Common infectious diseases
Roseola infantum
Also called (exanthem subitum or sixth disease)ETIOLOGY :
It is caused primarily by Human herpesvirus 6 (HHV-6A and HHV-6B) which is large double-stranded DNA virus & less commonly HHV-7.EPIDEMIOLOGY:
It is a disease of infancy. The peak age of primary HHV-6 infection is 6-9 mo of life.
- majority of children acquire infection from the saliva or respiratory droplets of asymptomatic individuals.
-Two mechanisms of vertical transmission of HHV-6 have been identified, transplacental infection and chromosomal integration.
CLINICAL MANIFESTATIONS :
*The incubation period 5–15 days .*It is characterized by the abrupt onset of high fever(38- 40°C), with irritability .
The fever usually resolves acutely after 72 hr. coincident with the appearance of a faint pink or rose-colored, nonpruritic rash (macules and papules) on the trunk.
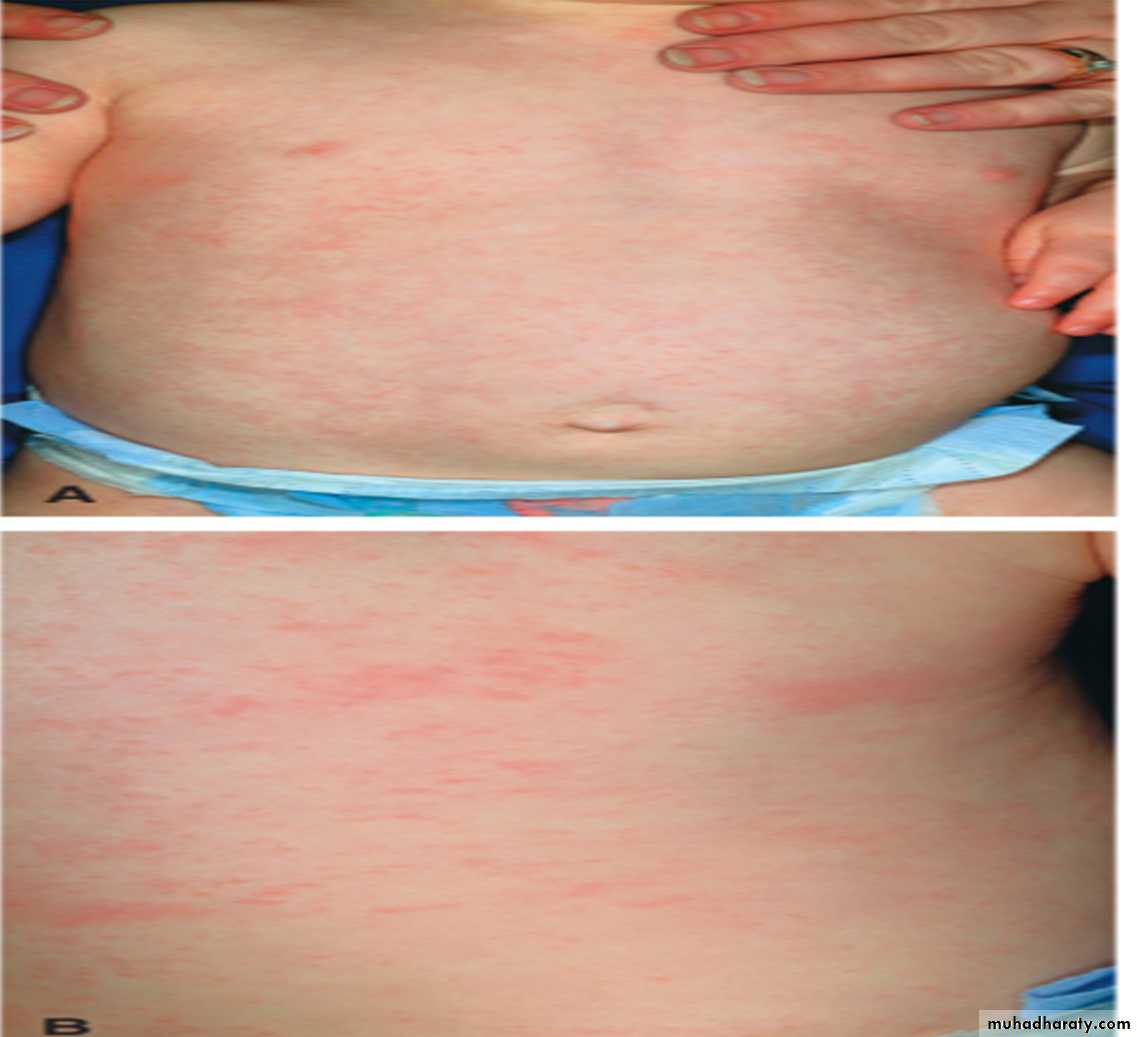
The rash usually lasts 1-3 days, spreading from the trunk to the face and extremities.
