Dr.Bara'a Lukman Humo Al-Ibrahim FABOG/FIBOG/DGO
Hirsutism & virilismDefinition
Hirsutism is excessive growth of terminal (coarse) hair following a male like pattern in a woman.Latin hirsutus = shaggy, hairy
Not only it is a psychosocially distressing condition for many women, it may also be caused by certain potentially dangerous causes such as androgen producing tumours which need aggressive treatment.
Virilization:
refers to concurrent presentation of hirsutism with a broad range of signs suggestive of androgen excess, such as:
Severe acne or hirsutism or both,
Frontotemporal balding,
Deepening of the voice,
A decrease in breast size,
Clitorial hypertrophy,
Increased muscle mass,
Amenorrhoea/ oligomenorrhoea.
Epidemiology:
Hirsutism affect between 5% and 15% of women.Physiology of hair growth
There are three types of hair growth:
Lanugo hair is soft, unmedullated hair covering the fetus.
Vellus hair is short (2-5mm) and fine, lightly pigmented. Excessive growth of vellus hair produces a fuzzy appearance called hypertrichosis and is not associated with hyperandrogenism.
Terminal hair is long, dark and coarse and is affected by androgens giving hirsutism.
Types of hair
Lanugo Fetal hair .
Vellus ShortFine, Unpigmented Before puberty .
Terminal Long, coarse, pigmented arises from vellus hair
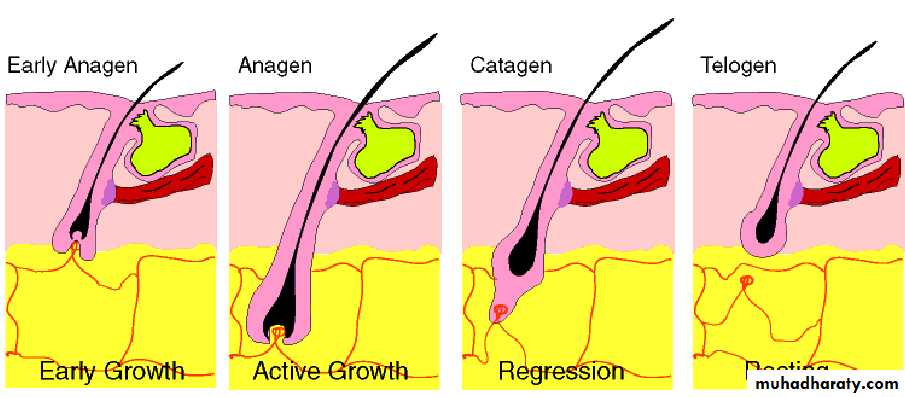
Hair growth is cyclical in three phases:
Anagen phase: the active growth phase.
Catagen phase: the transitional phase of arrested growth.
Telogen phase: the resting stage of the hair cycle, when it is shed.
This cyclical activity is generally scattered all over the body between all phases of the life cycle. The phases themselves last for varying lengths of time depending on the area of the body hair.
Cycle growth of hair
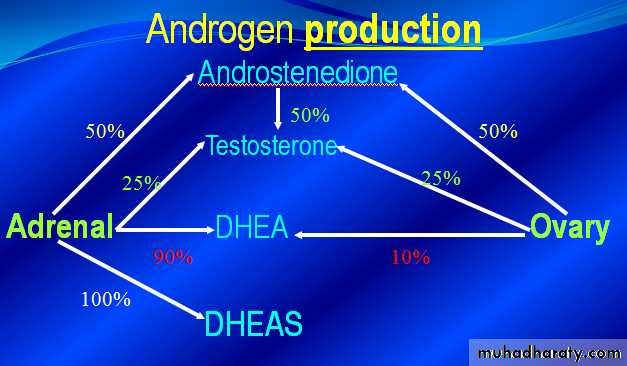
Androgen activity can be studied in three stages:
Androgen production by the adrenal gland and ovaries.Transport in the blood stream by sex hormone- binding globulin (SHBG) to the cell.
Binding to the receptor and intracellular modification.
Most circulating androgens are bound to SHBG. Only 1% of androgen circulate freely; these are the biologically active form. Thus, the affinity for SHBG determines the biological activity. Subsequently, a small change in the SHBG level causes a dramatic change in free circulating androgens.
5a- reductase (5aRA) fond in hair follicles and sebaceous glands, converts testosterone (T), androstenedione (AD) and dehydroepiandrosterone (DHEA) to dihydrotestosterone (DHT), the most biologically active androgen.
Peripheral 5aRA activity is increased by local growth factors and circulating androgens.
Progesterone competes with testosterone for 5a-RA. This may indicate why anovulation is more commonly associated with hirsutism.
