د. محمد سامي 2013/10/24
Lec : 3Structural Abnormalities Chromosome Mutation;
Structural changes in chromosomes result from chromosomal breakage then loss or rearrangement of the materials.The mechanisms that can generate changes in chromosomes is the mutation
Types of structural abnormalities
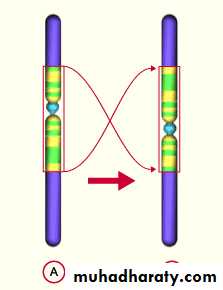
Translocation (t):
which implies transfer of a part of one chromosome to another.
Two types of translocation are identified:
Balanced reciprocal translocation is a term used when the entire broken fragments are exchanged (without loss). It is not harmful.

Robertsonian translocation, occurs between acrocentric chromosomes in most of which the breaks occur close to the centromere, affecting the short arms of both chromosomes. Transfer of the segments leads to one very large chromosome & an extremely small one which will be lost & the carrier will have 45 chromosomes. Such loss is compatible with survival.

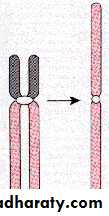
2. Isochromosomes
In which the centromere divides horizontally rather than vertically. One of the two arms is then lost & the remaining arm is duplicated resulting in a chromosome with either 2 long or 2 short arms only.
The most common isochromosome in live births involve the long arm of X-chromosome & is designated as i(Xq), when fertilized with normal gamete the result will be monosomy for genes on Xp & trisomy for those on Xq.
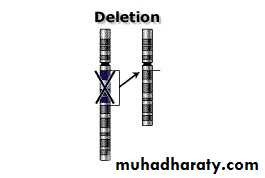
3. Deletion:
Involves loss of a portion of a chromosome. A single break may delete a terminal segment or two interstitial breaks which may result in loss of chromosome material between the breaks and reunion of the proximal & distal segments.Terminal (rare), result from single break in a chromosome arm producing a fragment with no centromere which is lost in next division.
Ring chromosome is a variant of a deletion, after loss of segments from each end of the chromosome, the arms unite to form a ring.
Ring chromosomes do not behave normally in meiosis or mitosis and usually results in serious consequences.

4. Inversion occur when there are two interstitial breaks in a chromosome, & the segment reunite after a complete turnaround. There are 2 types, pericentric and para-centric. It is often compatible with normal development

