
Fifth stage
ENT
Lec-4
د.سعد
5/10/2015
Chronic Sinusitis
Definition:
is defined as 8 weeks of persistent symptoms and signs of sinusitis that does
not respond to appropriate and aggressive medical therapy. In this case the long-standing
infection of the sinus will lead to irreversible change in the mucosa even when the original
cause of infection is removed.
The most commonly affected sinus
is the maxillary sinus because its osteum is
high and not gravity dependant.
Chronic Maxillary Sinusitis
Predisposing factors;
1) Nasal:
o Obstruction of the drainage ostia due
to long-standing blockage (with e.g.;
deviated nasal septum, nasal polyposis
and enlarged inferior turbinates).
o Recurrent acute infection leads to
chronic state.
o Chronic irritation from environmental
gases.
II
2) Dental
(10% of cases) The upper 2nd premolar and the 1
st
and 2
nd
molar (i.e. 5
th
, 6
th
and 7
th
upper teeth) impinge
closely on the floor of the maxillary antrum and may indeed penetrate it. Root infection or dental abscesses are
commonly the cause of unresolved maxillary sinus infections. The organism here are mainly anaerobes, and the
secretion is characteristically fetid . Healing of this form of sinusitis is impossible without dental treatment.
Pathology:
chronic sinusitis can be divided pathologically into
:
1. Chronic hypertrophic sinusitis: there is hypertrophy of mucosa due to increase vascular permeability.
2. Chronic atrophic sinusitis: (less common) there is generalized flattening of the epithelium due to
endarteritis obliterans of the arterioles.
Diagnosis:
Symptoms:
Major symptoms
Minor symptoms
Nasal discharge (copious greenish,
yellowish post nasal discharge)
Fever
Nasal obstruction (due to swelling of
inferior turbinate )
Halitosis (bad mouth odor )
Headache and facial pain
(due to
blockage of drainage ostea and build up
of secretion)
Anosmia( because air not reach the
olfactory region) and cacosmia (i.e.
unpleasant smell, due to chronic
odiferous sepsis).
In addition to the above symptoms, chronic irritation in side the nose may produce; vestibulitis due to
chronic use of handkerchief, nose bleeds, otitis media due to oedema of eustachian tube , granular
pharyngitis and chronic laryngitis.
Signs:
Examination is often unhelpful, but we may see;
o Generalized inflammation of the mucosa.
o Purulent secretion or crusts.
o If a vasoconstrictor is used to shrink the nasal mucosa, pus may be seen emanating from the middle meatus.
o Otitis media and granular pharyngitis may be present in the absence of any specific nasal symptoms.
III
Investigations:
1)Radiography:
X-Ray of paranasal sinus
is helpful in the diagnosis sinusitis (mucosal thickening, polyps and fluid level may present).
2)
CT scan:
Coronal CT scan provide most information about the osteo-meatal complex. Axial CT is indicated mainly for defining
disease in the sphenoid or frontal sinus.