Febrile Seizures may occur in 5–10% of cases. Infrequent complaints include rhinorrhea, sore throat, enlarged suboccipital nodes, abdominal pain, vomiting, and diarrhea.
DIAGNOSIS:
1- clinical: age, history & clinical findings.2- Serological tests for HHV-6: early IgM antibody & later IgG antibody detection.
3- Virus culture
4- PCR
TREATMENT: Supportive which include adequate fluid intake & antipyretic.
Prognosis: excellent.Mumps
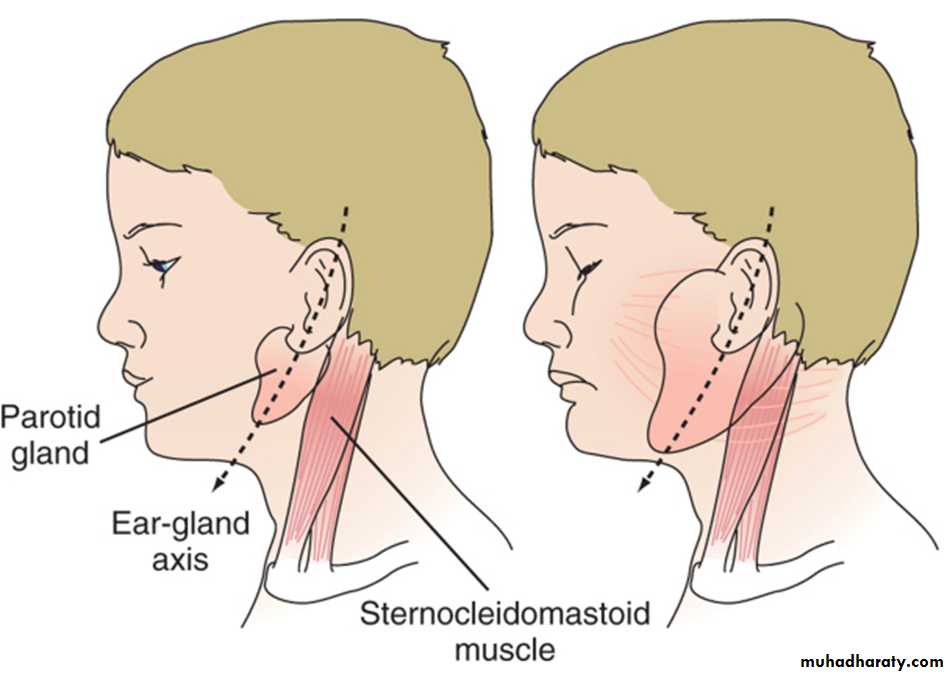
It is characterized by fever, bilateral or unilateral parotid swelling & tenderness .ETIOLOGY.
Mumps virus which is a single-stranded RNA virus.
EPIDEMIOLOGY:
- Mumps infection occurred more in the winter and spring months .
- most common in older children, adolescents, and young adults.
- spread from person to person by respiratory droplets.
- The period of maximum infectiousness is 1–2 days before to 5 days after parotid swelling.- Life long immunity follow clinical & subclinical infection .
PATHOLOGY AND PATHOGENESIS
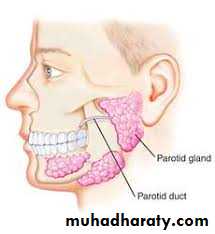
Mumps virus targets the salivary glands, central nervous system (CNS), pancreas, testes, and, to a lesser extent, thyroid, ovaries, heart, kidneys, liver, and joint synovia.CLINICAL MANIFESTATIONS :
- Incubation period is usually 16 to 18 days.- Prodrome lasting 1–2 days consisting of fever, headache, & vomiting.
