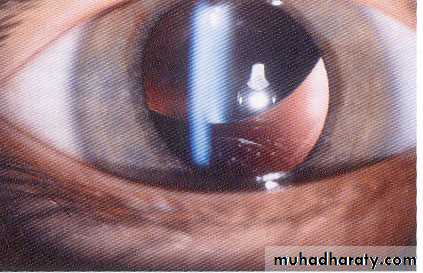
Lens dislocation (ectopic lens)What are the possible visual symptoms? Blurred vision and diplopia and refractive errors.
Enumerate three possible systemic causes:
1-trauma
2-marfan syndrome
3-homocystinuria
4-high myopia (eye problem)
5-ehler danlose

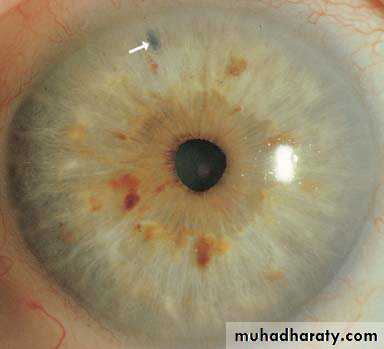
33-
Keratic precipitate (white dots in cornea)
What is your diagnosis? It is a feature of iritis or anterior uveitis
What do you think the presentation of this patient?
Blurred vision, photophobia, pain, redness, and lacrimation.
Treatment:
1- topical: atropin sulphate and corticosteroid
2- systemic: steroids (severe cases) or AB (infected cases)

34-
Herpes zoster ophthalmicus
Describe the skin lesion:
Erythematous base lesion with crust, pastule and some sloughing involving forehead and side of the nose and upper + lower lid of lift eye.
Describe the ocular lesion:
FLOURESCEIN stain showing corneal ulcer of left eye+ skin lesion involve upper + lower lid.
ملاحظة :
35-
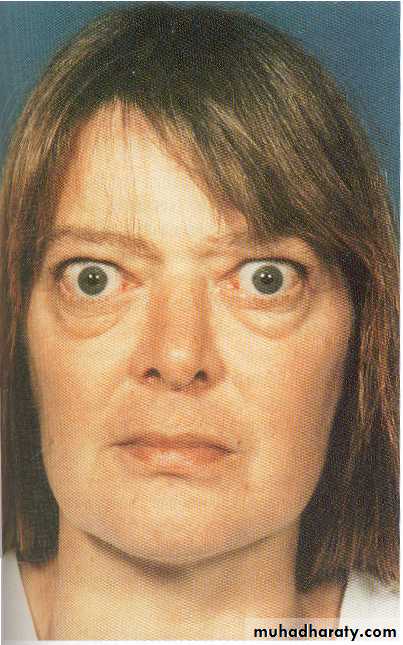
Thyrotoxicosis
Describe this facies:
Staring facies with periorbital edema
Enumerate four ocular features of this disease:
1-lid lag
2-lid retraction
3-exophthalmos
4-excessive lacrimation
5-Chemosis.
6-Periorbital soft tissue changes as chemosis & lid swelling.
7-Exposure keratopathy.
8-Ophthalmoplegia.
9-optic neuropathy
-proptosis
-st changes
-periorbital edema
-opthalmoplagia
Enumerate four systemic features of this disease:
1-sweating 2-palpitation 3-tremor 4-tachycardia
5- Goitre 6- Increased appetite with loss of weight
36-
What is this procedure? Eversion of upper lid
What are its benefits?look for sign that are otherwise hidden
1-very simple
2-F.B. detection
3-papillae detection
4-follicular reaction detection
5- Arlet line of trachoma.
6- Giant papillary conjunctivitis.
7- Adrenochrome deposits.
8- Melanoma.
9- Conjunctival concretion
10-concretion
11-lost contact lens
12-scar
13-chalazation
37-
What is this procedure?
• Cover/uncover test
In which disease you want to use it in your examination?
• Used to detect inapparent squint (phoria)
#70%have latent sequnt
38-
Left complete ptosis
What are the possible causes?
1- 3rd palsy 2-congenital 3-birth injury 4-horner syndrome
Would you go for surgery for this child? Yes, to avoid amblyopia or reduction of visual acuity and here we do sling procedure.
39-
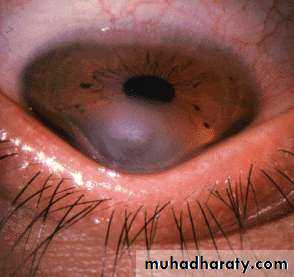
Munson sign
Describe what you see: This patient asked to look down, lower lid is seen pushed by cornea due to increased corneal curvature with opacity.
What is the disease? Keratoconus with acute hydrops
Significance: It is one of the common causes of reduction in visual acuity (myopia & Astigmatism).
Diagnosis of keratoconus:
1-Ask the patient to look down.
2-Placido disc.
3-Corneal topography (green normal, blue depression, red elevation).
4-Keratometry (give the reading in diopter).
What are the lines of treatment for this case?
1-contact lens or patching
2-hypertonic drops to cause withdrawal of hydrops
3-corneal graft
40-
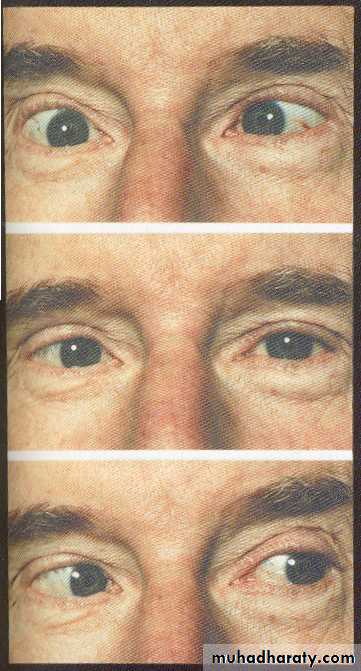
Is it a concomitant or incomitant squint? incomitant
• Which muscle is affected? Right lateral rectus
• What is the nerve supply? Abducent nerve
• concomitant: angle of squint not changed in different visual directions
• incomitant: angle changed
jjj