Panic disorder
ByDr. Safeyya Adeeb Alchalabi
Panic attack
EssencePanic attack A period of intense fear characterised by a constellation of symptoms that develop rapidly, reach a peak of intensity in about 10 mins, and generally do not last longer than 20-30 mins (rarely over 1 hr).
Attacks may be either
spontaneous (out of the blue) or
situational (usually where attacks have occurred previously).
Sometimes attacks may occur during sleep
(nocturnal panic attacks), and
rarely, physiological symptoms of anxiety may occur without the psychological component
(non-fearful panic attacks).
intense fear
10 mins
20-30 mins
(out of the blue)
nocturnal panic attacks
non-fearful panic attacks
situational
10 min
20-30mins(rarely1hr)Intense fear
Panic disorder
Recurrent panic attackswhich are not secondary to
substance misuse,
medical conditions, or
another psychiatric disorder.
Frequency of occurrence may vary from
many attacks a day, to
only a few attacks a year.
There is usually the persistent worry about having another attack or the consequences of the attack (which may lead to phobic avoidance of places or situations), and significant behavioural changes related to the attack.
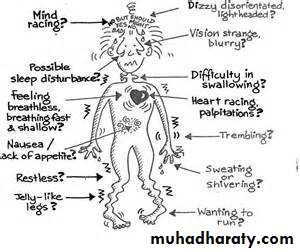
Symptoms/signs of panic attack
Symptoms associated with panic attacks
(in order of frequency of occurrence)
Palpitations, pounding heart, or accelerated heart rate.
Sweating.Trembling or shaking.
Sense of shortness of breath or smothering.
Feeling of choking or difficulties swallowing (globus hystericus).
Chest pain or discomfort.
Nausea or abdominal distress.
Feeling dizzy, unsteady, light-headed, or faint.
Derealization or depersonalization (feeling detached from oneself or one's surroundings).
Fear of losing control or going crazy.
Fear of dying (angor animus).
Numbness or tingling sensations (paraesthesia).
Chills or hot flashes.
Palpitations
Sweating
Trembling or shaking
shortnessof breath
choking or difficulties swallowing
Chest pain
Nausea
or abdominal distressdizzy, unsteady,
light-headed, or faint.Derealization or depersonalization
losing control
or going crazy
Fear of dying
Numbness or
tingling sensations
Chills or hot flashes
Symptoms/signs of panic attack
Physical symptoms/signs are related to autonomic arousal (e.g. tremor, tachycardia, tachypnoea, hypertension, sweating, GI upset) which are often compounded by HVS (in 50-60% of cases).Concerns of death from cardiac or respiratory problems may be a major focus, leading to patients presenting (often repeatedly) to emergency medical services.
Panic disorder may be undiagnosed in patients with unexplained medical symptoms (chest pain, back pain, GI symptoms including IBS, fatigue, headache, dizziness, or multiple symptoms).
Thoughts of suicide (or homicide) should be elicited as acute anxiety (particularly when recurrent) can lead to impulsive acts (usually directed towards self). Risk of attempted suicide is substantially raised where there is comorbid depression, alcohol misuse, or substance misuse.

Epidemiology
Lifetime prevalence:1.5-3.7% for panic disorder,
8% for panic attacks
Women are 2-3 times more likely to be affected than men.
Age of onset has a bimodal distribution with highest peak incidence at 15-24 yrs and a second peak at 45-54 yrs. Rare after age 65.
2-3 times
15-24
45-54
Differential diagnosis
Other anxiety or related disorder (panic attacks may be part of the disorder),substance or alcohol misuse/withdrawal (e.g. amphetamines, caffeine, cocaine, theophylline, sedative-hypnotics, steroid),
mood disorders,
psychiatric disorders secondary to medical conditions,
medical conditions presenting with similar symptoms (e.g. endocrine: carcinoid syndrome, Cushing's disease/syndrome, hyperthyroidism, hypoglycemia, hypoparathyroidism, phaeochromocytoma; haematological: anaemia, cardiac: arrhythmias, mitral valve prolapse, MI; respiratory: COPD/asthma, HVS; neurological: epilepsy(esp. TLE, vestibular dysfunction).
Investigations
There are no specific tests for panic disorder, however basic investigations should be performed to exclude physical causes (e.g. FBC, U&Es, glucose, TFTs, ECG, and if supported by history/physical examination: toxicology, Ca2+, urinary VMA/pHVA, ECHO, and EEG).
Aetiological models
The serotonergic modelExaggerated post-synaptic receptor response to synaptic serotonin, possibly secondary to subsensitivity of 5HT1A receptors.
The noradrenergic model
Increased adrenergic activity, with hypersensitivity of presynaptic alpha2 receptors. (Locus coeruleus activity affects the hypothalamic-pituitary-adrenal axis and the firing rate is increased in panic.)The GABA model
Decreased inhibitory receptor sensitivity, with resultant excitatory effect.Cholecystokinin-pentagastrin model
Pentagastrin induces panic in a dose-dependent fashion in patients with panic disorder.The lactate model
Postulated aberrant metabolic activity induced by lactate, from studies involving exercise-induced panic attacks (replicated by IV lactate infusion).Aetiological models
The false suffocation carbon dioxide hypothesisExplains panic phenomena by hypersensitive brainstem receptors.