Parotitis then appears and may be unilateral or bilateral in about 70% of cases .The parotid gland is tender with ear pain on the ipsilateral side.
Ingestion of sour or acidic foods or liquids may enhance pain in the parotid area.
There is redness & edema around opening of the Stensen duct.
The parotid swelling peaks in approximately 3 days then gradually subsides over 7 days. Fever resolves in 3 to 5 days .-Submandibular salivary glands may be involved. Edema over the sternum due to lymphatic obstruction may also occur.
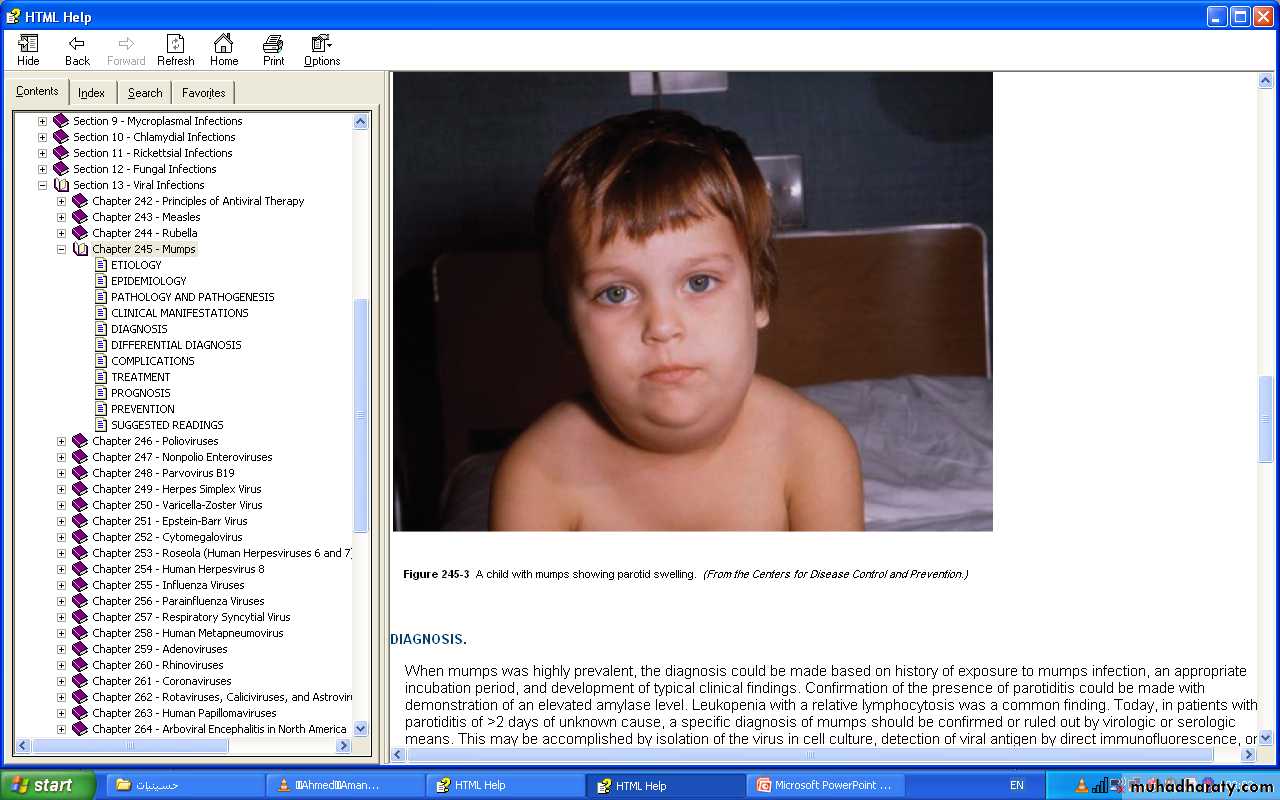

DIAGNOSIS :
1- clinical from history & examination .2- leukopenia & relative lymphocytosis .
