Fifth stage
GynecologyLec-
9/5/2017
Pelvic organ prolapseDefinition:
A prolapse is a protrusion of an organ or structure beyond its normal confines.Prolapsesare classified according to their location and theorgans contained within them.
Classification:
Anterior vaginal wall prolapse• Urethrocele: urethral descent
• Cystocele: bladder descent
• Cystourethrocele: descent of bladder and urethra
Posterior vaginal wall prolapse
• Rectocele: rectal descent
• Enterocele: small bowel descent
Apical vaginal prolapse
• Uterovaginal: uterine descent with inversion of vaginalapex
• Vault: post-hysterectomy inversion of vaginal apex
Prevalence:
Pelvic organ prolapse is a very common problem with a prevalence of 41–50 per cent of women over the ageof 40 years.
There is a lifetime risk of 7 per cent ofhaving an operation for prolapse and a lifetime risk of11 per cent of having an operation for incontinenceor prolapse.
The annual incidence of surgery for POPis within the range of 15–49 cases per 10 000 womenyears, and it is likely to double in the next 30 years.
Grading:
Three degrees of prolapse are described and the lowestor most dependent portion of the prolapse is assessedwhile the patient is straining:• 1st: descent within the vagina
• 2nd: descent to the introitus• 3rd: descent outside the introitus.
In the case of uterovaginal prolapse, the mostdependent portion of the prolapse is the cervix, andcareful examination can differentiate uterovaginaldescent from a long cervix. Third-degree uterineprolapse is termed ‘procidentia’ and is usuallyaccompanied by cystourethrocele and rectocele.
Aetiology:
The connective tissue, levator ani and intact nervesupply are vital for the maintenance of position of thepelvic structures, and are influenced by pregnancy,childbirth and ageing. Whether congenital oracquired, connective tissue defects appear to beimportant in the aetiology of prolapse and urinarystress incontinence.Congenital
Two per cent of symptomatic prolapse occurs innulliparous women, implying that there may be acongenital weakness of connective tissue. In addition,genital prolapse is rare in Afro-Caribbean women,suggesting that genetic differences exist.Childbirth and raised intra-abdominal pressure
The single major factor leading to the development ofgenital prolapse appears to be vaginal delivery. Studiesof the levator ani and fascia have shown evidenceof nerve and mechanical damage in women withprolapse, compared to those without, occurring as aresult of vaginal delivery.Parity is associated with increasing prolapse. TheWorld Health Organization (WHO) PopulationReport (1984) suggested that prolapse was up toseven times more common in women who hadmore than seven children compared to those whohad one. Prolapse occurring during pregnancy israre, but is thought to be mediated by the effects ofprogesterone and relaxin. In addition, the increasein intra-abdominal pressure will put an added strainon the pelvic floor and a raised intra-abdominalpressure outside pregnancy (e.g. chronic cough orconstipation) is also a risk factor.
Ageing
The process of ageing can result in loss of collagen andweakness of fascia and connective tissue. These effectsare noted particularly during the post-menopause asa consequence of oestrogen deficiency.
Postoperative
Poor attention to vaginal vault support at the time ofhysterectomy leads to vault prolapse in approximately1 per cent of cases. Mechanical displacement as a resultof gynaecological surgery, such as colposuspension,may lead to the development of a rectocele orenterocele.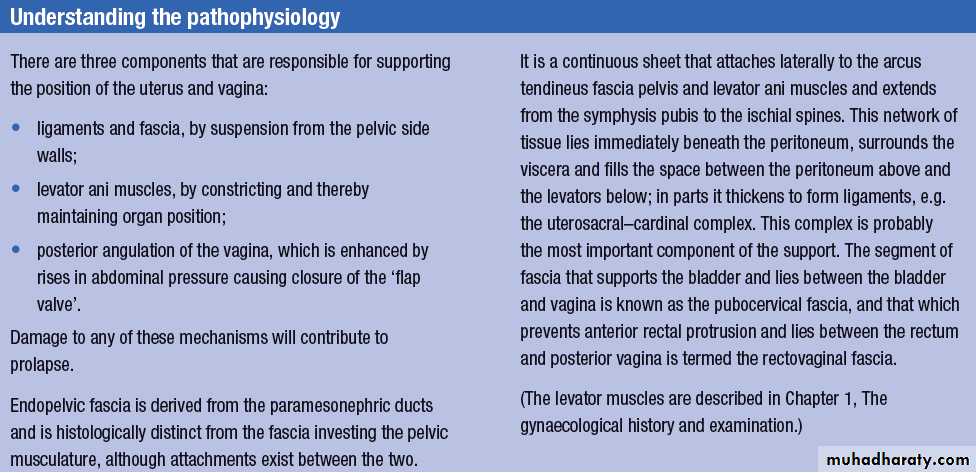
History:
Women usually present with non-specific symptoms.Specific symptoms may help to determine the typeof prolapse. Aetiological factors should be enquiredabout.