The neuroanatomical model
Suggests that panic attacks are mediated by a ˜fear network in the brain
that involves the amygdala, the hypothalamus, and the brainstem centres.
The genetic hypothesis
Panic disorder has moderate heritability of around 30-40%(from family and twin studies).
Most studies to date suggest that vulnerability is genetically determined,
but critical stressors are required to develop clinical symptoms.
The recently discovered genomic duplication (DUP25) on chromosome 15
(found in 7% of the population, but -95% of patients with panic disorder)
is perhaps the best evidence yet for genetic susceptibility.
Management guidelines
Combination of pharmacological and psychological treatments may be superior to single approach.Choice of initial approach will depend upon
patient preference,
past history of previous benefit,
costs,
availability,
local guidelines.
Management guidelines
Pharmacological
SSRIs
Citalopram(20-30mg),
Escitalopram(5-10mg),
Paroxetine (10-40mg),
Sertraline (50-200mg)
are recommended as 1st line by NICE.
In view of the possibility of initially increasing panic symptoms, start with low dose and gradually increase.
Beneficial effect may take up to 12 weeks and require high doses.
Management guidelines
Alternative antidepressantSNRIs(e.g.venlafaxine)
TCAs (e.g. imipramine or clomipramine)
MAOIs (e.g. phenelzine) may be superior to TCAs (for severe, chronic symptoms).
RIMAs (e.g. moclobemide).
Management guidelines
BDZs (e.g. alprazolam or clonazepam)should be used with caution (due to potential for abuse/dependence/cognitive impairment) but may be effective for severe, frequent, incapacitating symptoms.
Use for 1-2 weeks in combination with an antidepressant may cover symptomatic relief until the antidepressant becomes effective.
N.B. Anti-panic effects do not show tolerance, although sedative effects do.
Management guidelines
Limited benefit:
Little evidence to support use of
buspirone,
bupropion,
mirtazapine,
inositol,
reboxetine,
antipsychotics,
anticonvulsants,
propranolol.
Management guidelines
2nd –line treatment Consider change to a different class agent (i.e. TCA, SSRI, MAOI) or
Addition of BDZ,
Trial of bupropion,
Severe symptoms SGA (olanzapine).
Management guidelines
If successfulContinue treatment for -12-18mths before trial discontinuation (gradual tapering of dose over 2-4mths).
Do not confuse withdrawal effects (10-20% of patients) with re-emergence of symptoms (50-70% of patients).
If symptoms recur, continue for -1yr before considering second trial discontinuation.
(N.B. Patient may wish to continue treatment, rather than risk return of symptoms).
Emergency treatment of an acute panic attack
Maintain a reassuring and calm attitude (most panic attacks spontaneously resolve within 30 mins).
If symptoms are severe and distressing consider prompt use of BDZs (immediate relief of anxiety may help reassure the patient,provide confidence that treatment is possible, and reduce subsequent emergency presentations).
If first presentation, exclude medical causes (may require admission to hospital for specific tests).
If panic attacks are recurrent, consider differential diagnosis for panic disorder and address underlying disorder (may require psychiatric referral).
Management guidelines
PsychologicalBehavioural methods:
to treat phobic avoidance by exposure,use of relaxation, and
control of hyperventilation
(have been shown to be 58-83% effective).
Cognitive methods:
teaching about bodily responsesassociated with anxiety,
education about panic attacks,
modification of thinking errors.
Psychodynamic methods:
there is some evidence for brief dynamic psychotherapy,
particularly emotion-focused treatment
(e.g. panic-focused psychodynamic psychotherapy),
where typical fears of being abandoned or trapped are explored.
Issues of comorbidity
In view of high levels of comorbidity, treatment of these conditions should not be neglected.For the other anxiety disorders and depression, this issue is somewhat simplified by the fact that SSRIs and other antidepressants have been shown to be effective for these conditions too. However, behavioural interventions (e.g. for OCD, social phobia) should also be considered.
Alcohol/substance abuse may need to be addressed first, but specific treatment for persistent symptoms of panic ought not to be overlooked.
Phobias
Dr. Safeyya Adeeb AlchalabiEssence
• Social phobia• (social anxiety disorder)
• Simple or specific phobias
• Agoraphobia
• Symptoms of incapacitating anxiety (psychological and/or autonomic)
• are not secondary to delusional or obsessive thoughts and
• are restricted to particular social situations,
• leading to a desire for escape or avoidance (which may reinforce the strongly held belief of social inadequacy).
• Recurring excessive and unreasonable psychological or autonomic symptoms of anxiety, in the (anticipated) presence of a specific feared object or situation leading, whenever possible, to avoidance.
• DSM-5 distinguishes 5 subtypes:
• animals,
• natural environment,
• blood/injection/injury,
• situational, and
• Other.