3- elevated serum amylase level.
4- isolation of the virus by culture from saliva, CSF, blood & urine.
5- detection of viral antigen by direct immunofluorescence or polymerase chain reaction.
6- Serological test:
Detect mumps IgM & IgG antibodies.DIFFERENTIAL DIAGNOSIS :
1- other viral infections that cause parotitis as Cytomegalovirus, Epstein-Barr virus, and HIV.
2- Purulent parotitis :caused by Staphylococcus aureus ( unilateral, extremely tender, and associated with an elevated white blood cell count, and purulent drainage from the Stensen duct.
3- Submandibular or anterior cervical adenitis .
4- Noninfectious causes : obstruction of the Stensen duct, collagen vascular diseases such as systemic lupus erythematosus.COMPLICATIONS :
1- CNS complications:a-Meningitis and Meningoencephalitis.
b- Transverse myelitis, aqueductal stenosis, facial palsy & sensory neural hearing loss.
2- Orchitis & oophritis: orchitis is rare in prepubertal age, but common in adolescent & young adult. It may causing atrophy of the testes, but sterility is rare .
3- Pancreatitis. Some studies suggested that mumps may be associated with the subsequent development of diabetes mellitus.
Myocarditis
Arthritis ThyroiditisPneumonia
Nephritis Thrombocytopenia
TREATMENT:
No specific antiviral therapy is available for mumps.
Supportive care: 1-antipyretic for fever.
2- bed rest & analgesia for pain associated with orchitis.
3- adequate hydration.
PREVENTION:
*Isolation period of 5 days after onset of parotitis for patients with mumps.*MMR vaccine.
Diphtheria
ETIOLOGY:Corynebacterium diphtheriae
which is aerobic,
gram-positive bacilli of
3 biotypes
(mitis,gravis,intermedius).

EPIDEMIOLOGY.
*it is exclusive inhabitant of human mucous membrane & skin.*spread by airborne respiratory droplets, direct contact with respiratory secretions or exudate from infected skin lesions.
PATHOGENESIS :
*The major virulence of the organism is ability to produce exotoxin, which inhibits protein synthesis and causes local tissue necrosis & pseudomembrane formation .Toxin absorption lead to systemic manifestations like cardiomyopathy, and demyelination of nerves which occurs 2–10 wk after mucocutaneous infection
CLINICAL MANIFESTATIONS :
-Respiratory Tract Diphtheria:Incubation period: 2–4 days.
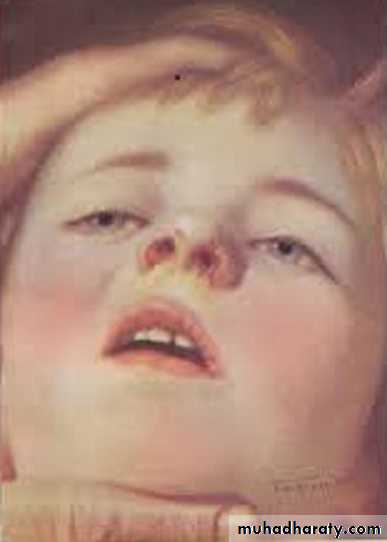
Infection of the anterior nares, which is more common among infants, causes purulent, erosive rhinitis with membrane formation. Shallow ulceration of the external nares and upper lip is characteristic.
*Tonsillar and pharyngeal diphtheria : sore throat is the universal early symptom. only half of patients have fever, and fewer have dysphagia, hoarseness, or headache
Underlying soft tissue edema and enlarged lymph nodes can cause a bull-neck appearance.


*Laryngeal diphtheria : Hoarseness, stridor, dyspnea, and croupy cough occurs .
