
Anaesthesia
Local & Regional Anaesthesia
Dr. Dena A. Alkazzaz
F.I.C.M.S. (Anaesthesia & intensive care)
Lecturer of anaesthesia /dep. of surgery /Mosul medical collage
Local anaesthesia may be safer than general anaesthesia in certain circumstances & lead to fewer unpleasant side
effects, but it is often ignored in favor of comparative speed & ease of administration of general anaesthesia.
• Analgesia : The state when only relief of pain is provided. This may allow some minor surgical procedures to be
performed, for example infiltration analgesia for suturing.
• Anaesthesia : The state when analgesia is accompanied by muscle relaxation, usually to allow major surgery to be
undertaken. Regional anaesthesia may be used alone or in combination with general anaesthesia.
All drugs will be referred to as local anaesthetics irrespective of the technique for which they are being used.
Mechanism of action of local anesthetic drugs:
Agents injected or applied topically close to the cell or to the axonal nerve process on which they are to act, they
penetrate the axonal or cell membrane where exert their blocking action.
Later on they are absorbed into the blood stream, destroyed & eliminated.
Local anesthetic drugs are composed of aromatic & tertiary amine groups, linked by a group that is either an ester or
amide.
At relatively alkaline media around the nerve the local anesthetic drugs molecule is lipophilic so enable the local
anesthetic to penetrate the lipoid membrane of the nerve axon. Inside the nerve is relatively acidic & these leads to
release of ionized form of local anesthetic that it causes block the sodium channels in the nerve cell membrane & thus
prevent the ionic exchange essential for the normal transmission of the electrical impulse along the axon.
Indication for Local or Regional Anaesthesia:
1.If life of the patient would be endangered by unconsciousness, for example by respiratory obstruction.
2.Emergencies: when there is no time to reduce the hazards of general anaesthesia, for example cases of full stomach &
operative obstetric delivery, in some cases of diabetes mellitus, myasthenia gravis.
3.Avoid hazard of administration of general anaesthetic drugs, for example acute intermittent porphyria, repeated
halothane anesthesia, myotonia, and renal or hepatic failure.
4.Procedure require patient co-operation for example tendon repair
5. Minor superficial & body surface lesion for example dental extraction, skin lesion, minor laceration & scar revision.
6. To provide postoperative analgesia for example circumcision, thoracotomy, herniorraphy, skin graft donor site &
abdominal surgery.
7. Provide sympathetic block as in free flap or reimplantation surgery or limb ischemia.
8. Blood loss can be reduced with controlled hypotension.
9. If the patient or the surgeon or the anesthetist has a preference for local anesthesia & can convince the other parties
that local anesthesia is appropriate.
10. There is a considerable reduction in the equipment required and the cost of anaesthesia.
5. Extensive surgery that will require toxic doses of local anesthetic agent.
6. Lack the consent or co-operation on the part of patient.
7. If immediate anesthesia is required (for example obstructed breach delivery).
8. Lacked of skilled personnel.
9. Lacked of resuscitation facilities.
Local anesthetic drugs: -
Most commonly used local anesthetic drugs are: -
1. Amide linked local anesthetic drugs; lignocaine, prilocaine, bupivacaine, levo bupivacaine, ropivacaine.
2. Ester linked local anesthetic drugs; cocaine, procaine.

Lignocaine: -
1. Rapid onset of action.
2. Duration of action: 90 min without adrenalin, 120 min with adrenaline.
3. Use for infiltration, peripheral nerve block, spinal, epidural, intravenous regional, in concentration: 0.
5%, 1%, 1.5%, 2% solution.
4. For topical anesthesia used in concentration of 4%, 5%.
5. Maximum safe dose 4.5mg/kg without adrenalin, 7mg/kg with adrenaline.
Prilocaine: -
1. Onset slower than lignocaine.
2. Duration of action: little longer than lignocaine.
3. Concentration similar to that of lignocaine.
4. Toxicity less than that of lignocaine.
5. Maximum safe dose 8mg/kg.
6. Most important use: -
When large volume of drug is required.
