Ophthalmology
EyelidsAnatomy
The eyelid is the protective cover or the curtain o f the eye-ball
Composed of five layer :
1- Skin
2- Muscles; Orbicularis oculi, and Levator palpebral muscle
3- Sub-muscular layer
4- Tarsal plate forms the fibrous backbone of the lid
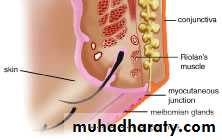
5- Conjunctiva; mucous membrane forms the inner lining layer
The margin of the lid
is 2mm muco-cutaneous junction,contains :
The lashes (Cilia).
Grey line
Orifices of Meibomian glands.
Mucocutaneous junction.
Superior and inferior puncti of Naso- lacrimal system.
Muscles of the eyelids:
1- Orbicularis oculi muscle:It is a thin oval sheet of concentric striated muscle fibers surrounding the palpebral fissure.
It can be divided into:
a- Peripheral (orbital) part: This is involved in forceful closure of lids.
b- Central (palpebral) part: This is involved in involuntary blinking and participates in forceful closure with the orbital part.
Nerve supply: Facial nerve.
2- Levator palpebrae superioris muscle:
It is originates from the periosteum covering the lesser wing of sphenoid bone at the apex of the orbit.
The aponeurosis inserts into:
a- Skin of the eyelids, so it forms skin creases on the eyelid.
b- Upper edge and anterior surface of the tarsal plate.
c- Medial and lateral palpebral ligaments.
Function: To keep the palpebral fissure open against gravity.
Nerve supply: Oculomotor nerve.
3- Superior palpebral muscle (Müller's or superior tarsal muscle):
It is a small sheet of smooth muscle originated from the under surface of the LPS muscle and inserted to the upper edge of the upper tarsal plate.
Nerve supply: Sympathetic nerves.
Function: Like LPS, is to keep the palpebral fissure open against gravity.
Glands in the eyelids:
Accessory lacrimal glands which contribute in the secretion of aqueous tear
Goblet glands, are unicellular glands which secret inner mucous layer of the tear film.
Meibomian glands are modified sebaceous glands embedded in the tarsal plates, about 20-30 in each lid. Meibomian glands secret the outer oily layer of the tear film.
Functions of the lids
Protection to the eye globe by blinking reflex.
Prevent dryness of the eye from continuous exposure.
Contributes in tear secretion; secrets oily layer of the tear film
Drainage of tear through the upper and lower puncti and canaliculi.
Spread tears over the anterior surface of the eye
Abnormalities in shape and position:
Trichiasis
Misdirection of the eyelashes which may cause irritation and ulceration of the cornea.
Causes : scarring to the lid margin e.g. trachoma, trauma, chronic blepharitis.
Treatment: For isolated misdirection cilia
a- Epilation: Repeated every few weeks.
b- Electrolysis: Destruction to hair follicles by cauterization.
c- Cryosurgery: Destruction to hair follicles by freezing.
d- Laser ablation: Destruction to hair follicles by laser.
Entropion
Inward inversion of the lid . Eyelashes cause rubbing and ulceration of the cornea.Causes
Congenital
Cicatricial conjunctivitis secondary to scarring of palpebral conjunctiva e.g. trachoma, chemical burn.
Senile; Due to weakness of Orbicularis oculi muscle .
Treatment : all of the above condition is treated surgically .
Spastic : secondary to any condition causing severe ocular irritation (irritation leads to overriding of Orbicularis oculi muscle fibers), e.g.: conjunctivitis, keratitis and ocular surgery. Treatment: of underlying cause and taping of lid (turned outward).
Ectropion
Outward eversion of the lid.
Misdirection of the lacrimal puncti cause
Tearing (epiphora)
Exposure conjunctivitis and keratitis
Causes
Congenital
Cicatricial; secondary to scarring of skin e.g. post-traumatic
Paralytic; facial nerve palsy. Treatment: we should wait for 6 months for spontaneous recovery e.g. (Bell's palsy) then lateral tarsorrhaphy is indicated.