In body hair, DHT stimulates;
Increased sebum production
The differentiation of the hair follicle from vellus to terminal hairs
The prolongation of the anagen phase resulting in longer and thicker hair
Hirsutism is a consequence of several factors. An increase in:
1. Androgen production2. The sensitivity of the androgen receptors at the level of the hair follicle.
3. The activity of 5œ-reductase.
Etiology
1. Adrenal Causes
2. Ovarian Causes
3. Exogenous Medications
4. Pitutary Causes (cushing’s disease, acrommegally, hyperprolactinemia)
5. Ectopic virilizing Tumors
6. Idiopathic or undetermined Causes :
A- minor dysfunction of the adrenals.
B- minor dysfunction of the ovaries.
C- more active 5- α-reductase enzyme.
D- Androgen receptors in the hair follicles are either large in number or oversensitive
A. Ovarian:
.PCOS: 90%
{hyperandrogenism, oligo-ovulation, PCO}
.Virilizing ovarian tumors
{arrhenoblastoma, hilus cell tumor, lipod cell tumor, granulosa cell tumor}
.Luteoma of pregnancy
{ Not true tumor but an exaggerated reaction of ovarian stroma to chorionic gonadotropins. It is solid, usually unilateral & regress after labour}
B. Adrenal:
Cong adrenal hyperplasia
Tumors
Cushing syndrome
D. Drugs
Hirsutism
Anabolic steroids
Danazol
Metoclopramide
Methyldopa
Phenothiazines
Progestins
Reserpine
Testosterone
Hypertrichosis
Cyclosporine
Diazoxide
Hydrocortisone
Minoxidil
Penicillamine
Phenytoin
Psoralens
Streptomycin
Clinical evaluation
The primary objective include:Grading the severity of the hirsutism using the modified Ferriman-Gallway scale.
Determining the source of the androgen excess.
Ruling out the rare but potentially life -threatening causes.
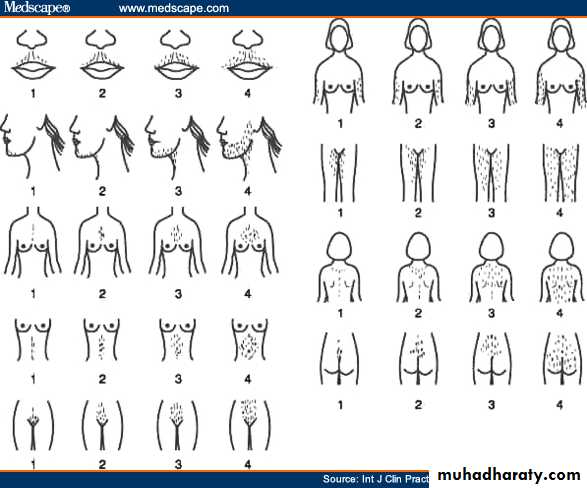
The Ferriman-Gallway score
Is a method of evaluating and quantifying hirsutism in women.
Hair growth is rated from 0 (no growth) to 4 (complete and heavy cover), in nine locations (upper lip, chin, chest, upper back, lower back, upper abdomen, lower abdomen, the upper arm and thigh), giving a maximum score of 36.
In white races, a score of 8 and above is considered indicative of androgen excess. In other ethnic groups, the amount of hair expected for that race should be considered.
History
.Onset & duration:Rapidly progressive virilization: androgen secreting tumors
.Menstrual history:
PCOS, Pregnancy
.Family history:
Hair patterns are similar in families
.Drug intake
Examination
General:Thyroid disease,
Cushing syndrome,
Signs of virilization,
Signs of insulin resistance e.g. acanthosis nigricans.
Breast: Galactorrhea {Hyperprolactinaemia can be accompanied by increase in adrenal androgen}
Pelvic: mass
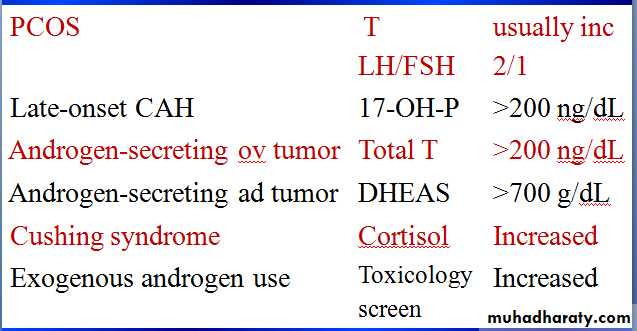
Investigations
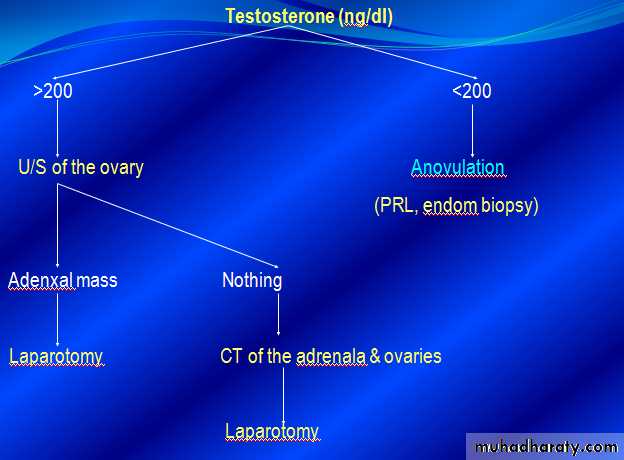
Initial laboratory investigation1.Total testosterone:
measures the ovarian & adrenal activity.
