محمد الموسوي 12-10-2015 . د L.2
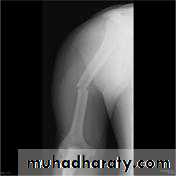
Fracture shaft of humerus:
Traumatic & pathological3-5% of all fractures
Bimodal age distribution
young patients with high-energy trauma
Elderly, osteopenic patients with low-energy injuries or due to 2ndary metastasis.
Fracture location: proximal, middle or distal third.
Fracture pattern: spiral, transverse, comminuted or oblique.

Clinical features:
Pain, bruises at site of fracture, radial nerve examination before &after treatment by extension of metacarpo-phalangeal joints.Holstein-Lewis fracture :
a spiral fracture of the distal one-third of the humeral shaft commonly associated with neuropraxia of the radial nerve (22% incidence due to entrapment of the radial nerve between fracture site),& need urgent open reduction & internal fixation with freeing of the nerve.
X-ray: to show types & site of fracture.
Treatment of humeral shaft fractures:
-Nonoperative
Splint for 7-10 days until pain &odema subside followed by functional brace (3-6) weeks, or using hanging cast from shoulder to wrist joint to pull the fragment in alignment with elbow 900 with sling to neck for 2-3 weeks replaced by functional cast for 6 weeks.


indications
gold standard and indicated in vast majority of humeral shaft fracturescriteria for acceptable alignment include:
< 20° anterior angulation
< 30° varus/valgus angulation
< 3 cm shortening
absolute contraindications :
severe soft tissue injury or bone lossvascular injury requiring repair
brachial plexus injury
outcomes
90% union rate
Operative treatment
Indications:
Severe multiple injuries
Open fracture
Segmental fracture
Displaced intraarticularextention of the fracture
Pathological fracture
Flowting elbow
Radial nerve pulsy after manipulation (Holstein-Lewis fracture )
Non-union
Type of fixation either by plate and screws or intramedullary nail(in closed fracture) while in open fracture using external fixation with antibiotic cover, ATS and wound debridement and later on either secondary suture of the wound or skin graft in case of skin and soft tissue loss.



Complications:
Early:Vascular injury (brachial artery injury)
Nerve injury
Radial nerve pulsy (wrist drop + paralysis of metacarpophalangeal joint extention)
Late:
1-Delayed union and malunion
2-Joint stiffness
Supracondylar fracture of humerus:
Supracondylar humeral fracture in children is one of the most common fractures seen in the pediatric orthopedic clinic setting worldwide. It's a fracture that occurs at the supracondylar area or the metaphysis of the distal humerus & accounts for 65.4% of upper extremity fractures in children .There are two types of supracondylar fractures in children according to direction of displacement of distal fragment i.e. extension type (97%) and flexion (3%).
X-ray of elbow joint (lat. View)
Mechanism:
The fracture is caused by fall on an outstretched hand in 70% of cases. As the hands hits the ground, the elbow is hyperextended resulting in fracture above the condyles. This fracture is most commonly seen in children between the ages of 5-15 yrs. There are two ways supracondylar fractures occur, high impact on a hyperextended elbow or a supracondylar flexion of more than 90 degrees. Fractures of the distal humerus are most commonly due to a falling on your hand with arms fully extended, causing direct trauma to the elbow. The distal condylar complex would shift in either the posterolateral or posteromedial direction, which account for approximately 95% of supracondylar fractures. The remaining 5% of these fractures result from a direct blow to the posterior aspect when the elbow is flexed more than 90°. In these cases, the distal condylar complex is more likely to displace in the anterolateral direction.
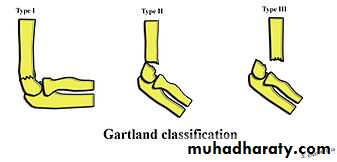
The Gartland classification is a system of categorizing supracondylar humerus fractures (extended type), clinically useful as it predicts the likelihood of associated neurovascular injury, such as anterior interosseous nerve neurapraxia or brachial artery disruption.
Type
DescriptionI
Non-displaced
II
Angulated with intact posterior cortex
III
Complete displacement
Presentation:
Presenting complaints: The child presents with history of a falling on an outstretched hand followed by pain, swelling and inability to move the affected elbow.
Diagnosis:
The fracture can however be difficult to identify and often a joint effusion is used to increase one's suspicion of the presence of a fracture. Upon examination the doctor will evaluate the arm for signs of damage to the nerves and blood vessels; they will look for swelling and deformity. This will allow the doctor to determine a likely diagnosis. Damage to the elbow is a common injury in children; injuries to blood supply of the arm may necessitate early surgical intervention. The radiographic study of the injured limb should include an anteroposterior (AP) and a lateral view.
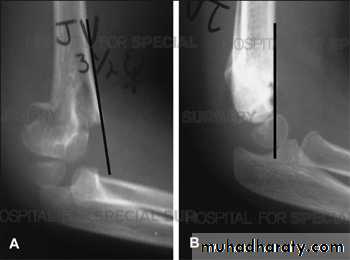
(AP) –view ( Lat.) –view
Treatment :-Nonoperative
long arm posterior splint then long arm casting with less than 90° of elbow flexion, typically used for 3-4 weeks and may be followed for additional time in removable long arm posterior splint .indications
Type I (non-displaced) fractures
Type II fractures that meet the following criteria
anterior humeral line intersects the anterior half of capitellum
minimal swelling presentno medial comminution
-Operative
closed reduction and percutanous pinning
indications
adequate reduction cannot be obtained by closed reduction (type II)
type III
more frequently required with flexion type fractures
immediate closed reduction and percutanous pinning
indications
vascular compromise is present (e.g, pale, cool hand)

