Dr. Safeya Alchalabi
Antidepressant drugs1

2
3
4
Groups of antidepressant drugs
• Drug• Advantages
• Disadvantages
• TCAs
• Well studied
• Efficacy never surpassed
• Cardiotoxic*, dangerous in overdose
•
•
• Anticholinergic side effects**
•
• Useful sedative effect in selected patients
• Cognitive impairment
•
•
• Weight gain during longer-term treatment
• SSRIs/SNRIs
• Lack cardiotoxicity***: relatively safe in overdose †
• Long-term toxicity not fully evaluated
•
• Not anticholinergic
• Gastrointestinal disturbance, sexual dysfunction
•
• No cognitive impairment
• May worsen sleep and anxiety symptoms initially
•
• Relatively easy to give effective dose
• Greater risk of drug interaction
• Trazodone
• Lacks cardiotoxicity, relatively safe in overdose
• Daytime drowsiness
• Mirtazapine
• Useful sedative effect in selected patients
• Weight gain common
• Less well-established efficacy in severe depression
5
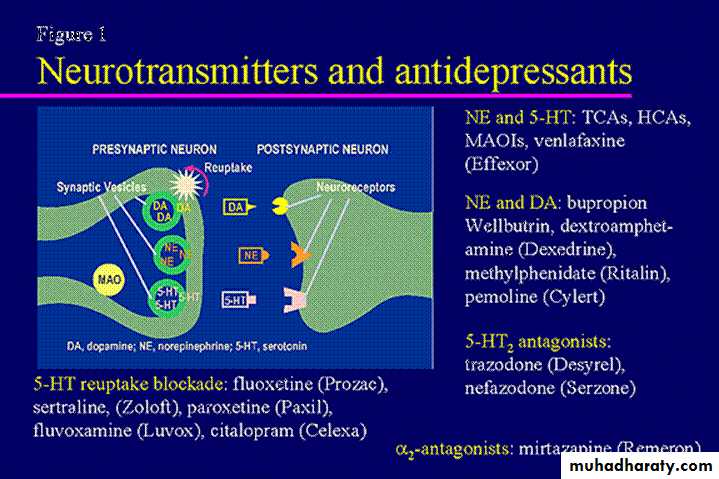
Selective serotonin reuptake inhibitors
In general, SSRIs are now preferred to tricyclic antidepressants in the firstline treatment of depression because they are moderately better tolerated and markedly less toxic in overdose
6
Selective serotonin reuptake inhibitors
Pharmacological propertiesSix SSRIs—citalopram, escitalopram, fluoxetine, fluvoxamine, paroxetine, and sertraline—are available at present for clinical use.
They all inhibit the reuptake of 5-HT with high potency and selectivity.
7
SSRI
8
9
Selective serotonin reuptake inhibitors
Pharmacokinetics
The half-lives of citalopram, escitalopram, fluvoxamine, paroxetine, and sertraline are between 20 and 30 hours, whereas the half-life of fluoxetine is 48–72 hours.
Fluoxetine is metabolized to norfluoxetine, which is also a potent 5-HT uptake blocker and has a half-life of 7–9 days.
10
Side effects of SSRIs
• Gastrointestinal• Common: nausea, appetite loss, dry mouth, diarrhoea, constipation, dyspepsia Uncommon: vomiting, weight loss
• Central nervous system
• Common: headache, insomnia, dizziness, anxiety, fatigue, tremor, somnolence
• hUncommon: extrapyramidal reaction, seizures, mania
• Other
• Common: sweating, delayed orgasm, anorgasmia Uncommon: rash, bleeding, pharyngitis, dyspnoea, serum sickness, hyponatraemia, alopecia
11
SSRIs and suicidal behavior
In adolescents and children the risk of self-harm with SSRIs might be greater.SSRIs can cause agitation and restlessness early in treatment, and it is possible that in predisposed individuals this might trigger dangerous behaviour.
the relative risk in the first 9 days of treatment was increased almost 40-fold
increased rates of self-harm has been reported in patients with depression in the early stages of psychological treatment.
12
13
Differences between SSRIs
DrugRisk of pharmacokinetic interaction *
Discontinuation syndrome
Other
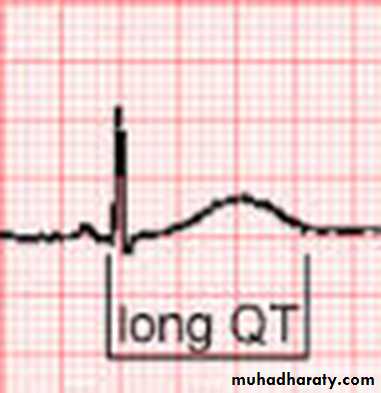
Citalopram
+
+
Increases QT interval
Escitalopram
+
+
Increases QT interval
Fluoxetine
+++
0
Increased risk of agitation, slower onset of action
Fluvoxamine
+++
+++
Less well tolerated
Paroxetine
+++
+++
Weight gain
Sertraline
++
++
May have dopaminergic effects
14
Tricyclic antidepressants
Tricyclic antidepressants continue to be useful agents because of their efficacy in severely ill depressed patients and those with treatment-refractory illness.
At low doses tricyclics are still used widely for the treatment of neuropathic pain syndromes.
15
Compounds available
These includeamitriptyline,
clomipramine,
desipramine dosulepin,
doxepin,
imipramine,
lofepramine,
nortriptyline, and
trimipramine.
16
Clomipramine is the most potent of the tricyclic antidepressants in inhibiting the reuptake of 5-HT.
Tricyclic antidepressants
17
Lofepramine is a fairly selective inhibitor of noradrenaline reuptake, and has fewer anticholinergic and antihistaminic properties than amitriptyline.