2.17 OHP:
an intermediate metabolite in steroidogensis in the adrenals.
3. DHEAS:
Good marker of Adrenal androgen production
Not essential
Evaluation of accompanying medical disorders:
Ovulation disorder :FSH,LHThyroid dysfunction:TSH
Hyperprolactinemia :PRL
Other investigations ( in selected cases)
Provocative tests : Corticotropin stimulation tests, Insulin resistance determination
Treatment
I. GeneralII. Specific
III. Local
IV. Surgery
I. General
Reassurance:
explain the condition, treatment regimen & the time required
Stop smoking
Weight reduction:
{Inc SHBG: Dec FT}
Keep BMI around 21 kg / m2
II. Specific
I. Ovarian suppression:
1. OCPs 2. Progestagen 3. GnRha
II. Adrenal suppression: Corticosteroids
III. Antiandrogens:
1. Spironolactone 2. Cyproterone acetate
3. Flutamide 4. Ketoconazole
IV. 5 alpha reductase inhibitors: Finasteride
V. Insulin sensitizer: Metformin
Oral contraceptive pills
Combined oral contraceptive pills, and in particular one containing the anti-androgen cyproterone acetate (Dianette ) are the most popular treatments for hirsutism. The new pill - Yasmin- is particularly helpful.
mechanism of action: the estrogen in the COCP:
Increase the estrogen level in the blood and this directly reduces hirsutism.
Increases the SHBG level and this reduces the amount of free androgen; the free androgen is largely responsible for hirsutism.
Suppress gonadotrophin (FSH&LH) from the pituitary. Reducing LH production results in lower level of ovarian androgen production.
Cyproterone acetate (androcure)
Dose:50-100 mg from D5 to D15 &
EE2: 30-50 ug from D5 to D25.
Decrease dose after remission
Mechanism:
is an anti-androgen; it competes at the receptor sites with androgens and reduces their effects.
progestational effect
Side effects:
menstrual irregularities, mastalgia, feminization of male fetus, loss of libido, fatigue, edema, weight gain, decrease HDLP & cholesterol, glucose intolerence.
Use with EE2 or OCPs
Dianette is a special combined oral contraceptive pill that contains 2mg cyproterone acetate.
Effects:
maximal by 3months improvement in 60-90%
Spironolactone:
Is an oral aldosterone antagonist with anti-angrogenic properties.
The most common dose used: 25-100 mg twice daily.
Side effects:
Menstual irregularities (metrorrhagia)
Urticaria
Mastodynia
Scalp hair loss
Nausea and fatigue can occur with high dose
III. Local
Suppress hair growth: Eflornithine Hydochloride (Vaniqa)Remove hair pigment: Bleaching
Temporary depilation: shaving, chemical depilators
Temporary epilation: plucking, waxing
Permanent removal: Electrolysis, Laser & intense pulsed light
Eflornithine Hydochloride (Vaniqa)
Eflornithine HCl (Vaniqa - Vaniqa is pronounced 'Vanika') 13.9% cream is the first topical prescription treatment to be approved by the US FDA for the reduction of unwanted facial hair in women.It irreversibly inhibits ornithine decarboxylase (ODC), an enzyme that catalyzes the rate-limiting step for follicular polyamine synthesis, which is necessary for hair growth.
In clinical trials eflornithine cream slowed the growth of unwanted facial hair in up to 60% of women. Improvement occurs gradually over a period of 4-8 weeks or longer. Most reported adverse reactions consisted of minor skin irritation.
Guidelines for management
1. The most desirable & effective tt is combination of OCP & antiandrogen.
2. Response is relatively slow, & at least 6 months are required to demonstrate an improvement.
3. Treatment should be continued for at least 1-2 yr.
4 There is no evidence that one agent is better than another & choices should be governed by cost & side effects.
5. The addition of GnRHa should be reserved for patients resistant to initial therapy.
7. Local methods should be used but reserved until hormonal therapy has reduced the rate of hair growth i.e. after 6 months.