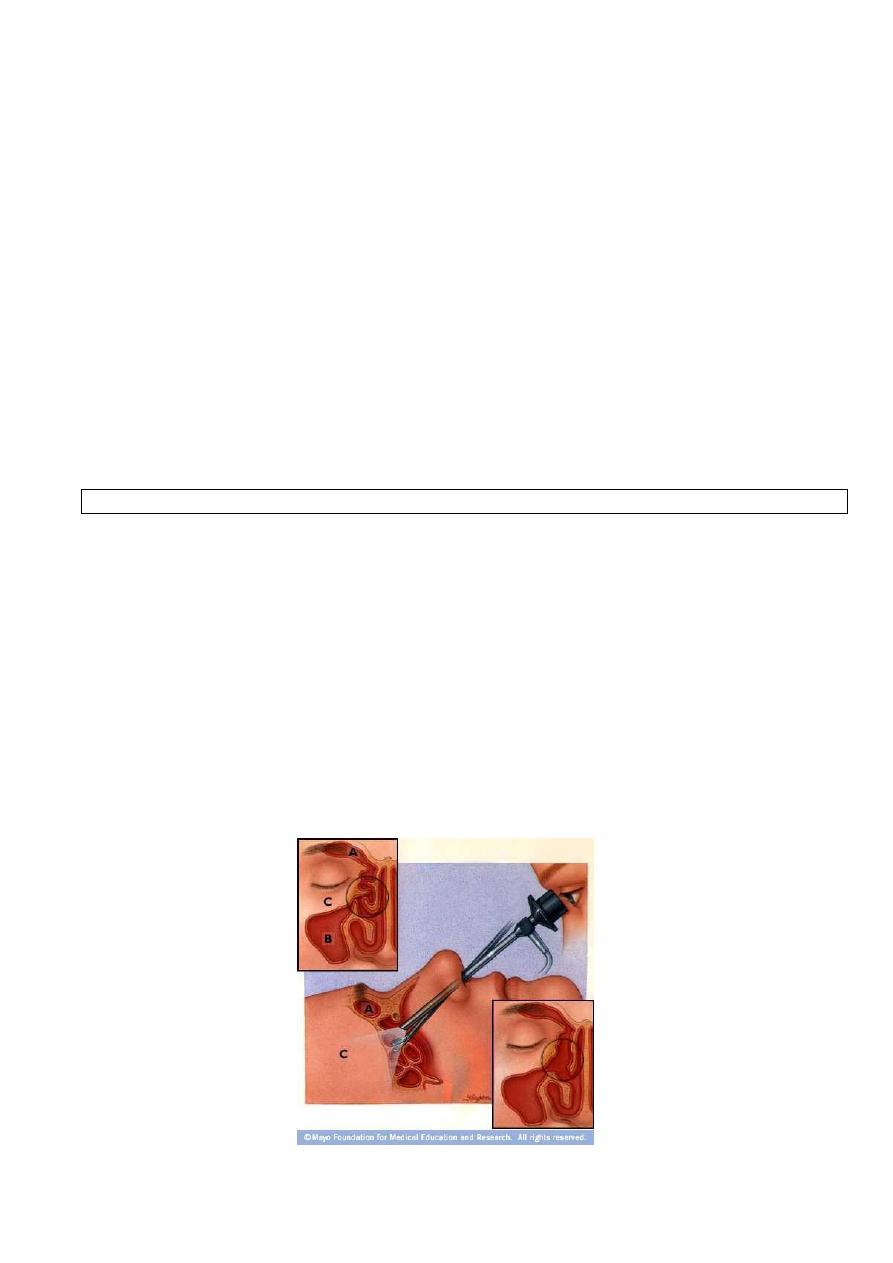
3) Endoscopic assessment
Endoscopic assessment has now become routine in the examination of the nose and paranasal sinuses.
There are several important features to be looked for;
a) The presence of pus in the middle meatus.
b)The cause of osteal obstruction
c) Sometimes biopsy is taken to confirm the diagnosis.
The key elements in the diagnosis are the history, the endoscopic assessment and the findings on coronal CT.
Treatment:
The principle of treatment is to restore the normal mucosa to the sinus lining. If this is not possible, i.e. when
the mucosa has been irreversibly changed, then the mucosa may need to be removed.
At the stage of chronic changes, medical treatment has been tried and is of no value.
Surgical treatments of the chronic maxillary sinusitis include;
1) FESS (functional endoscopic sinus surgery ) is considered nowadays as the procedure of choice for the
treatment of chronic sinusitis. The basic philosophy of FESS is to remove only the diseased areas in order to
relieve the obstruction and so restore natural sinus drainage, ventilation and physiology.
2) Antral lavage.
IV
3) Intranasal antrostomy.
4) Caldwell-Luc procedure.
Complication of chronic sinusitis;
Mucoceles:
Definition; A
mucocele
is a
mucous-containing cyst completely filling a sinus and capable of expansion. They arise
in order of frequency in the frontal, ethmoidal, maxillary and sphenoidal.