Inversions Pericentric Paracentric


Features of chromosomal disorders
Chromosomal disorders may be associated withAbsence (deletion or monosomy)
Excess (trisomy) or
Abnormal rearrangement (translocation, inversion)
Loss of chromosomal material produces more severe defects than gain.
Excess chromosomal material may result from complete chromosome (as in trisomy) or part of a chromosome (as in robertsonian translocation).
Imbalances of sex chromosome (excess or loss) are tolerated much better than similar changes of autosomes.
Sex chromosomal disorders often produce subtle abnormalities that are sometimes not detected at birth. Infertility which is a common manifestation cannot be diagnosed until adolescence.
Most of chromosomal disorders result from de novo changes (i.e. parents are normal & the risk of recurrence in siblings is low). An important exception is the translocation form of Down syndrome.
A-Cytogenetic disorders involving autosomes
Trisomy (21, 18, 13)Deletion (Cri du chat syndrome which involves chromosome 5).
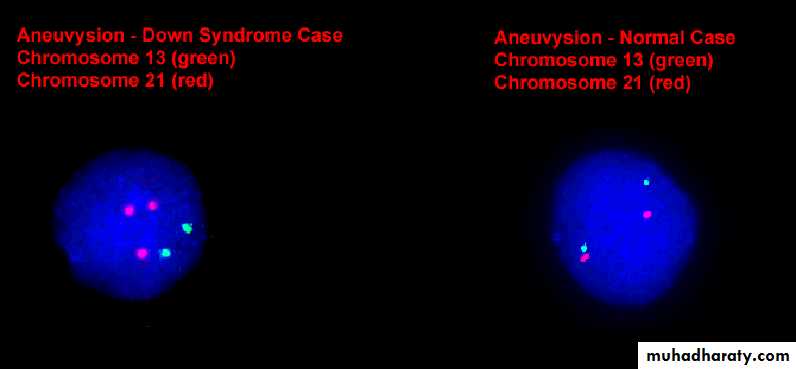
Trisomy 21 (Down syndrome)
It is the most common chromosomal disorder.
About 95% of affected persons have trisomy 21 (usually non-disjunction).
In 95%, the extra chromosome is maternal in origin.
The parents are normal in all respects.
Maternal age has a strong influence on the incidence which is 1 in 1550 live births in women < 20, in contrast to 1 in 25 live births in women > 45 years.
No effect of paternal age.
In 4%, the extra chromosomal material is present not as a trisomy but as a translocation of the long arm of chromosome 21 to chromosome 22 or 14. Such cases are usually familial.
Approximately 1% of trisomy 21 are mosaics, usually having a mixture of 47 & 46 chromosome cells. Symptoms in such cases are variable & milder, depending on the proportion of abnormal cells.
B-Cytogenetic disorders involving sex chromosomes
A number of abnormal karyotypes involving sex chromosomes, ranging from 45X to 49XXXXY, are compatible with life.
On the other hand males who are phenotypically normal may have two or even three Y- chromosomes.
Klinefelter syndrome
Defined as a male hypogonadism that develops when there are at least two X chromosomes & one or more Y-chromosomes.
Most patients are 47,XXY.
The extra X may be maternal or paternal.
Advanced maternal age & a history of irradiation of either parent may contribute to the condition.
Approximately 15% of patients show mosaic patterns including 46,XY/47,XXY, /48,XXXY & others. The presence of 46,XY line is associated with a milder form.
Turner syndrome (45,X0)
A primary hypogonadism in phenotypic females.
Results from partial or complete monosomy of the short arm of X-chromosome.
In 57% of patients, the entire X-chromosome is missing, resulting in 45,X karyotype. These patients are the most severely affected & can be diagnosed early in life.
C/ Disorders of multifactorial inheritance (polygenic)
Largest group among genetic disorders
Governed by the additive effects of two or more genes with a small effect & conditioned by environmental influences.
Involved in many physiologic characteristics of human like height, weight, blood pressure, hair color.
Features of multifactorial inheritance
The risk of expressing the disorder is conditioned by the number of mutant genes inherited. Also the greater the number of affected relatives, the higher the risk for other relativesThe rate of recurrence is the same for all first-degree relatives of the affected individual (between 2-7 %).
The risk of recurrence of the phenotypic abnormality in the subsequent pregnancies rises to 9% after 2 affected siblings.
The frequency of concordance for both identical twins is significantly less than 100 % (20-40%), but is much greater than the chance of nonidentical twins.
Expression of the disorder depends on when the combined influences of genes and environmental factors cross a certain threshold.
E.g. Hypertension, diabetes mellitus, gout, cleft lips, cleft palates and pyloric stenosis, congenital heart diseases, cancer.
D/ Single gene disorders with Non-Classic (Atypical) pattern of inheritance.
Four groups of diseases resulting from mutations affecting single genes do not follow mendelian inheritance.Diseases caused by triplet repeat mutations (e.g. fragile X syndrome, & myotonic dystrophy).
Diseases caused by mutations in mitochondrial genes.
Disease associated with genomic imprinting.
Disorders associated with gonadal mosaicism
Triplet repeat mutations:

CGGCGGCGGCGGCGG
GGCGGCGGCGGCGGCGGCGGCGGCGGFragile X syndrome
Characterized by a long repeating sequence of three nucleotides of X-chromosome.It is one of the most common causes of familial mental retardation.
Frequency of 1 in 1550 for affected males and 1 in 8000 of affected females
Clinically affected males have moderate to severe mental retardation.
The mutated gene is on Xq.
Where is the atypicality
Unlike patients with other X-linked recessive disorders, approximately 20% of males carrying the mutated gene are clinically normal.These carrier males can transmit the disease to their grandsons through their phenotypically normal daughters they are called "transmitting males".
Another peculiarity is the presence of mental retardation in 50% of carrier females.
These unusual features have been related to the dynamic nature of the mutation.
In normal population the number of CGG repeat in is small (within 29), whereas affected individuals have 230-4000 repeats.
Carrier males & females have premutations (characterized by 52-230 CGG repeats).
Risk of phenotypic effect, the risk depends on the position of the individual in the pedigree.
Brothers of transmitting males are at 9% risk of having mental retardation. Where as grandsons incur 40% risk. This is called Sherman paradox.
Anticipation, clinical features worsen with each successive generation