Abdominal examination should be performed toexclude organomegaly or abdominopelvic mass.
Symptoms:
Non-specific:Lump, local discomfort, backache, bleeding/infection if ulcerated, dyspareunia or apareunia.
Rarely, inextremely severe cystourethrocele, uterovaginal or vaultprolapse, renal failure may occur as a result of ureterickinking.
Specific:
Cystourethrocele urinary frequency and urgency,voiding difficulty, urinary tract infection, stress incontinence.
Rectocele incomplete bowel emptying, digitation,splinting, passive anal incontinence.
Vaginal examination:
Prolapse may be obvious when examining the patientin the dorsal position if it protrudes beyond theintroitus; ulceration and/or atrophy may be apparent.
Vaginal pelvic examination should be performedand pelvic mass excluded.
The anterior and posterior vaginal walls andcervical descent should be assessed with the patientstraining in the left lateral position, using a Simsspeculum.
Combined rectal and vaginal digitalexamination can be an aid to differentiate rectocelefrom enterocele
Investigations:
There are no essential investigations. If urinary symptoms are present, urine microscopy, cystometry and cystoscopy should be considered.The relationship between urinary symptoms and prolapse is complex.
Some women with cystourethrocele have concurrent incontinence; as the prolapse increases in severity, urethral kinking may restore continence but lead to voiding difficulty.
Should renal failure be suspected, serum urea and creatinine should be evaluated and renal ultrasound performed.
For women with symptoms of obstructed defaecation MR proctography can help diagnose a rectocele.
Differential diagnosis:
Anterior wall prolapse: congenital or inclusion dermoid vaginal cyst, urethral diverticulum.Uterovaginal prolapse: large uterine polyp.
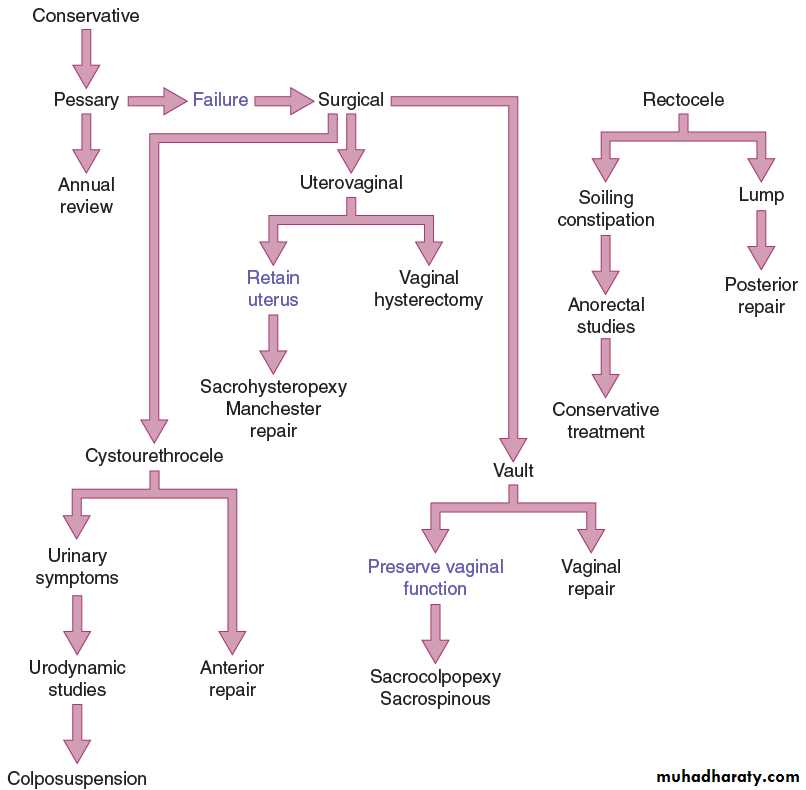
Treatment:
The choice of treatment depends on the patient’swishes, level of fitness and desire to preserve coitalfunction.Prior to specific treatment, attempts shouldbe made to correct obesity, chronic cough orconstipation. If the prolapse is ulcerated, a 7-daycourse of topical oestrogen should be administered.