Complications:
ischemic contracture (Volkmann contracture) due to damage / occlusion to the brachial artery and resulting in compartment syndromemalunion - resulting in cubitus varus (varus deformity of the elbow, also known as gunstock deformity)
damage to the median nerve or radial nerve or ulnar nerve.
Joint stiffness.
Lateral condyle fracture of humerus:
Fractures involving the lateral condyle of the humerus & account about 17% of all distal humerus fractures in the pediatric population,typically occurs in patients aged 5-10 years old,most commonly are Salter-Harris IV fracture patterns of the lateral condylemechanism of injury :
1-avulsion fracture of the lateral condyle that results from the pull of the common extensor musculature
2-fall onto an outstretched hand causes impaction of the radial head into the lateral condyle causing fracture
Classification
Milch Classification
Type I
Fracture line is lateral to trochlear groove
Type II
Fracture line into trochlear groove
Presentation
History
fall onto an outstetched hand
Symptoms
lateral elbow pain
mild swelling
Physical exam
inspection
exam may lack the obvious deformity often seen with supracondylar fractures
swelling and tenderness are usually limited to the lateral side
motion
may have increased pain with resisted wrist extension/flexion
may feel crepitus at the fracture site
Imaging
Radiographs
recommended views
AP, lateral, and oblique views of elbow
internal oblique view most accurately shows maximum displacement and fracture pattern .
optional views
contralateral elbow for comparison when ossification is not yet complete
CT scan indication --improved ability to assess the fracture pattern in all planes
Treatment
-Nonoperative : long arm cast with elbow at 90 degrees and forearm supination & weekly follow up ( total length of casting is 3-7 weeks )
indications only indicated if < 2 mm of displacement, which indicates the cartilaginous part intact
-Operative : open reduction & fixation by K-wire or screw.
Indications lateral condylar fractures with> 2 mm of displacement ,joint incongruity, fracture non- unionComplications
1-AVN : (Avascular Necrosis) due to posterior dissection can result in lateral condyle osteonecrosis may also occur in the trochlea2-Nonunion/malunion : caused from delay in diagnosis and improper treatment & may result in cubitus valgus and tardy ulnar nerve palsy


3-Tardy ulnar nerve palsy :slow, progressive paralysis of the ulnar nerve ,caused by stretching of the nerve, as is seen with cubitus valgus

Medial condyle fracture of humerus:
Failure to diagnose these injuries can lead to significant long term disability. Fortunately as these injuries involve an apophysis rather than an epiphysis, no growth arrest of the arm occurs, however elbow instability and even recurrent dislocations can result from suboptimal healing.Fifty percent of medial epicondyle fractures are associated with an elbow dislocation.It is important to distinguish a medial epicondyle fracture (common) from a medial condyle fracture (very rare). Medial condyle fractures are intraarticular, extending into the elbow joint and require urgent open reduction internal fixation (ORIF).


AP –view (displaced) (undisplaced)
Mechanismfall on outstretched arm :( most common)
elbow dislocation : associated with elbow dislocations in up to 50%
traumatic avulsion : usually occurs in overhead throwing athletes
PresentationSymptoms medial elbow pain
Physical exam
tenderness over medial epicondyle
valgus instability
X-ray : AP , lateral & oblique view also x-ray to other elbow to see ossification center & for comparism.
Treatment: - Nonoperative brief immobilization (3 to 4 weeks) in a long arm cast or splint in undisplaced fracture.
-Operative: open reduction internal fixation in displaced fracture with entrapment of medial epicondyle fragment in joint..
Complications
1-ulnar nerve injury
2-elbow stiffness
3-non-union