Senile; Due to laxity of lower lid tendons. Treatment: surgical correction.
Ptosis
It is an abnormal low position or dropping of the upper eyelid. It could be unilateral or bilateral, and both of them could be partial or complete. Usually the upper lid covers only 2 mm from cornea. If more, is called blepharoptosis.
Causes:
1-Congenital, present at birth, may be unilateral or bilateral.Treatment : surgery .
2-Neurogenic :
Oculomotor nerve palsy
Causes complete ptosis, with impairment of eye movement
Sympathetic palsy (Horner syndrome)
Causes mild ptosis about 2-3mm dropping of the upper lid
3-Muscular :
Myasthenia gravis, impairment of transmission at the neuromuscular junction .Treatment :Medical.
Myotonic dystrophy
4- Aponeurotic blepharoptosis:
Weakness of the Levator palpebral aponeurosis (tendon)
i- Involutional (senile).
ii- Post operative.
5- Mechanical blepharoptosis:
Is the result of impaired mobility of the upper lid .
Dermatochalasis
Large tumour
Severe oedema
Heavy scar tissue
Lid retraction
Over-exposure of the eye, the sclera is exposed at the upper and lower limbus.It occurs most commonly in Dysthyroid Ophthalmopathy
6.Blepharospasm:
Involuntary sustained closure of the eyelids which occurs
spontaneously (essential)
sensory stimuli (reflex).
Inflammation of the lid
1.Stye (External hordeolum) :
Acute Staphylococcus infection of a eyelash hair follicle or one of the associated glands.
Clinical features; small tender swelling in the lid margin
Treatment;
a- Hot compresses
b- Topical antibiotics eye ointment
c- Epilation (removal of eyelashes by a forceps) to enhance drainage of pus.
d- Systemic antibiotics if there is severe preseptal cellulitis.
2. Internal hordeolum;
Acute Staphylococcus infection of a meibomian gland
Clinical features; tender hyperemic, swelling within the lid .
Treatment;
Topical antibiotics
Surgical drainage for the residual nodule after the acute infection has resolved.
3. Chalazion
Chronic lipogranulomatous inflammation of a meibomian secondary to retention of sebum and there is NO infection.
It is more frequent and multiple in patients with acne rosacea or seborrhoeic dermatitis
Clinical features; painless swelling within the lid .
Treatment
Surgical : The most common method
Steroid injection: Good alternative to surgery, 0.1-0.2 ml triamcinolone infiltrated around the lesion, the success rate is 80%. In unresponsive cases, another injection is given two weeks later. Chalazion should be small in size to be treated with steroid injection.
Systemic tetracyclines: As prophylaxis, particularly in acne rosacea and seborrhoeic dermatitis where chalazion is recurrent.
Blepharitis
Inflammation of the eyelid margin
Types of chronic blepharitis:
1- Anterior: a- Staphylococcal infection.b- Seborrheic dysfunction.
2- Posterior : meibomian gland dysfunction
Symptoms of chronic marginal blepharitis: (anterior and posterior)
Burning, grittiness, mild photophobia, and crusting and redness of the lid margin. The symptoms are characterized by remissions and exacerbations. The symptoms are usually worse in the mornings.
Signs of anterior blepharitis:
a.Seborrhoic
Clinical features; Redness of the lid margin, and presence of white dandruff like scales
b.Staphylococcal (Ulcerative)
Staphylococcus infection with purulent discharge, associated with chronic conjunctivitis and recurrent styes
Treatment:
Lid hygiene, with removing crusts and toxic products by washing the lids with weak solution of baby shampoo.
Short coarse of weak topical steroids
Topical antibiotics ointments in Staphylococcus infection
Tear substitutes
Oral azithromycin 500 mg daily for three days
Lid Tumors
Benign
Xanthelasma; yellowish slightly elevated plaque of lipid deposits
located medial aspects of both lids
Malignant
Basal cell carcinoma; elderly people, starts as well defined nodule, then the center becomes ulcerated and crusted