Aetiology;
polyps, trauma, tumours and previous surgery particularly in the frontal recess. Over 30 years can elapse
between the traumatic event and the clinical presentation of a mucocele.
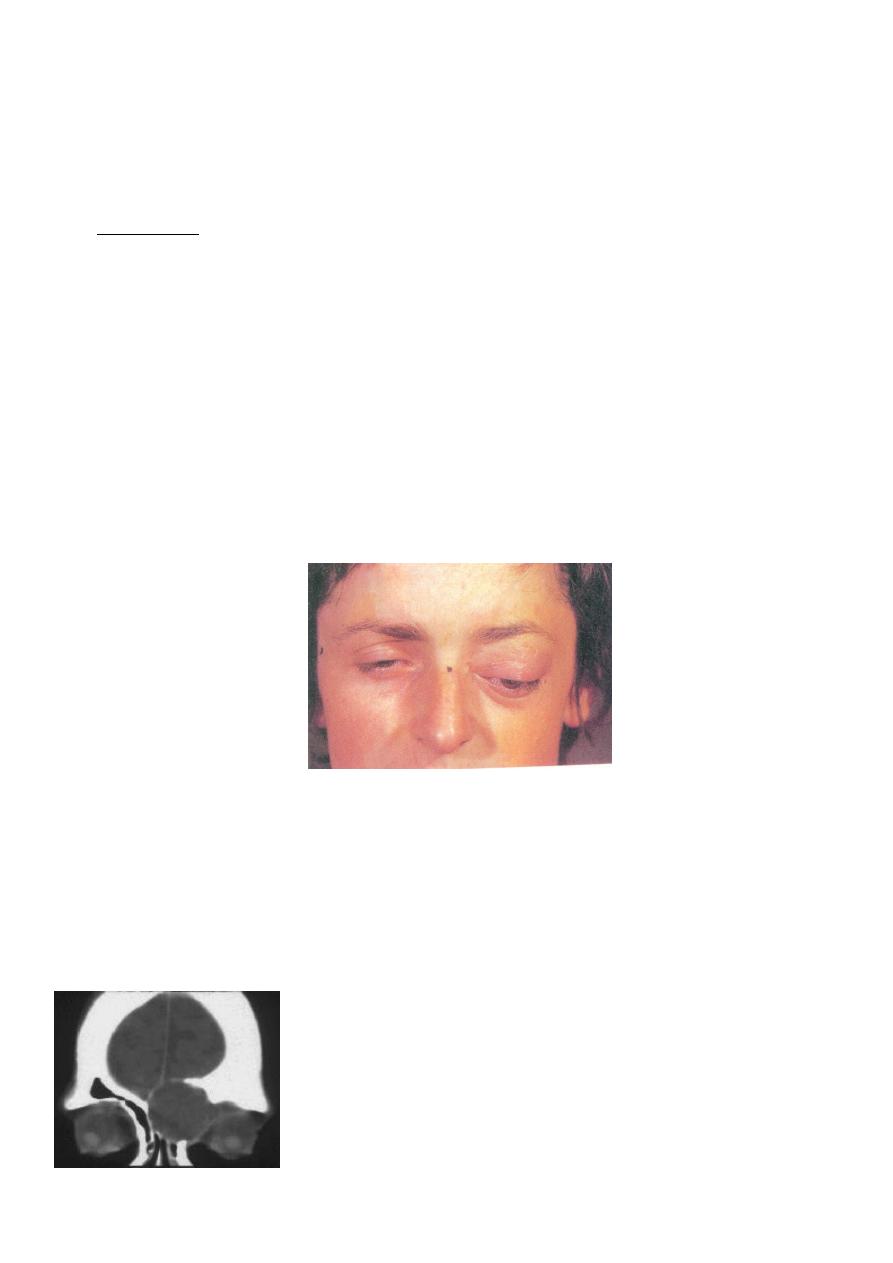
Frontoethmoidal mucocele
Clinical presentation
;
o In the early stages the patient is asymptomatic but, particularly in the frontal type, a dull ache develops and a
swelling appears at the supramedial aspect of the orbit.
o The swelling is tender and feels rubbery, not as firm a consistency as bone.
o Increase in size thins the bone more and pressure may damage the optic nerve or vasculature causing
blindness.
o If infection supervenes it is called a pyocoele and has more sinister consequences.
o With increase enlargement the eye may proptose.
