Achalasia:-
1. What is the meaning of achalasia?2. How can you diagnose a patient with achalasia?
3. An old patient with long history of GERD present with dysphagia, what do you think the cause of his condition?
4. How could you manage a patient with CA esophagus?
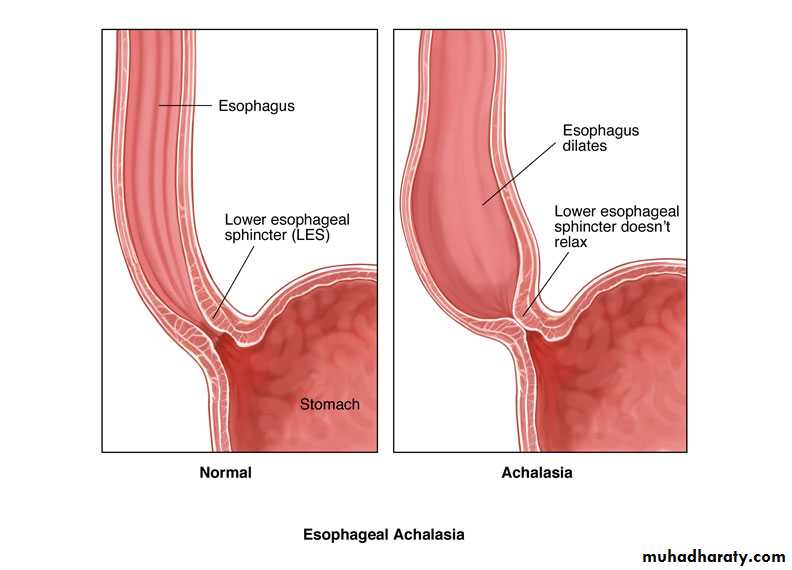
It is functional obstruction at the level of lower esophageal sphincter due to:-
Hypertonic lower oesophageal sphincter which fail to relax in response to the swallowing wave.Failure of propagated oesophageal contraction, leading to progressive dilatation of the gullet.
Degeneration of ganglion cell in the muscles of the mid and lower oesophageal. This abnormal non adrenergic non cholinergic (NANC) innervations related to abnormal nitric oxides synthesis with in the lower oesophageal sphincter and the body of esophagus
Loss of the dorsal vagal nuclei with in the brain stem in the later stages.
Chagas dis.:-is endemic in South America due to parasite trypanosome cruzy leads to myocarditis and arrange of motility disorders of the GIT at various level.