Used in intravenous regional anaesthesia (IVRA) or Bier’s block
Bupivacaine: -
1. Slower in onset than lignocaine.
2. Long duration of action because its greater ability to bind to protein, so adrenaline has no effect on it.
3. Maximum safe dose 3mg/kg with or without adrenalin.
4. More potent than lignocaine so used in concentration 0.125-0.75%.
Epinephrine (Adrenaline): -
Added to local anaesthetic solution in strength 1:80 000-
1:200 000 to obtain intense vasoconstriction (alpha-adrenergic
effect) so: -
1. Decrease blood flow at the site of injection, leading to decrease vascular absorption & increase neuronal uptake of
local anaesthetic, so the depth & duration of neuronal blockade are increased.
2. Decrease the likelihood of high blood level of local anaesthetic (decrease toxic reaction of local anaesthetic).

3. In infiltration technique, local vasoconstriction leads to decrease bleeding.
Side effect: -
1. If injected intravenously may cause cardiac effect (ventricular effect, ventricular tachycardia, ventricular fibrillation),
hypertension, and myocardial ischemia.
2. Should not be used for ring block of digit, penis, tip of nose that may cause vasoconstriction of end arteries & lead to
ischemia & gangrene.
3. Local ischemia in infected area lead to anaerobic infection.
Local anaesthetic toxicity:-
High plasma levels of local anaesthetic can be found in:
1. Drug overdose
2. Direct intravascular injection
3. Rapid absorption/ injection into a highly vascular area
4. Cumulative effect of multiple injections or continuous infusion
Symptoms and signs of toxicity:-
Mild toxicity:-
1. Perioral tingling
2. Metallic taste
3. Tinnitus
4. Visual disturbance
5. Slurred speech
Moderate toxicity:-
1. Altered conscious state
2. Convulsion
3. Coma
Potentially fatal toxicity:-
1. Respiratory arrest
2. Cardiac arrhythmias
3. Cardiovascular collapse
Preparation & precaution before the use of local anaesthesia: -
1. Formal explanation to the patient & verbal consent.
2. Starvation especially when supplementary sedation is a possibility.
3. Indwelling intravenous needle & infusion.
4. Monitoring: ECG, blood pressure, SpO2 (oximeter).
5. Resuscitation equipment: O2, suction, positive pressure ventilation, defibrillator should be available.
6. Resuscitation medicine & supplementary drug & apparatus for systemic analgesia & sedation should be
available.
Types of Local Anaesthesia
Topical anaesthesia: -
Most local anaesthetics produce rapid anaesthesia when applied to mucous membranes.
Sites: eye (conjunctiva), nasal cavity, throat, larynx, lower respiratory tract, ear, urethra, birth canal.
Application: instillation, spray, ointment, pastes, gels.
1. EMLA cream: mixture of lignocaine & prilocaine for application to the skin before venipuncture, this is
especially valuable for children but take one hour to act.
2. Lignocaine: 4% maximum 5ml in 70kg man.
3. Cocaine: 5% maximum 5ml in 70kg man.
Local infiltration - field block: -
Superficial injection into or around the lesion to block sensory nerve ending for body surface surgery, it is simple,
familiar & reliable technique.
Peripheral nerve blocks
Major peripheral nerve blocks-plexus block
Peripheral nerve block is placed proximal to the site of the scheduled painful procedure or the site of pain. These blocks
can be accomplished either by injecting local anesthetic according to: -
1. Anatomical land marks (e.g. intercostals, finger& toe, penile nerve block).
2. Searching for paraesthesia with the needle tip (some technique of brachial plexus block).
3. Using a special nerve stimulator connected to the needle (e.g. femoral nerve block, some
techniques of brachial plexus block).
Intravenous regional anaesthesia
(Bier’s block)
1. Produce anaesthesia to the limbs usually the upper limbs.
2. Large volume of local anaesthetic is used 30-40ml of 0.5% prilocaine without adrenaline.
3. Used in patients when there is no contraindication to use arterial tourniquet.
4. Cuff inflated 100 mmHg above the systolic blood pressure.
5. Local anaesthetic injected to intravenous cannula inserted as distal as possible.
6. Cuff should be inflated at least 20min whatever the length of operation, otherwise the concentration of
local anaesthetic in the blood will reach an unacceptably high level when it is deflated.