Radiography of the sinus;
Thinning of the bone.
Displacement of the medial frontal sinus floor downwards.
Loss of scalloping of the superior border of the sinus.
The intersinus septum may be displaced or eroded.
CT scan is important in determining the anatomy and extent of the lesion.
V
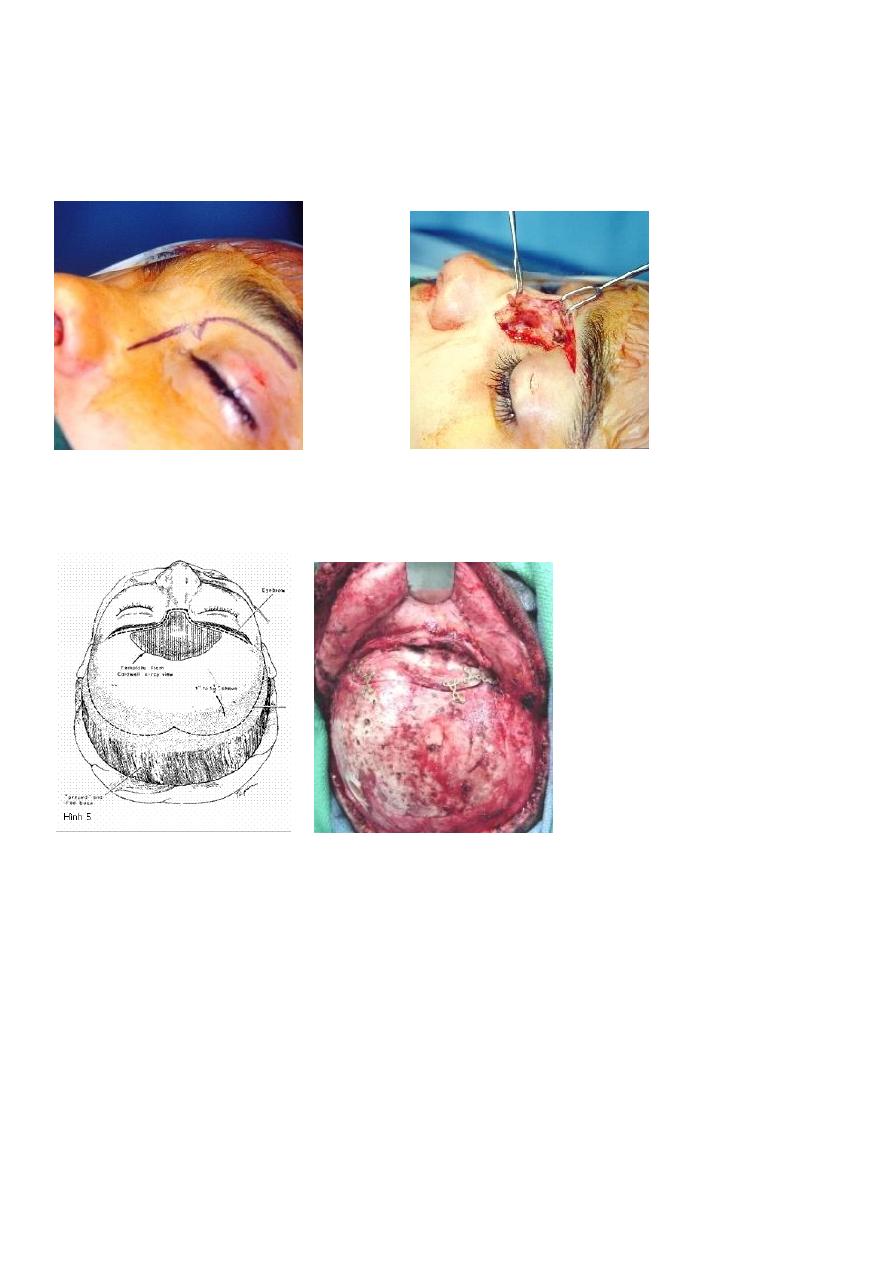
Treatment;
Is by evacuation of the contents of the sinus by ;
1) Endoscopic technique.