Clinical picture:-
It is usually developed in middle life but can occur at any age.
Dysphagia develops slowly; it is initially intermittent, worse for solid and is eased by drinking liquid and by standing and moving around post eating.Heart burn doesn’t occur because no GERD can occur. As disease progress, nocturnal aspiration and severe dysphagia for both solid and liquid (vigorous achalasia) .
Achalasia is a predisposing factor for CA esophagus rarely as squamous cell carcinoma.
Investigations:-
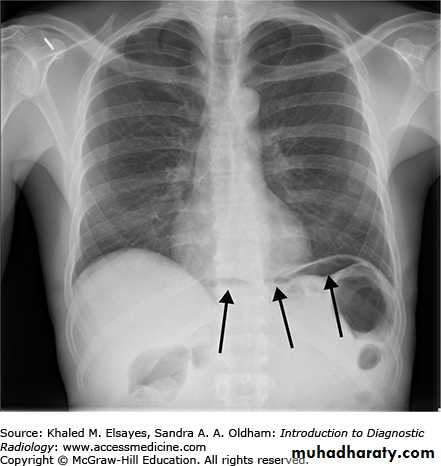
Chest x-ray may be abnormal in late dis., with widening of mediastinum (oesophageal dilatation) and presence of aspiration pneumonitis.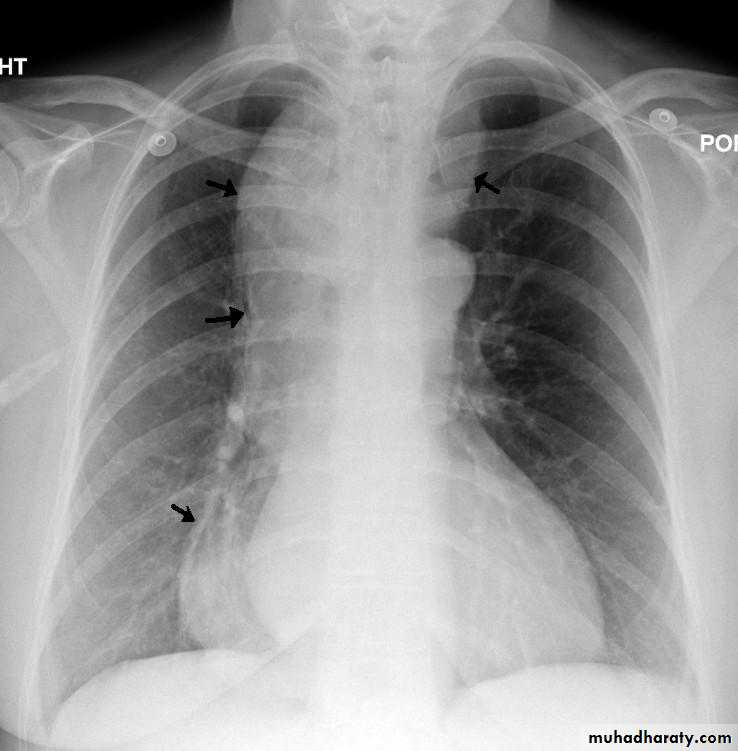
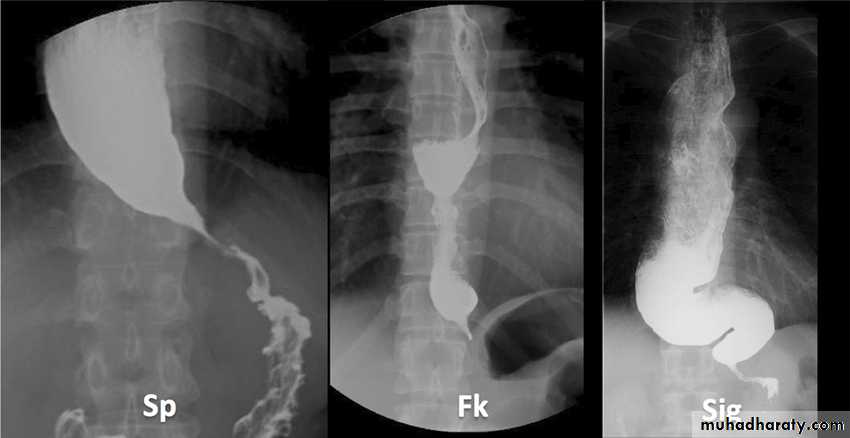
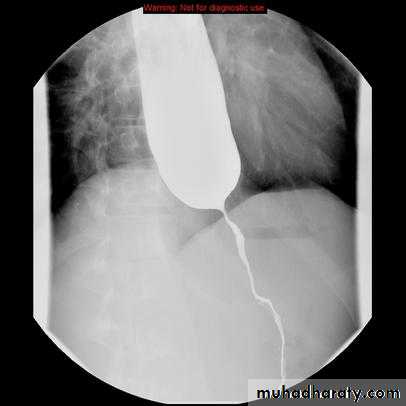
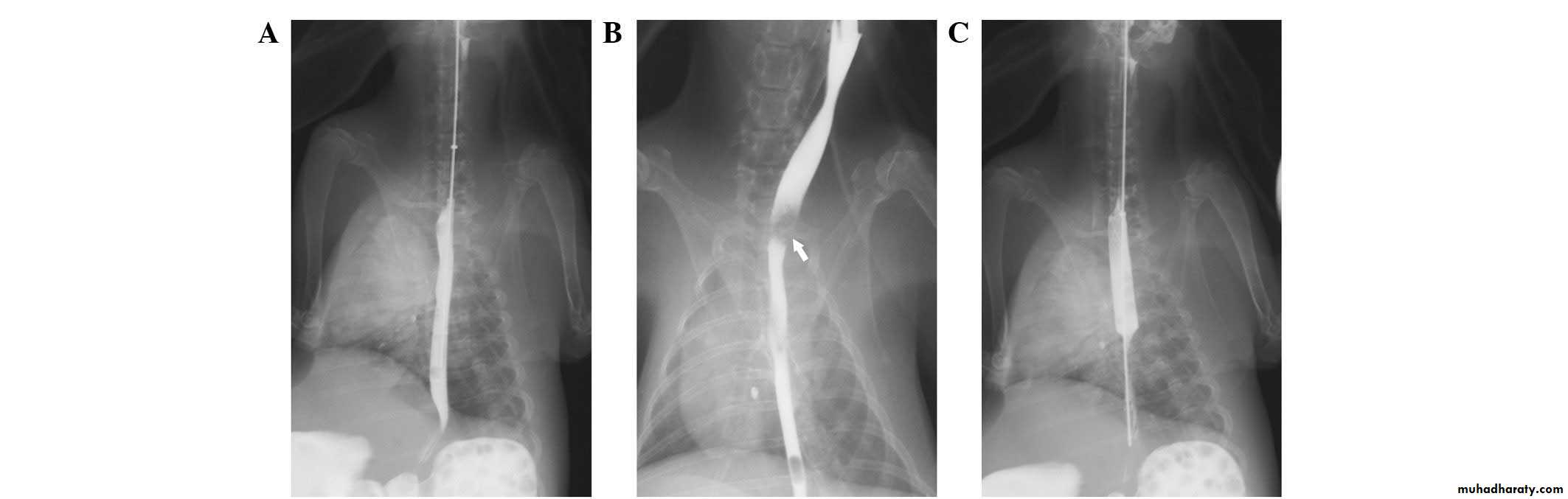
Barium swallows . Tapered narrowing (bird beak) of the lower oesophagus and dilating body of oesophagus, a peristaltic and food filled (sigmoid oesophagus).