, it is not cardiotoxic safer than other tricyclics for patients with cardiovascular disease.
There have been reports of hepatitis in association with lofepramine.
Tricyclic antidepressants
18Some adverse effects of tricyclic antidepressants
• Pharmacological action• Adverse effec
• Muscarinicreceptor blockade (anticholinergic)
• Dry mouth, tachycardia, blurred vision, glaucoma, constipation, urinary retention, sexual dysfunction, cognitive impairmen
• α1 -Adrenoceptor blockade
• Drowsiness, postural hypotension, sexual dysfunction, cognitive impairment
• Histamine H1 receptor blockade
• Drowsiness, weight gain
• Membranestabilizing properties
• Cardiac conduction defects, cardiac arrhythmias, epileptic seizures
19
Psychiatric effects.
These include tiredness and drowsiness with amitriptyline and other sedative compounds, insomnia with desipramine and lofepramine, and acute organic syndromes.Mania may be provoked in patients with bipolar disorders and generally tricyclics are not recommended for patients with bipolar illness.
20
Cardiovascular effects.
Tachycardia and postural hypotension occur commonly.The electrocardiogram frequently shows prolongation of PR and QT intervals, depressed ST segments, and flattened T-waves.
Ventricular arrhythmias and heart block develop occasionally, more often in patients with pre-existing heart disease.
21
Toxic effects
The main signs of overdosage.The cardiovascular effects include ventricular fibrillation, conduction disturbances, and low blood pressure. Heart rate may be increased or decreased Sedation and coma lead to respiratory depression.
The resulting hypoxia increases the likelihood of cardiac complications.
Aspiration pneumonia may develop.
In practice most patients need only supportive care, but cardiac monitoring is important, and arrhythmias require urgent treatment by a physician in an intensive care unit.
22
TCAs
Contraindications
agranulocytosis,
severe liver damage,
glaucoma,
prostatic hypertrophy,
uncontrolled epilepsy, and
significant cardiovascular disease.
Tricyclics must be used cautiously in epileptic patients and in the elderly.
23
Monoamine oxidase inhibitors
MAOIs were introduced just before the tricyclic antidepressants, but their use has been less widespread because of both troublesome interactions with foods and drugs.In adequate doses MAOIs are useful antidepressants, often producing clinical benefit in depressed patients who have not responded to other medication or ECT.
MAOIs can be useful in refractory anxiety states
24
Monoamine oxidase inhibitors
Pharmacological propertiesMAOIs inactivate enzymes that oxidize noradrenaline, 5-HT, dopamine, and tyramine, and other amines.
there are two forms of MAO—type A and type B —.
In general, MAO-A metabolizes intraneuronal noradrenaline and 5-HT, whereas both MAO-A and MAO-B metabolize dopamine and tyramine.
25
Monoamine oxidase inhibitors
Compounds available
Phenelzine
Isocarboxazid is reported to have fewer side effects than phenelzine,
Tranylcypromine differs from the other compounds:
Amphetamine-like stimulating effect, which may be helpful in patients with anergia and retardation. However, some patients have become dependent on the stimulant effect of tranylcypromine
tranylcypromine is more likely to give rise to hypertensive crises,
It is less likely to damage the liver.
Moclobemide differs from the other compounds in selectively binding to MAO-A, which it inhibits in a reversible way. This results in a lack of significant interactions with foodstuffs, and a quick offset of action.
26
MAOI
Side effect27
28
Monoamine oxidase inhibitors
Foods to be avoided during MAOI use● All cheeses except cream, cottage, and ricotta cheeses
● Red wine, sherry, beer, and liquors
● Pickled or smoked fish
● Brewer’s yeast products (e.g. Marmite, Bovril, and some packet soups)
● Broad bean pods (e.g. Italian green beans)
● Beef or chicken liver