2) Radical frontal sinus operation.
3) Osteoplastic flap operation.
______________________________________________________
Tumors of the nose and paranasal sinuses
Tumors of the nose and paranasal sinuses can be subdivided into;
A.
Benign; e.g. Squamous papilloma (in the vestibule), osteoma (in frontal, ethmoidal and maxillary sinus),
Haemangiomas (on nasal septum) angiofibroma and inverted papilloma.
B.
Malignant tumours (uncommon); Squamous carcinoma is the most common followed by adenocarcinoma,
malignant melanoma, ethesioneuroblastoma, sarcoma and lymphoma. The maxillary sinus is the most common site
for development of malignancy.
VI
*Malignant tumours, unlike most of the other head and neck cancers, do not usually occur in heavy smoking or
heavy drinking population. They may occasionally result from exposure to environmental carcinogens (e.g.
adenocarcinoma in woodworkers)
* The chief symptoms of nasal malignancy are unilateral obstruction with haemorrhage (men > woman, average age
at presentation is 60)
*Tumours of the skin of the nose are probably the most common of the facial cancer.
Inverted papilloma
(Transitional cell papilloma or Schneiderian papilloma)
;
This lesion represents about 4% of all nasal neoplasms. It is the most common benign neoplasm of the nose
and sinuses.
Aetiology; unknown.
Sex; Male-female ratio 5-1.
Age; most commonly in the 5
th
decade.
Site of origin; lateral wall of the nose (occasionally from the septum) with extension to the ethmoid and maxillary
sinus.
Clinical presentation; Unilateral nasal polyp → unilateral nasal obstruction and sinusitis of all groups. The tumour is
soft and friable and may become detached or bleed with hard nose blowing.
X-Ray and CT scan of the sinuses; unilateral sinus opacity with bony erosion.
Histopathological examination; the surface of the tumour is covered by alternating layers of Squamous and columnar
epithelium, i.e. transitional type of epithelium.
The lesion is characterized by;
1) Being locally aggressive and causing bony erosion.