Endoscope. is a must ,to exclude carcinoma of oesophagus, which can give (pseudo achalasia) due to the same radiological
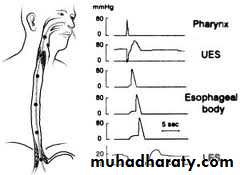
Manometer:- confirms high pressure , non-relaxing lower esophageal sphincter ,with poor contractility of the oesophageal body. The intraoesophageal pressure is higher than the gastric pressure due to a fluid and food filled oesophagus.
Differential diagnosis:-
Chagas dis.pseudo achalasia
diffuse oesophageal spasm
Scleroderma oesophagus with peptic stricture.
Management:-
endoscopically:-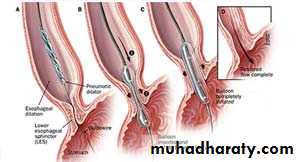
a. forceful pneumatic dilatation using 30-35 mm diameter fluoroscopically positioned balloon across the gastro esophageal junction. It improves the symptoms in 80% of pt. we face two problems:-
- Perforation of oesophagus in less than 3% may need surgical repair.
- Recurrent achalasia need frequent dilatation may improve with surgery.
b. botulinum toxin injection: under endoscope guided procedure to the lower oesophageal sphincter.
Advantage: - improvement of symptoms in 85%of pt.
Disadvantage:-
1. Symptoms relapse occur over 50% in 6-9 months although repeated injections give some improvement.It is not appropriate for elderly with multiple medical problems.
it is inferior for pneumatic dilatation and surgery.Surgery
Hurler’s operation:-either open operation or laparascopically.it improve the symptoms in 85 % of the patients
Complicated by GERD in 20%, therefore; partial fundoplication (antireflux surgery) is done.We need proton pump inhibitor drugs post operatively.
Causes of oesophageal stricture:-
GERDwebs and ring
CA oesophagus and or cardia.
Extrinsic compression from CA bronchus.
corrosive ingestion
post-operative scarring from oesophageal resection
post radiotherapy
Following long term nasogastric intubations.
Other causes of benign stricture


GERD, occur in elderly with poor oesophageal clearance.
Upper oesophageal ring (Plummer –Vinson syndrome) post cricoids web it is a rare complication of iron deficiency anemia, may be complicated by squamous cell CA.Lower oesophageal web (schatzki ring) causes intermittent dysphagia often starting in middle age.
Endoscope and dilatation is treatment of choice +treatment of original dis.
Oesophageal tumor
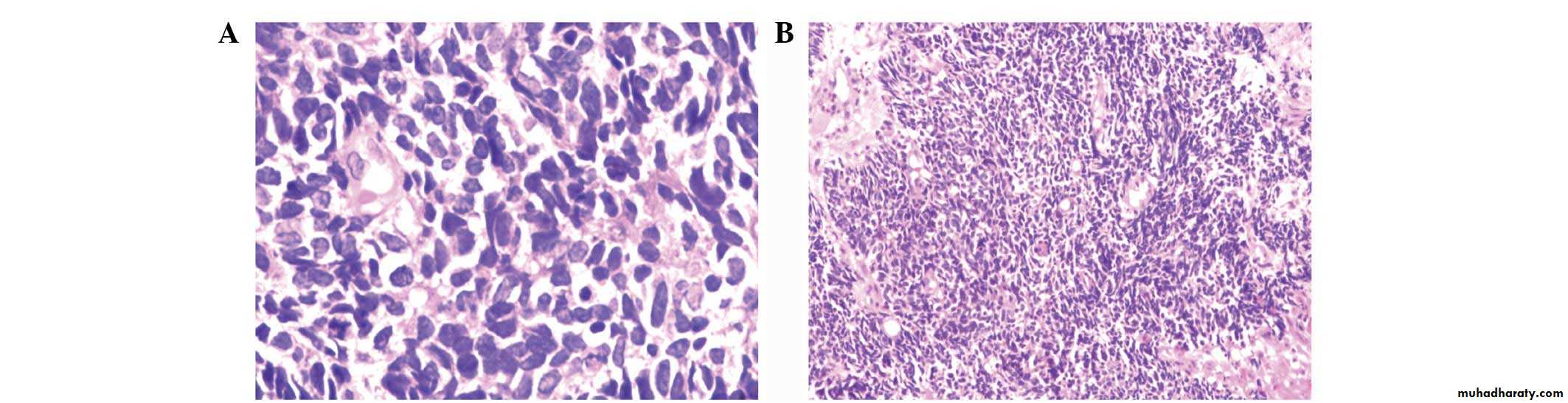
Basic classification of esophageal tumor:-Malignant - squamous cell carcinoma
-adenocarcinoma
- Melanoma
- Sarcoma (rarely leiomyosarcoma)
Benign
Leiomyoma
Adenoma
Cysts
Other said:- almost all are adenocarcinoma or squamous cell carcinoma ,small cell CA is rare third type.