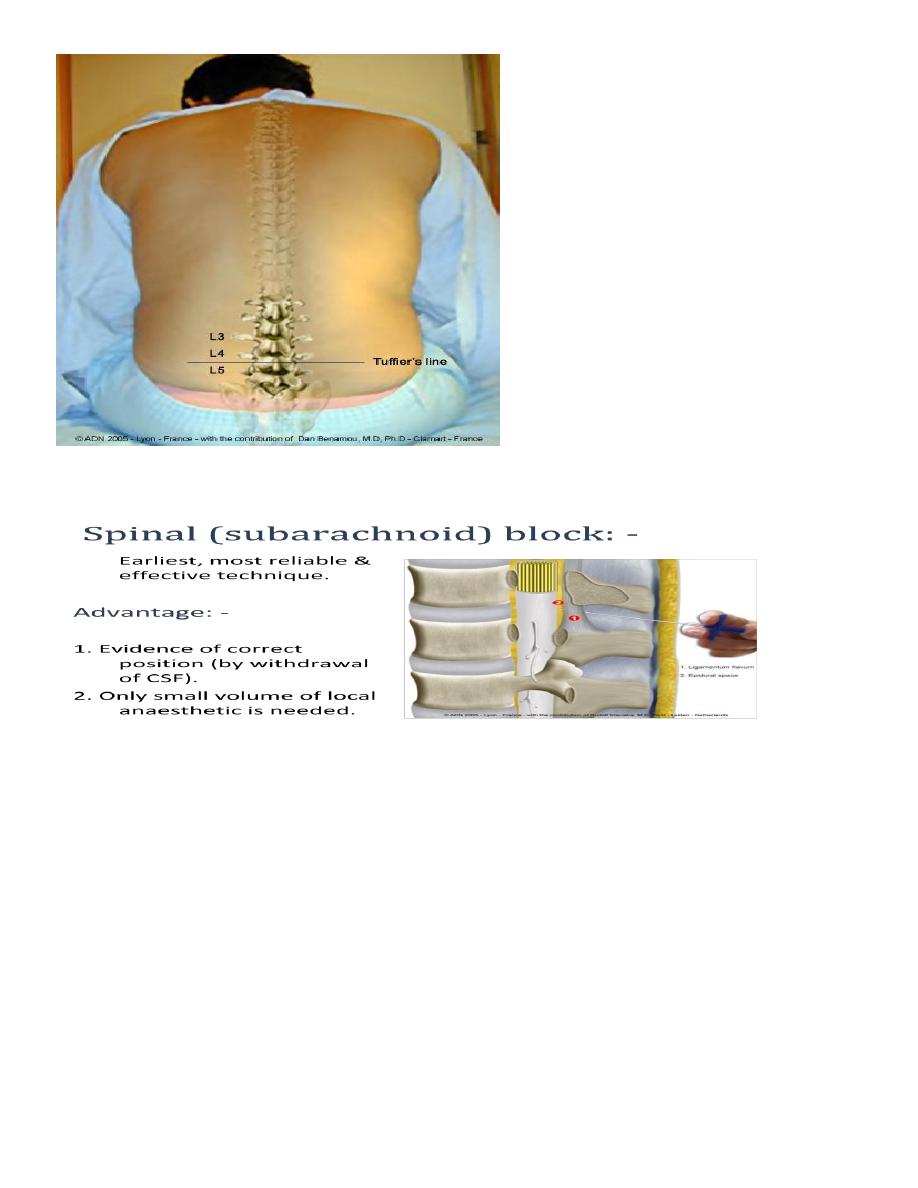
2. Central block-spinal/epidural block
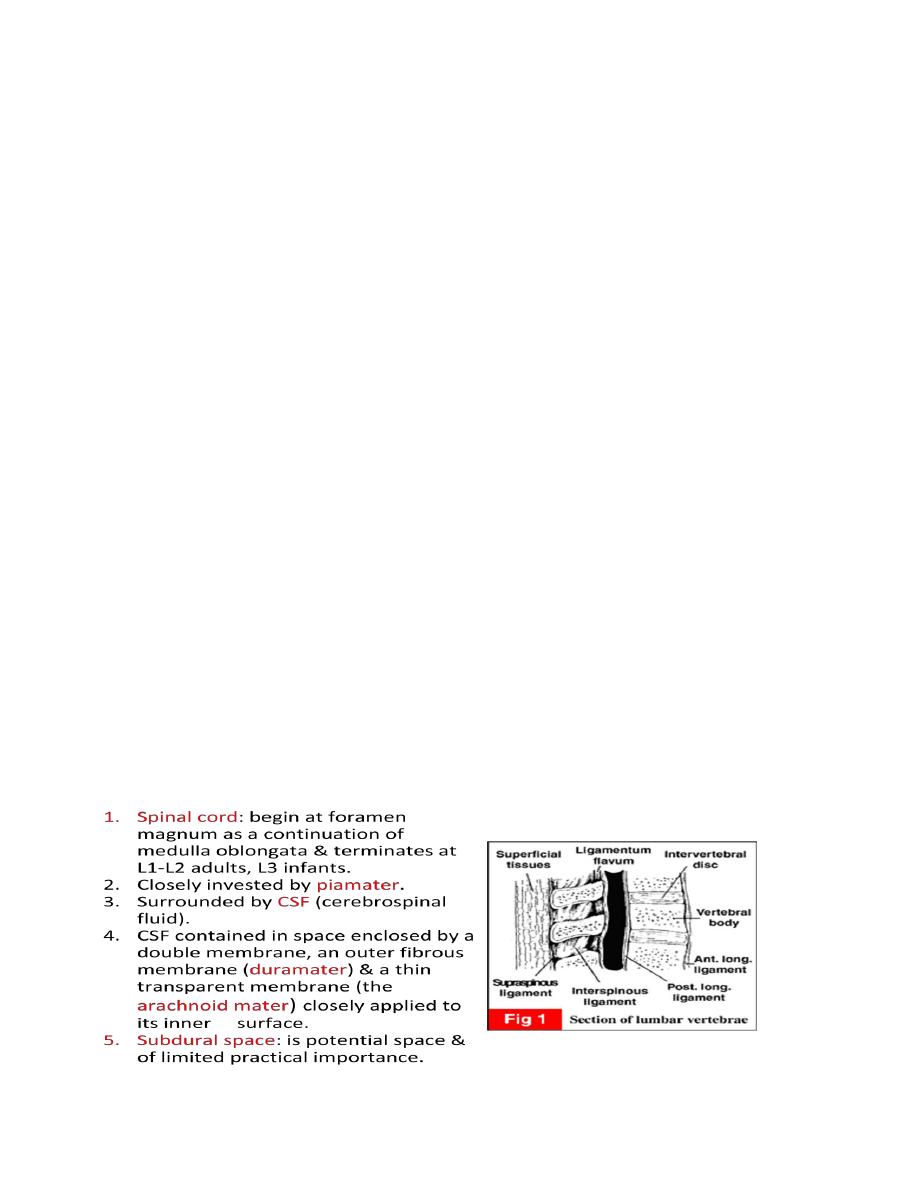
3. Anatomy of the vertebral column& spinal cord& its investing membrane
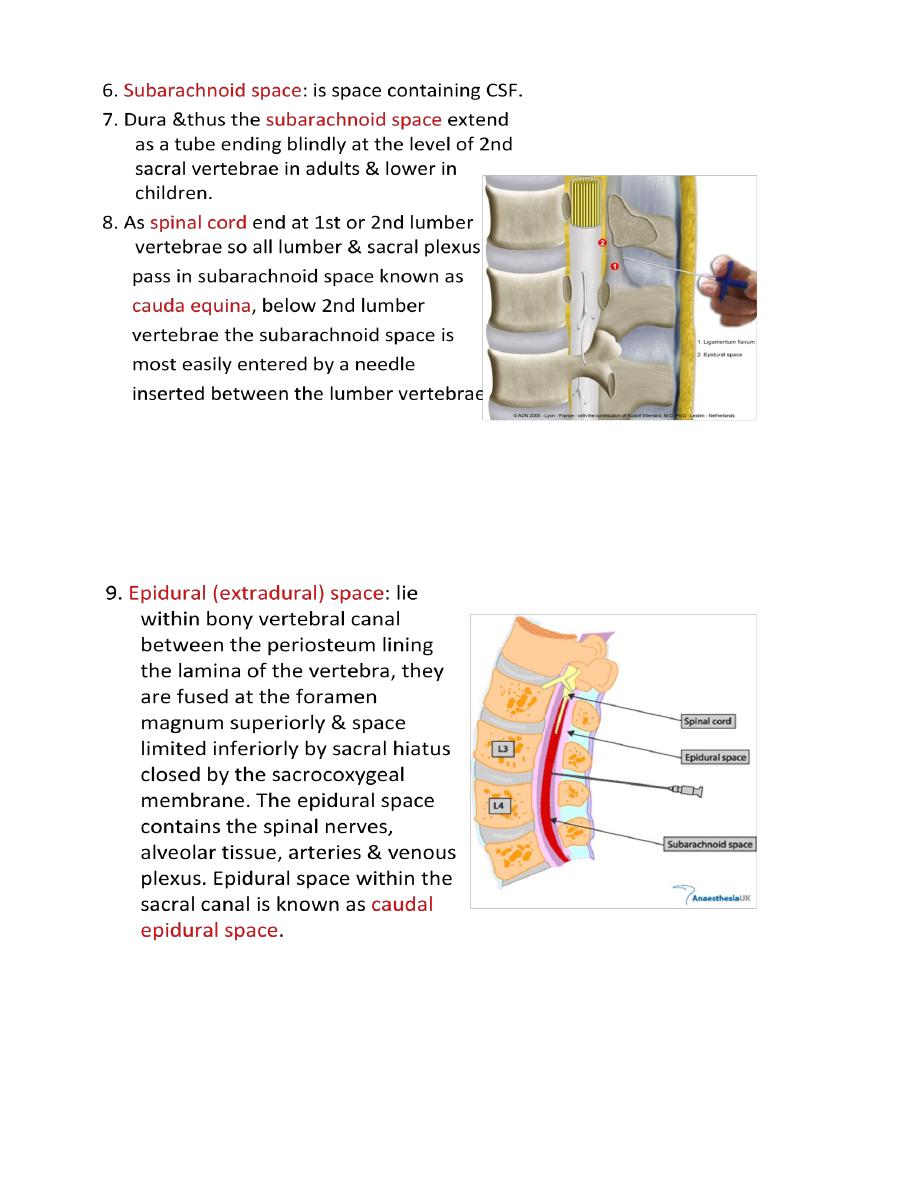
4. 6. Subarachnoid space: is space containing CSF.
5. 7. Dura &thus the subarachnoid space extend as a tube ending blindly at the level of 2nd sacral vertebrae in
adults & lower in children.
6. 8. As spinal cord end at 1st or 2nd lumber vertebrae so all lumber & sacral plexus
7. pass in subarachnoid space known as
8. cauda equina, below 2nd lumber
9. vertebrae the subarachnoid space is
10. most easily entered by a needle
11. inserted between the lumber vertebrae.
Disadvantage:
1. Risk of introduces infection (meningitis).
2. Spinal headache (per & post operatively due to CSF leak at the site of dural puncture).
3. Hypotension (due to sympathetic block).
4. High spread can cause prolonged respiratory paralysis necessitate artificial ventilation.
5. Damage to the cord or to spinal nerve roots whether from direct trauma or 2ry to spasm of the arteries
supplying the cord or 2ry to hypotension.