They are at risk for suffocation because of local soft tissue edema and airway obstruction by the diphtheritic membrane which may require establishment of an artificial airway and resection of the pseudomembrane.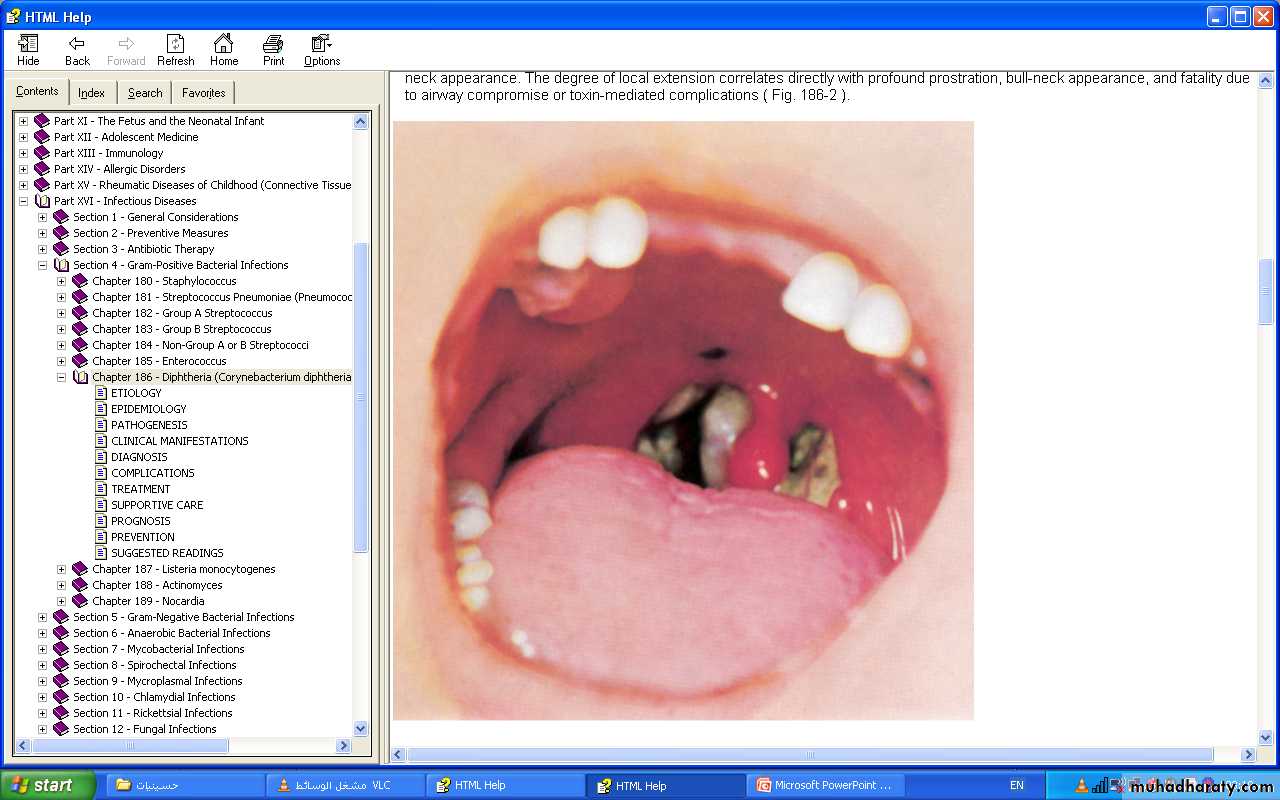


Cutaneous Diphtheria
Classic lesion is an indolent, nonprogressive infection characterized by a superficial, ecthymic, nonhealing ulcer.COMPLICATIONS :
1-Respiratory tract obstruction by pseudomembranes.
2-Toxic Cardiomyopathy.
3-Toxic Neuropathy.DIAGNOSIS :
-Specimens for culture obtained from the nose and throat and any mucocutaneous lesion .TREATMENT
1-Antitoxin: It is the mainstay of therapy and should be administered empirically as a single dose of 20,000–100,000 U based on the degree of toxicity. It neutralizes only free toxin.
2-Antimicrobial therapy :
Erythromycin (40–50 mg/kg/day divided every 6 hr PO, orcrystalline penicillin G (100,000–150,000 U/kg/day divided every 6 hr IV or IM), or daily Procaine penicillin (300,000 units/day IM for those <10 kg in weight; 600,000 units/day IM for those >10 kg in weight for 14 days.
Elimination of the organism should be documented by at least 2 successive negative cultures from the nose and throat (or skin) obtained 24 hr apart after completion of therapy.
3-Supportive treatment : isolation & bed rest during the acute phase & usually for 2 weeks .