INFECTION OF THE FEMALE GENITAL TRACT
At birth the neonate has been exposed to high level of estrogen &progesterone from her mother & vagina is lined with stratified squamous epithelium .In young female vagina is lined with a simple cuboidal epithelium .PH is neutral & it is colonized by organisms similar to skin commensals.
Under influence of estrogen at puberty stratified squamous epithelium develops & lactobacilli becomethe predominant organisms.
A drop in the PH occur to a level 3.5 to 4.5.
Following menopause atrophic changes occur with a return to bacterial flora similar to that of skin. The PH rises to 7.0
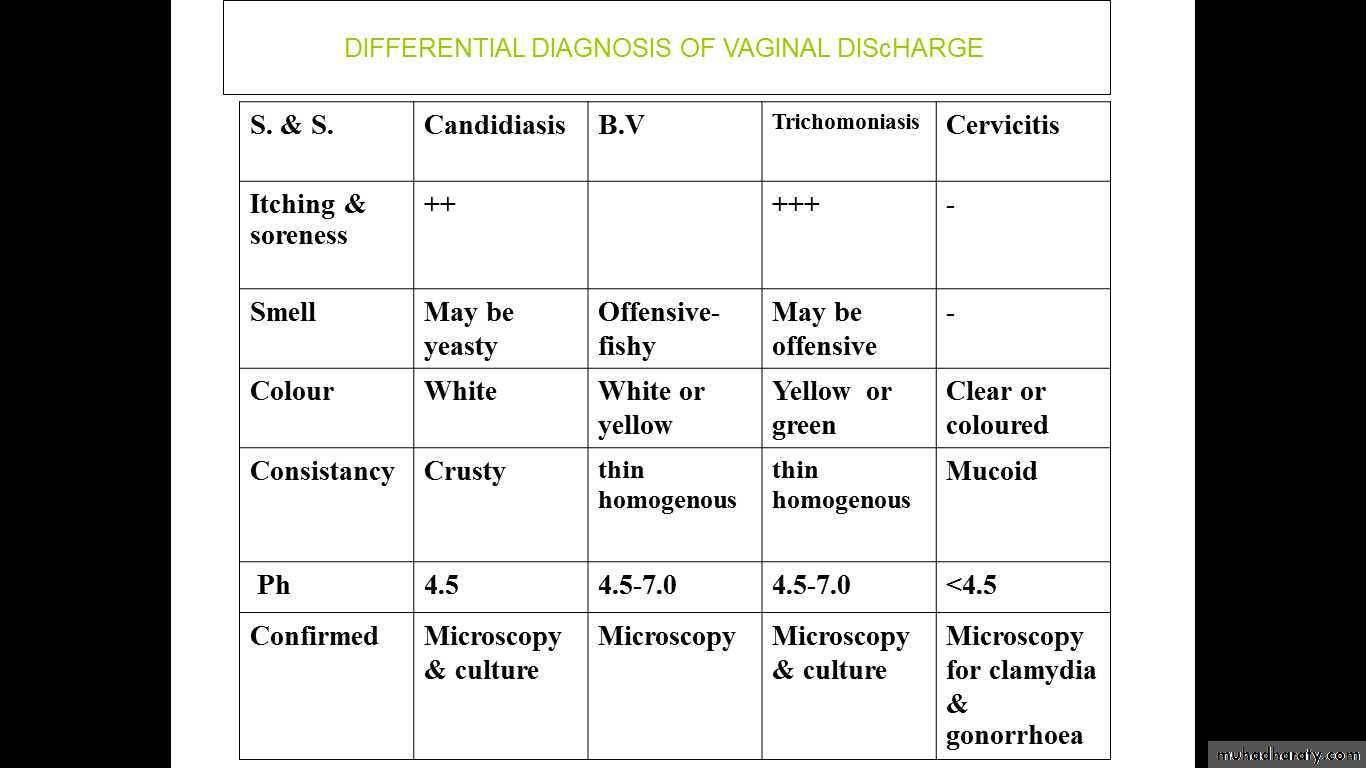
Vaginal discharge arising from the vagina can be physiological or pathological.
Physiological discharge
Normal vaginal discharge is white becoming yellowish on contact with air due to oxidation. It consist of desquamated epithelial cells from vagina & cervix , mucus originating from cervical glands, bacteria & fluid which is formed as transudate from vaginal wall.The acidic PH is maintaired by the lactobacilli through the production of lactic acid by vaginal epithelium metabolizing glycogen.
This discharge increase due to increase mucus from cervix in
mid-cycle
pregnancy
in women using COCP
Lower genital tract infection
1-candidal vulvovaginitis
Over three-quarters of women have at least one e episode of candidasis ,
the organism is carried in the gut, under the nails, in the vagina & on the skin#The microorganism
The yeast candida albicans is implicated in more than 80 percent of casesC. glabraba,C .krusei & C. tropicalis account for the rest
#The classical presentation
itching & soreness of vagina & vulva acurdy, white discharge which may smell yeasty but in some cases there may be thin watery discharge#On examination
Examination may be difficult because of tenderness , There is redress & inflammation of the vulval skin .when the discharge is removed the vaginal wall is red & inflamed .