6. Urinary retention.
7. Backache.
8. Expanding hematoma & possible compression of spinal cord or nerves.
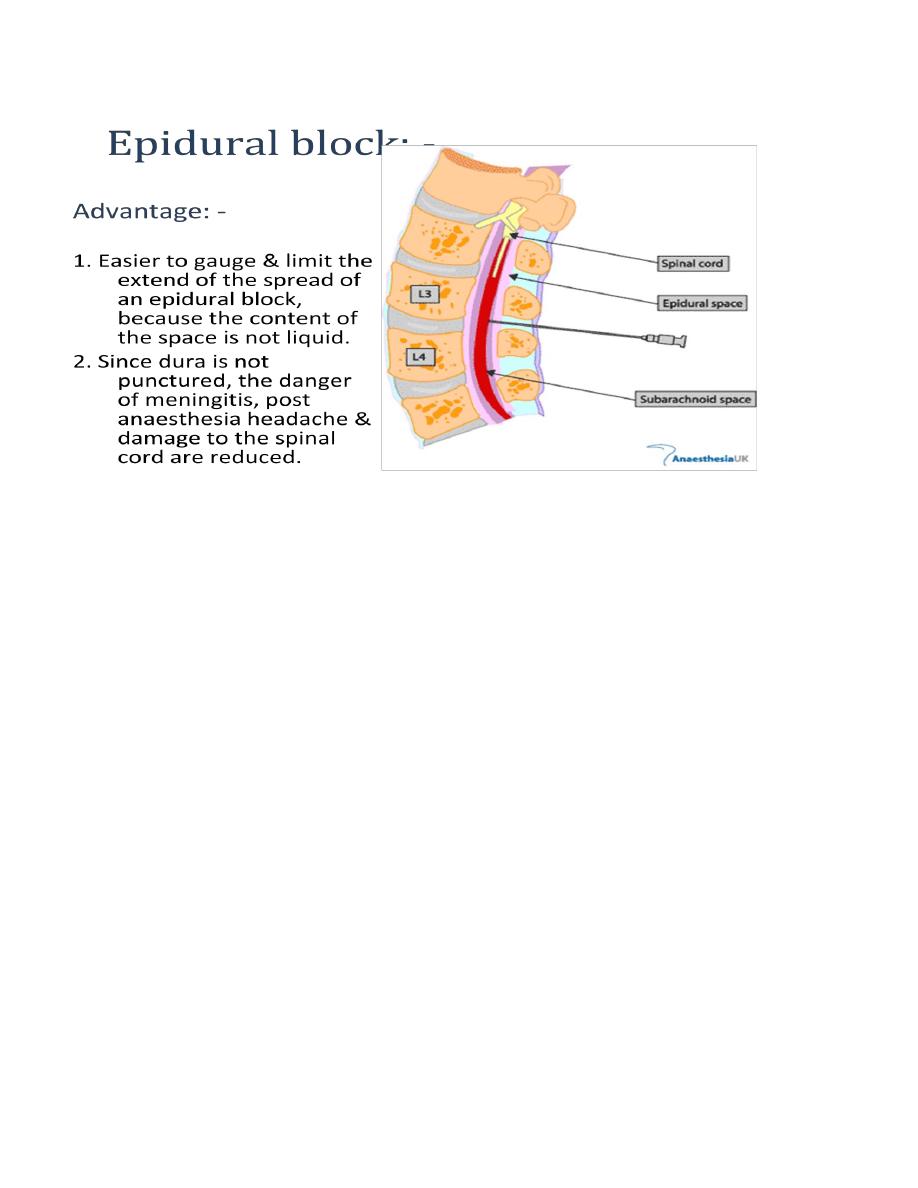
Disadvantage: -
1. Epidural block may be patchy due to anatomical variation like fibrous septa in the epidural space.
2. Much larger doses of local anesthetic are required for epidural block than for spinal subarachnoid
anaesthesia.
3. Technique is more difficult than subarachnoid.
4. There is always a danger that either the needle or the catheter may enter a blood vessel.
5. Dura may be penetrated with a wide bore needle so increase incidence of spinal headache.
6. If dura is penetrated & not detected, the volume of local anesthetic is several times than that required
for spinal anaesthesia may be injected subdurally causing total spinal anaesthesia (hypotension,
unconsciousness, apnea).