• Anxiety and panic symptoms associated with places or situations where escape may be difficult or embarrassing
• e.g. of crowds, public places, traveling alone or away from home), leading to avoidance.
Epidemiology
• Social phobia
• Simple or specific phobias
• Agoraphobia
• Lifetime rates vary from 2.4% (ECA) to 12.1% (NCS),
• 12mth prevalence 6.8%
• male = female for those seeking treatment (however community surveys suggest male > female);
• bimodal distribution with peaks at 5 yrs and between 11-15 yrs
• often patients do not present until they are in their 30s.
• Prevalence: lifetime 12.5%,
• 12-mth (NCS) 8.7%,
• 6-mth (ECA)
• 4.5-11.9%;
• Male/female = 1:3;
• animal/situational phobias may be more common in female; main age of occurrence mainly in childhood /adolescence (mean 15yrs):
• animal phobias -7yrs,
• blood injection/injury-8
• claustrophobia -20yrs.
• Prevalence (6 month)
• 2.8-5.8% ;
• Male/female = 1:3; as for panic disorder,
• there is a bimodal distribution with the first being somewhat broader (15-35 yrs).
• In later life agoraphobic symptoms may develop secondary to physical frailty, with the associated fear of exacerbating medical problems or having an accident.
Management
• Social phobia
• Simple or specific phobias
• Agoraphobia
• Psychological
• CBT, in either an individual or group setting, should be considered as a first-line therapy (along with SSRIs/MAOIs) and may be better at preventing relapse. Components of this approach include relaxation training/anxiety management (for autonomic arousal), social skills training, and integrated exposure methods (modelling and graded exposure).
• Pharmacological
• B-blockers (e.g. atenolol) may reduce autonomic arousal, particularly for specific social phobia (e.g. performance anxiety). For more generalised social anxiety, both SSRIs (e.g. fluoxetine, paroxetine, sertraline) and MAOIs (e.g. phenelzine) are significantly more effective. Other treatment possibilities include RIMAs (e.g. moclobemide) or the addition of a BDZ (e.g. clonazepam, alprazolam) or buspirone
• Behavioural therapy
• ”treatment of choice: methods aim to reduce the fear response e.g. Wolpe's systematic desensitisation with relaxation and graded exposure (either imaginary or in vivo), virtual reality exposure (VRE).
• Other techniques: reciprocal inhibition, flooding (not better than graded exposure), and modelling.
• Cognitive methods: education/anxiety management, coping skills/strategies, and cognitive restructuring may enhance long-term outcomes,
• Pharmacological
• Generally not used, except in severe cases to reduce fear avoidance (with BDZs e.g. diazepam) and allow the patient to engage in exposure techniques may reduce the efficacy of behaviour therapy by inhibiting anxiety during exposure
• (B-blockers may be helpful, but reduce sympathetic arousal, not subjective fear.
• Clear 2ry depression may require an antidepressant (SSRIsescitalopram, paroxetine).
• Pharmacological
• Antidepressants As for panic disorder.
• BDZs short-term use only (may reinforce avoidance) most evidence for alprazolam/clonazepam.
• Psychological
• Behavioural methods Exposure techniques (focused on particular situations or places), relaxation training, and anxiety management.
• Cognitive methods Teaching about bodily responses associated with anxiety/education about panic attacks, modification of thinking errors
Specific phobias-selected glossary
Accidents: Dystychiphobia
Animals: Zoophobia
Ants: Myrmecophobia
Automobiles: Amaxophobia, motorphobia
Bees: Apiphobia, melissophobia
Birds: Ornithophobia
Blood: Haemophobia
Bridges: Gephyrophobia
Cats: Felinophobia
Specific phobias-selected glossary
Choking/being smotheredAnginaphobia, pnigophobia, pnigerophobiaContamination, dirt, or infection Molysomophobia,
mysophobia
Creepy, crawly thingsHerpetophobia
Crossing streetsAgyrophobia
DarknessNyctophobia, scotophobia
DentistsDentophobia, Odontophobia
DepthBathophobia
DoctorsIatrophobia
Dogs or rabiesCynophobia
EverythingPanophobia, panphobia, pamphobia
Specific phobias-selected glossary
FeathersPteronophobia
FlyingAviophobia
Forests, at nightNyctohylophobia
FrogsBatrachophobia
Hair, fur, or animal skinsChaetophobia, Trichophobia, doraphobia
HorsesEquinophobia, hippophobia
HospitalsNosocomephobia
InjectionsTrypanophobia
JumpingCatapedaphobia
Lightning and thunderBrontophobia, karaunophobia
Specific phobias-selected glossary
MothsMottephobiaNeedlesAichmophobia, belonephobia
Open high placesAeroacrophobia
Operations: surgicalTomophobia
Place: enclosedClaustrophobia
Railways/trainsSiderodromophobia
RainOmbrophobia, Pluviophobia
RatsZemmiphobia
ReptilesHerpetophobia
SnakesOphidiophobia
SpidersArachnophobia.
VomitingEmetophobia
X-raysRadiophobia
Social phobia
Simple or specific phobias
Agoraphobia
Simple or specific phobias
Social phobia