#Diagnosis
depend onmicroscopy of wet preparations when candidal pseudohyphae or budding yeast mycelial threads are seen,
culture of vaginal fluid confirm diagnosis (> 10 yeast colonies).
PH of vaginal fluid is usually normal between 3.5&4.5.
#Predisposing factors
1- Increased oestrogen
- pregnancy
-COCP.
2- Underlying dermatosis e.g. eczema .
3-Broad –spectrum antibiotic therapy
4-Immunosuppression
- HIV
- Immunosuppressive therapy e.g. steroids.
5- Diabetes mellitus .
6-Vaginal douching ,tight clothing
#treatment
-local antifungal therapy
It is better to use topical treatment rather than systemic to minimize risk of systemic side effects
*single dose treatment clotrimazole 500mg
Nystatin pessaries 100.000 units for 14 days & nystatin cream is also applied to the vulva
-Oral therapy
may be used specially at time of menstruation , as single 150mg oral fluconazole.
In recurrent cases
-we should exclude diabetes and other predisposing factors
-we can give oral treatment as a once or twice a month for 6 months.
2-trichomoniasis
-This sexually transmissible infection
-can be carried asymptomatically,
-it can be carried in toilet articles from women to another ,
-cross-infection in antenatal & gynecological clinics may occur
-it causes vulvo vaginitis
-with purulent offensive yellow frothy discharge
-with irritation & soreness.
-The onset is sudden
-there may be history of previous attacks
-this infection usually seen during pregnancy
-It cause visible strawberry cervix
#Examination
-show yellow or green vaginal discharge which has unpleasent odour with
- inflammation of vulva, urethra & adjacent skin .
-The vaginal wall is intensively red & inflamed &
- numeraus minute punctate haemorrhages can occur on the vagina & cervix as strawberry spots.
#Diagnosis
It is confirmed by culture in specific media. Microscopy of vaginal discharge mixed
with seline has 60% sensitivity to detect the pear-shaped protozoon that can be recognized by its high motility with numerous leucocytes
#Treatment
Metronidozole is given orallyeither as 2 gram single dose or 400mg twice daily for five days ,
The partner should be given – same treatment .
3-bacterial vaginosis(B V)
-It is the commonest cause of vaginal discharge in women of child bearing age-It is not a STD and its Aetiology is unknown
-It is characterized by overgrowth of predominantly anaerobic organism like (Gardnerella vaginalis and Mycoplasma hominis) in the vagina.
-this leads to replacement of lactobacilli and an increase in PH from a normal 4.5 to 7
-It is more common in-black than white.
-and in smoker,
-and user of IUCD .
#Clinical features
*50% are asymptomatic .
*Symptomatic patient has offensive, fishy-smelling
*vaginal discharge, not usually associated with vulvovaginitis
*There is also thin, white, homogenous discharge coating the wall of vagina and vestibule
#complications
-Its incidence is high in patient with PID-Condition associated with post termination endometritis
-In pregnancy, it is associated with
1- late miscarriage
2-Preterm birth, preterm premature rupture of membrane, and post partum endometritis
-It is associated with vaginal cuff cellulites and abscess Formation following hysterectomy
#Diagnosis
The diagnosis is made using the composite (Amsel) criteria:-Vaginal PH>4.5
Release of fishy smell on addition of alkali (10% of potassium hydroxide).
Characteristic thin, white, homogenous discharge on examination .
Presence of clue cells on microscopy ( vaginal epithelia cells so heavily coated with bacteria that the border is obscured).
In addition to this criteria
Gram –stained vaginal smear show large number of Gram-positive &- negative cocci with reduced or absent large Gram-positive bacilli (lactobacilli)
#treatment
-avoid vaginal douching and use of antiseptic bath agents
-antibiotic treatment is recommended for symptomatic women,those undergoing surgical procedures, and some pregnant Women-recommended regimen is oral metronidazole 400-500 mg twice daily for 5-7 days or 2 g single dose
-alternative route is the vaginal one, intravaginal metronidazole 0.75% once daily for 5 days or clindamycin cream 2% once daily for 7 days
#Pregnancy& bacterial vaginosis
-All symptomatic pregnant women with bacterial vaginosis should be treated-also asymptomatic pregnant women with previous history of preterm birth or second trimester loss may be screened and treated.
Other causes of vaginal discharge
Atrophic vaginitis
bartholin abscess
Vaginal discharge in children
Vaginal discharge in children
Common conditionStreptococcal infection is the most common one
Recurrent infection may be due to foreign body
Entrobius vermicularis migrate at night and cause itching and irritation
Atrophic vaginitis
Is common in post menopausal women in whom.Vaginal epithelium atrophies& lactobacilli replaced by skin commensal organisms lead to vaginal soreness
the treatment is with oestrogen replacement .
Ocasionally true bacterial vaginitis is countered due to strentococci or other microorganism.
Bartholin abscess
Bartholin's gland situated on either side of the vagina and opening in the vestibuleBartholin's cyst can present as painless swelling if gland duct opening closed, and if infected becomes abscess and present as tender mass near lower part of vagina need
surgical treatment by marsupalization