2) Tendency to undergo malignant change in about 2-5% of patient.
3) There may be coincidental malignancy elsewhere in the upper respiratory tract.
4) It has high propensity for recurrence after removal.
Treatment; by adequate local excision usually through lateral rhinotomy approach.
VII
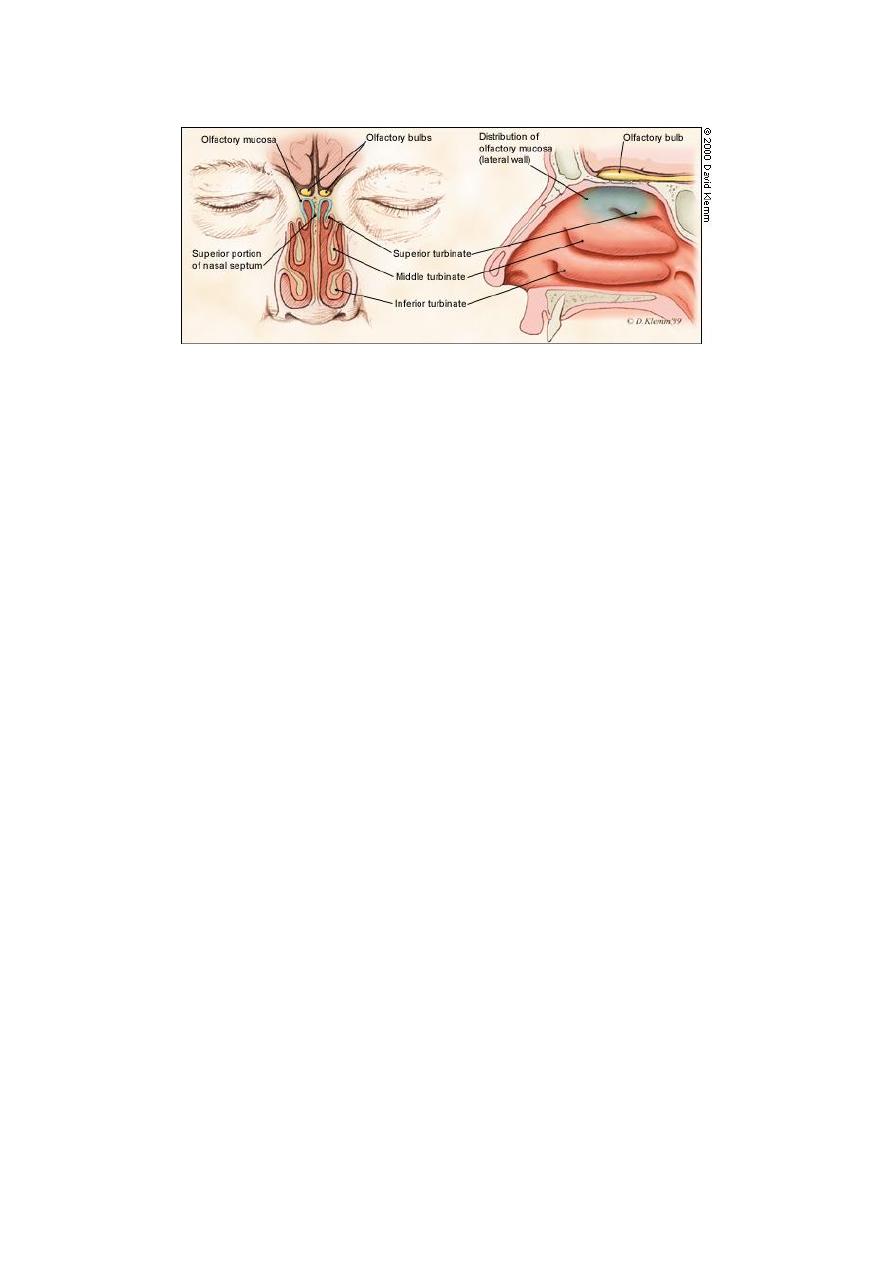
Disorders of smell
The olfactory cleft occupies the upper third of the nasal cavity in the area between the superior turbinate, cribriform
plate and corresponding area of the septum and is lined by specialized olfactory epithelium (this is a specialized
pseudostratified neuroepithelium containing the primary olfactory receptors and has a golden yellow color).
Terminology;
Anosmia; Inability to detect odors.
Hyposmia; Decreased ability to detect odors.
Parosmia; Altered perception of smell in the presence of an odor.
Phantosmia; Smelling of nonexistent odor.
(Both parosmia and phantosmia are associated with epilepsy and olfactory hallucination of schizophrenia).
Cacosmia; Unpleasant smell, due to chronic odiferous sepsis.
Classification of olfactory dysfunction:
1. Conductive anosmia; is due to impaired transport of airborne odorants to the olfactory cleft.
2. Neuronal anosmia; is due to impairment of olfactory epithelial function or disrupted neuronal
pathway.
Causes of olfactory dysfunction;
1. Obstructive nasal disease (23%): Include nasal polyposis, mucosal disease, tumours and nasal deformity.
2. Postviral anosmia (19%): Due to viral injury to olfactory epithelium and more common in those above age of
40.Hyposmia is more common than frank anosmia. About one third recover some function over 3-6 months.
No specific treatment
3. Head trauma (15%): Due to shearing force on olfactory filaments, olfactory bulb contusion or frontal lobe
injury.
4. Toxins, drugs (3%): Aminoglycosides, formaldehyde, alcohol, nicotine, organic solvents and direct application
of zinc salts.
5. Miscellaneous (21%): Aging, neoplastic, psychologic, nutritional deficiencies (e.g. vitamin A, thiamine) and
other causes.
6. Idiopathic (21%