● Fermented sausage (e.g. bologna, pepperoni, salami)
● Unfresh, overripe, or aged food (e.g. pheasant, venison, unfresh dairy products)
29
Monoamine oxidase inhibitors
Moclobemide and tyramine reactions
The hypertensive effect of oral tyramine is potentiated much less by moclobemide than by non-selective MAOIs.
Tyramine has relatively little effect in patients who are receiving moclobemide because MAO-B (present in the gut wall and the liver) is still available to metabolize much of the tyramine ingested.
Another factor may be that the interaction between moclobemide and MAO-A is reversible, thus allowing displacement of moclobemide from MAO when tyramine is present in excess.
30
Monoamine oxidase inhibitors
The serotonin syndrome.A number of drugs that potentiate brain 5-HT function can produce a severe neurotoxicity syndrome when combined with MAOIs.
It is worth noting that some of these symptoms resemble the neuroleptic malignant syndrome with which 5-HT neurotoxicity is occasionally confused.
Combination of MAOIs with SSRIs, venlafaxine, and clomipramine is contraindicated.
The combination of MAOIs with L-tryptophan has also been reported to cause 5-HT toxicity.
31
Monoamine oxidase inhibitors
Interactions with drugssympathomimetic amines
L-Dopa
Local anaesthetics
Some opiates (particularly pethidine, tramadol, and fentanyl),
cocaine,
insulin can be involved in dangerous interactions.
Sensitivity to oral antidiabetic drugs is increased, with a consequent risk of hypoglycaemia.
The ability of MAOIs to cause postural hypotension can increase the hypotensive effects of other agents.
The metabolism of carbamazepine, phenytoin, and other drugs that are broken down in the liver may be slowed.
32
Monoamine oxidase inhibitors
Clinical features of the serotonin syndrome
Neurological Myoclonus, nystagmus, headache, tremor, rigidity, seizures
Mental state Irritability, confusion, agitation, hypomania, coma
Other Hyperpyrexia, sweating, diarrhoea, cardiac arrhythmias, death
33
Monoamine oxidase inhibitors
Clinical features of the serotonin syndromeIf a 5-HT syndrome develops, all medication should be stopped and supportive measures instituted.
Drugs with 5-HT-receptor antagonist properties such as cyproheptadine or propranolol may be helpful
34
Other antidepressant drugs
AgomelatineMirtazapine
Trazodone
Venlafaxine
Duloxetine
Vortioxetine
Reboxetine
L-Tryptophan
St John’s wort
Bupropion
35
Agomelatine
melatonin receptor agonista melatonin-like action on circadian rhythms.
might lead to increased dopamine release in the prefrontal cortex,
agomelatine appears comparable in efficacy to venlafaxine and paroxetine,
agomelatine was dosed once-daily at 9.00 pm,
The most common adverse effects of agomelatine are nausea and dizziness.
Agomelatine is not sedating
Sexual dysfunction is less frequent than with SSRIs.
The most serious potential adverse effect of agomelatine is an increase in liver enzymes (ALT and AST).

36
Mirtazapine
Mirtazapine is a competitive antagonist at histamine H1 receptors and α1 - and α2 -adrenoceptors.Mirtazapine is not a muscarinic cholinergic antagonist and is not cardiotoxic.
The effective dose is usually between 10 mg and 45 mg daily.

37

The most serious side effect of trazodone is priapism
38
dose-related increases in blood pressure can occur.
39
40

depression-associated cognitive impairment,
41
better improvement in social function
42development of a severe scleroderma-like illness, the eosinophilia–myalgia syndrome (EMS), in which there is a very high circulating eosinophil count (about 20% of peripheral leucocytes), with severe muscle pain, oedema, skin sclerosis, and peripheral neuropathy. Fatalities have been reported.

43


St John’s wort is an extract from the plant, Hypericum perforatum.
It has been used in medicine for centuries for numerous indications, including burns, arthritis, snakebite, and depression.44

45