Squamous cell carcinoma:-
It can occur from the cricoid cartilage to the cardia of the stomach. Almost all tumors above the lower third of the oesophagus are squamous cell CA.Etiology:-
Cigarette smoking, high alcohol intake, celiac dis, radiation, achalasia, ingestion of strong acids or alkali, environmental carcinogen, and possible reflux oesophagitis, Plummer-Vinson disease and palmer hyperkeratosis (tylosis palmaris).
Adenocarcinoma:-
This arises in the lower third of the oesophagus from barrette’s oesophagus or from the cardia of the stomach.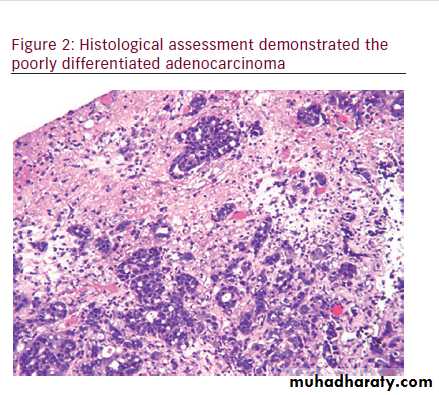
Clinical feature in all types :-
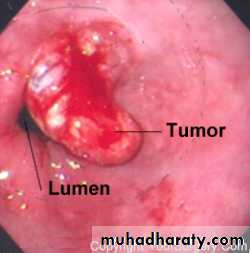
Most patients have a history of painless, progressive dysphagia for solid food or acutely because of food bolus obstruction. Dysphagia is usually rapidly progressive. Pain is usually retrosternal and is due to invasion into the mediastinum (hoarseness is also a symptom). Productive cough may reflex aspiration pneumonia or Broncho esophageal fistula (cough after swallowing)Weight loss is also obvious, anemia usually reflect bleeding or appetite depression, cervical LAP & hepatomegaly (metastasis) are a late symptoms.
Investigations:-
OGD
barium swallow
Chest x-ray and abdominal u\s to exclude metastatic lesion.
CT scan or MRI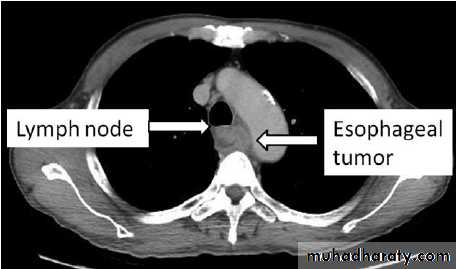
Endoscope is the most sensitive investigation.
Management:-
Approximately 70% of pt. has extensive dis. At presentation and treatment only to relief dysphagia and pain (palliative therapy) by:-laser therapy
insertion of stent
palliative radiotherapy to induce shrinkage of both adeno :&squamous CA
Nutritional support & analgesia.
The over all survival rate is less than 10% 5 years .survival rate depend on stage of tumor and type of CA. The overall survival following potential curative surgery (all microscopic tumor removed )is 30%at 5 years. But this can be improved by chemotherapy as cisplatinum and 5flurouracil.
The management of sq. cell CA is controversial because sq.CA is radiosensitive. Surgery or radical radiotherapy may be effective in patients who are fit, with no LN involvement or metastasis.
In the upper third, radiotherapy may be the preferred treatment as surgery is technically difficult procedure.
In the middle and lower third, surgery is preferred to radiotherapy if the patient is fit enough.
Surgery:-
the stomach is mobilized to the chest and anatomized to the oesophagus in the chest or
Colonic mobilization.
Radiation is complicated by oesophagitis and stricture.
Surgery is complicated by stricture, mediastinitis and anastomotic leaks.
Perforation of oesophagus
Causes: - iatrogenic by endoscope OGD either dilatation or intubations post malignant, corrosive or post radiotherapy stricture which need surgical therapy.Perforated peptic stricture is managed usually conservatively by antibiotics.
Spontaneous esophageal perforation (Boerhaave’s syndrome). Result from forced vomiting.Clinical picture:-
Chest pain, shocked subcutaneous emphysema, pleural effusion, and pneumothorax.Diagnosis:-

Water soluble contrast swallows CT or OGD under GA.
Treatment:-