Prevention:
Shortening the second stage of delivery and reducingtraumatic delivery may result in fewer womendeveloping a prolapse.
The benefits of episiotomy andhormone replacement therapy at the menopause havenot been substantiated.
Medical:
If a woman is found to have uterovaginal prolapseon examination but has no symptoms, then it wouldbe inappropriate to offer any surgical treatment andeither observation or conservative therapy wouldbe best.If symptoms are mild, then pelvic floorphysiotherapy is offered but there are no randomizedcontrolled trials examining the effectiveness of physiotherapy on prolapse.
Silicon rubber-based ringpessaries are the most popular form of conservativetherapy.
They are inserted into the vagina in muchthe same way as a contraceptive diaphragm andneed replacement at annual intervals.
Shelf pessaries are rarely used but may be useful inwomen who cannot retain a ring pessary.
The use ofpessaries can be complicated by vaginal ulceration andinfection.
The vagina should therefore be carefullyinspected at the time of replacement.
There are awhole range of newer pessaries that are undergoingevaluation and these may be more comfortable for thepatient.
Indications for pessary treatment are:
patient’s wish;as a therapeutic test;
childbearing not complete;
medically unfit;
during and after pregnancy (awaiting involution);
while awaiting surgery.
Surgery:
The aim of surgical repair is to restore anatomyand function.
There are vaginal and abdominaloperations designed to correct prolapse, and choiceoften depends on a woman’s desire to preserve coital function.
1- Cystourethrocele
Anterior repair (colporrhaphy) is the most commonlyperformed surgical procedure but should be avoidedif there is concurrent stress incontinence.An anteriorvaginal wall incision is made and the fascial defectallowing the bladder to herniate through is identifiedand closed. With the bladder position restored, anyredundant vaginal epithelium is excised and theincision closed.
2- Rectocele
Posterior repair (colporrhaphy) is the most commonlyperformed procedure.A posterior vaginal wallincision is made and the fascial defect allowing therectum to herniate through is identified and closed.
With the rectal position restored, any redundantvaginal epithelium is excised and the incision closed.
3- Enterocele
The surgical principles are similar to those of anteriorand posterior repair, but the peritoneal sac containingthe small bowel should be excised.In addition, thepouch of Douglas is closed by approximating theperitoneum and/or the uterosacral ligaments.
4- Uterovaginal prolapse
Uterine preserving surgery:Uterine preserving surgery is used largely whena woman still wants to have further children andtherefore the uterus has to be preserved. Occasionally,a woman wishes to preserve her uterus and then maychoose this option:
Hysterosacropexy
The Manchester repair
Le Fort colpocleisis
‘Total mesh’ procedure using an introducer device
Procedures involving hysterectomy:
These procedures involve removal of the uterus:
Vaginal hysterectomy
Total abdominal hysterectomy and sacrocolpopexy
Subtotal abdominal hysterectomy and sacrocervicopexy
5- Vault prolapse
Sacrocolpopexy is similar tosacrohysteropexy but the inverted vaginal vault isattached to the sacrum using a mesh and the pouch ofDouglas is closed. Sacrospinous ligament fixation is avaginal procedure in which the vault is sutured to oneor other sacrospinous ligament.
Key points:
A prolapse is a protrusion of an organ or structure beyond its normal confines; prolapses are extremely common in multiparous women.
Damage to the major supports of the vagina, i.e. ligaments, fascia and levator ani muscles, leads to prolapse.
Childbirth injury is the major aetiological factor.
Most women with prolapse present with non-specific symptoms, such as a lump and backache.
Women with cystourethrocele often have urinary symptoms.
Women with rectocele often have bowel symptoms.
Diagnosis is made by clinical examination.
Surgery is the mainstay of treatment.
Treatment of prolapse: