
1
Gynecology
.د
س
مير
Lec-1
Ultrasonography in Gynaecology
Introduction
Ultrasound was first introduced by Ian Donald (Glasgow 1950) in the field of medicine
Sonography is widely used in Gynaecology either with the transabdominal (TAS) or with
the transvaginal (TVS) probe
Because of the safety, high patient acceptance and relatively low cost, ultrasonography
has become a common diagnostic modality in gynaecology these days.
Use of Ultrasound in Gynaecology
Use of infertility workup
o Serial measurement of ovarian follicular diameter (folliculometry) and endometrial
thickness are done using TVS.
o Ultrasound can provide presumptive evidence of ovulation. Following ovulation,
internal echoes appear and free fluid is observed in pouch of Douglas.
o To detect correcting time of ovulation by folliculometry in conjuction with plasma
oestradiol.
o Sonographic guided oocyte retrieval in IVF and GIFT programmes.
Ectopic pregnancy can be detected on TVS as a “tubal ring” separate from the ovary in
a patient with empty uterine cavity.
Pelvic mass can be evaluated as regard to its location and consistency. Uterine fibroid,
ovarian mass, endometrioma, tubo-ovarian mass, etc. can be delineated when there is
confusion in clinical diagnosis.
Oncology: TV-CDS can assess the vascularity of the mass. Low flow impedance with a
high flow velocity raises the suspicion of a malignant tumor.
Endometrial disease: Women with unexplained uterine bleeding, or postmenopausal
bleeding .
Transabdominal sonography
Is done with a linear or curvilinear array transducer operating at 2.5-3.5 MHz.
TAS requires full bladder to displace the bowel out of pelvis.
Other wise gas in the bowel acts as a complete barrier to ultrasound waves.
2
TAS is best used for large masses like fibroid or ovarian tumor
Higher is the frequency of ultrasound wave, better is the image resolution but lesser is
the depth of tissue penetration
Transvaginal Sonography (TVS)
It is done with a probe which is placed close to the targt organ.
Preparing patient
There is no need of a full bladder
It also avoids the difficulties due to obesity, faced in TAS
Transvaginal ultrasound may be done for the following problems:
Abnormal findings on a physical exam, such as cysts, fibroid tumors, or other growths
Abnormal vaginal bleeding and menstrual problems
Certain types of infertility
Ectopic pregnancy
Pelvic pain
TVS operates at a high frequency (5-8 MHz).
Therefore, detailed evaluation of the pelvic organs (within 10 cm of the field) is
possible with TVS.
But the drawbacks of TVS are mainly due to narrow vagina as in virgins,
postmenopausal women or post radiation vaginal stenosis.
3
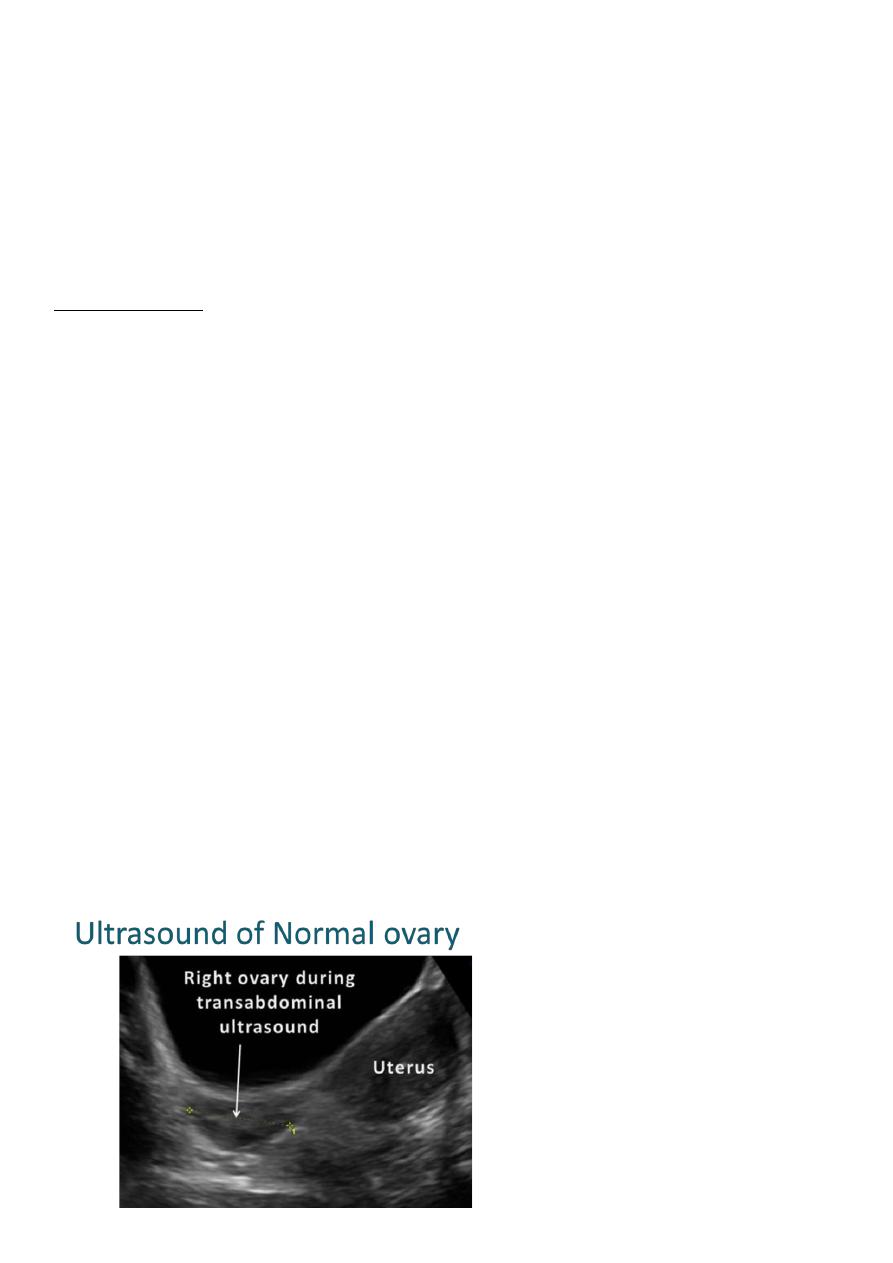
Normal Ovary
Normal ovary during a natural menstrual cycle demonstrating
normal follicle population and distribution on day 12
postmenstruation. A dominant follicle is visualized in the
central portion of the image and several subordinate follicles
from the wave (2–5 mm) are observed in the left lateral
aspect of the ovary.
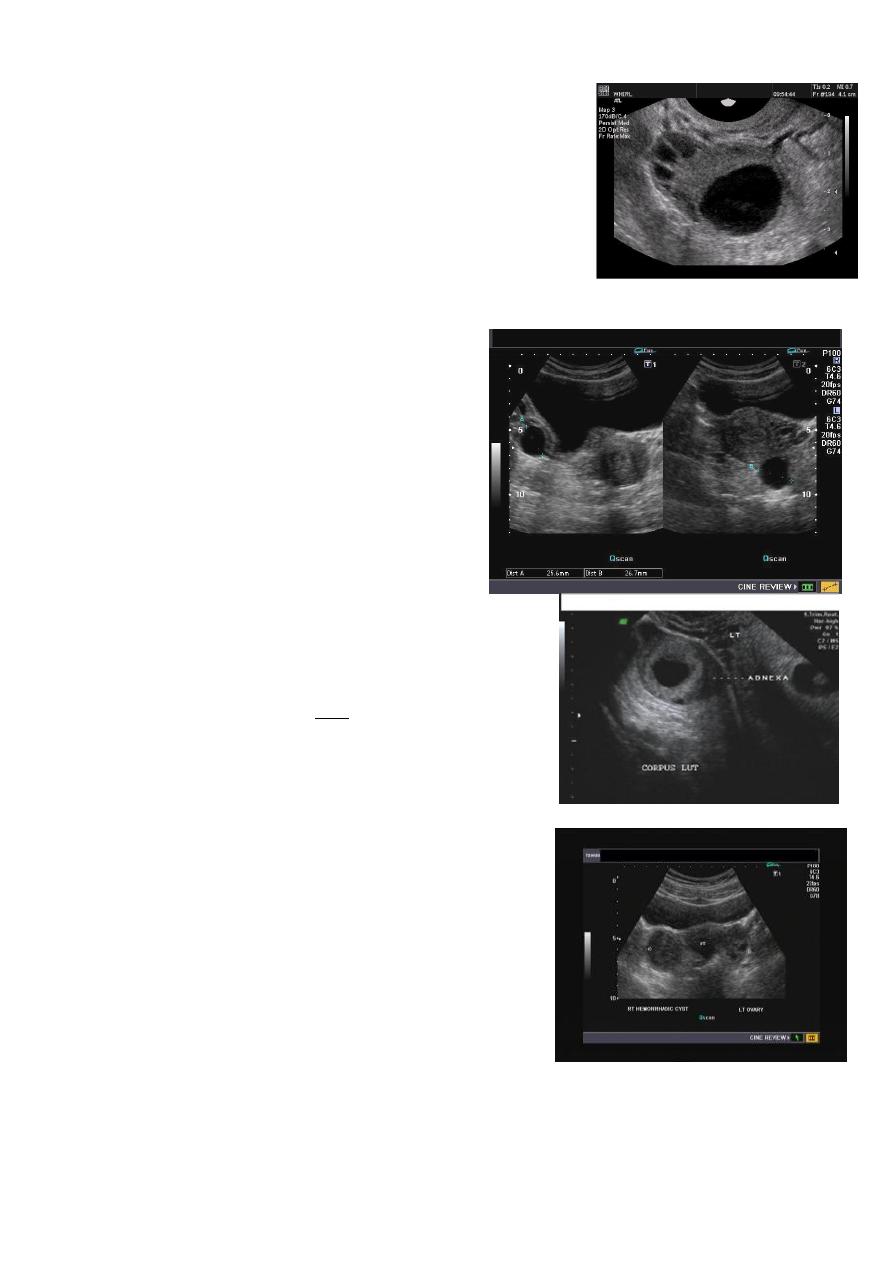
Functional cysts of the ovary - Follicular cysts:
This young female patient underwent
sonography for non-specific pain in the lower
abdomen. Ultrasound images of the pelvis show
bilateral ovarian cysts which show absence of
internal nodules, septae or debris. These findings
are typical of follicular cysts of the ovaries.
Follicular cysts are functional cysts and are
enlarged ovarian follicles that have not ruptured
(ovulated). They are usually unilateral.
Functional cysts of the ovary – Corpus Luteum cysts
Lt. adnexal cystic mass- Luteal cyst(Lt. ovary):
Hemorrhagic ovarian cysts:
Hemorrhagic cyst of ovary resulting from Ovulation
induction
This young nulliparous female patient undwerwent
ultrasonography following ovulation induction. The right
ovary shows a typical hemorrhagic cyst formed from the
corpus luteum. The first image (top row- left) is a
transabdominal ultrasound image showing fine fibrinous
strands within the cystic mass in the right ovary.
Transvaginal ultrasound and color Doppler images confirm these findings. The uterus shows
typical secretory changes in the endometrium suggesting post ovulatory phase.

4
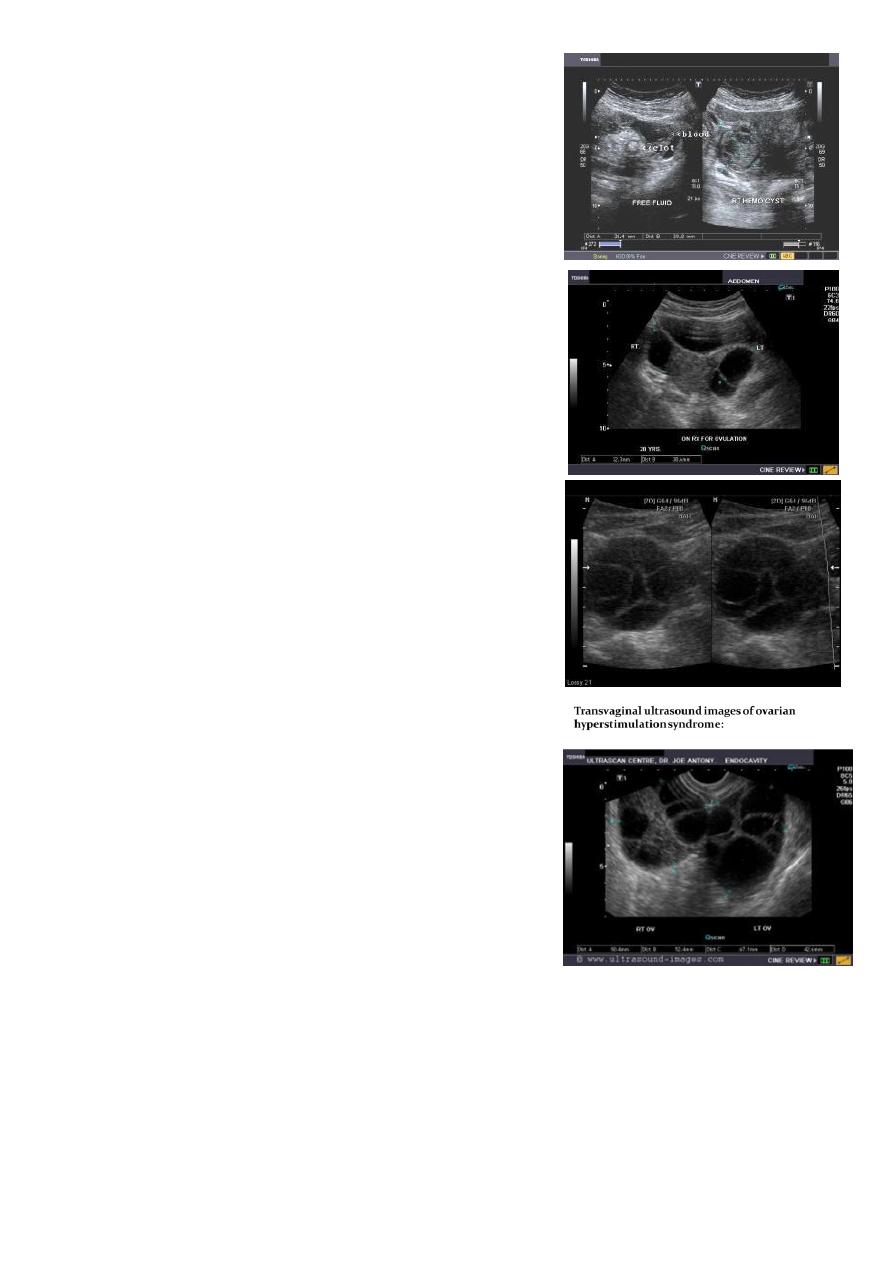
Hemorrhagic ovarian cysts:
Hemorrhagic cyst of ovary with co-existing chocolate cyst/
endometrioma:
This patient has a co-existing chocolate cyst with a
hemorrhagic cyst in the same (right) ovary. The cyst on the
left half of the ultrasound image is a hemorrhagic cyst.
Note the fine fibrinous strands within the cyst suggesting
clot formation. The cyst on the right half of the image is homogenous with fine echoes
throughout the ovarian cyst. This is a typical appearance of an endometrioma (chocolate
cyst)
Hemorrhagic ovarian cysts:
Hemorrhagic cyst of ovary with ruptured ectopic
pregnancy:
This female patient has a left ovarian hemorrhagic cyst
(see ultrasound image above-left). In addition, there is a
large collection of free fluid with particulate matter in the
pelvis. The right fallopian tube is thickened with a ring
shaped mass. This suggests that there is significant
hemorrhage into the pelvis due to a ruptured ectopic
pregnancy (right tubal ectopic gestation). The left ovarian
hemorrhagic cyst appears intact, ruling out ruptured hemorrhagic cyst.
Ovarian dermoid cyst or Cystic teratomas:
These ultrasound images reveal bilateral ovarian
complex masses that contain both solid and cystic
components. The right ovary shows a cystic mass
with a solid, highly echogenic "dermoid plug". This is
a solid nodule containing fat and various tissues
including hair. Posterior acoustic shadowing is seen.
The left ovary shows a dermoid plug and, in addition, a "dermoid mesh" is also seen, an
irregular echogenic solid mass within the cyst. Echogenic debris is seen floating within the
fluid
5
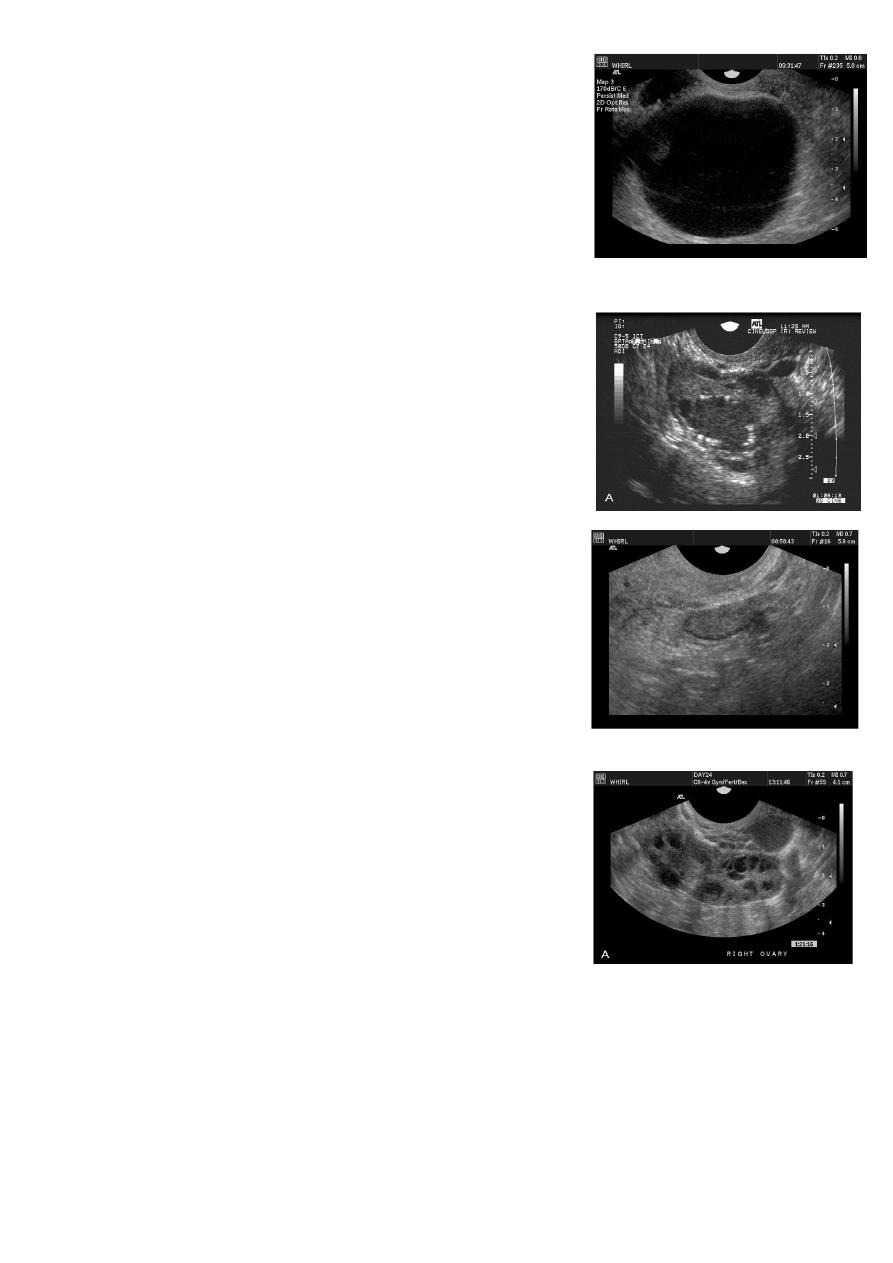
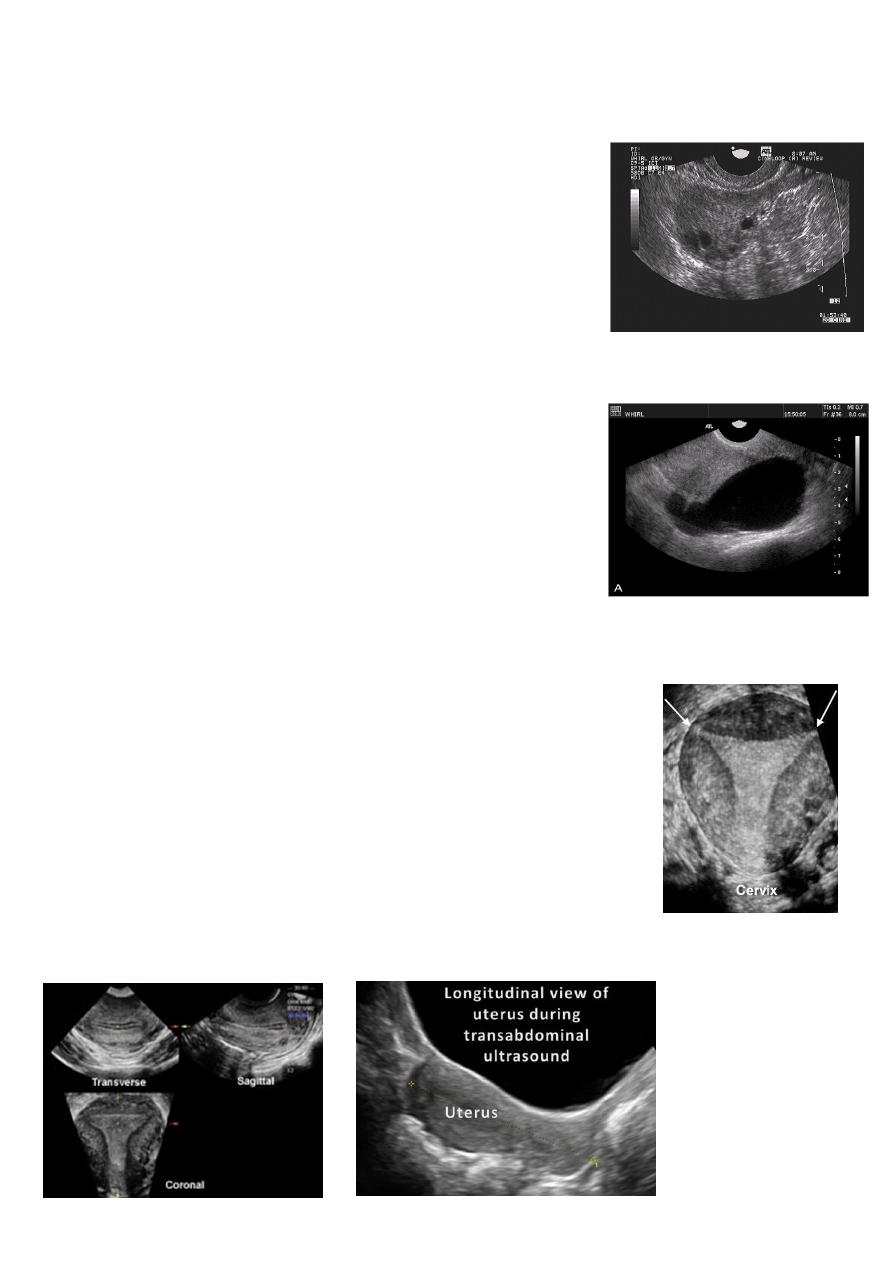
Rupture of hemorrhagic ovarian cyst:
Transabdominal scanned image
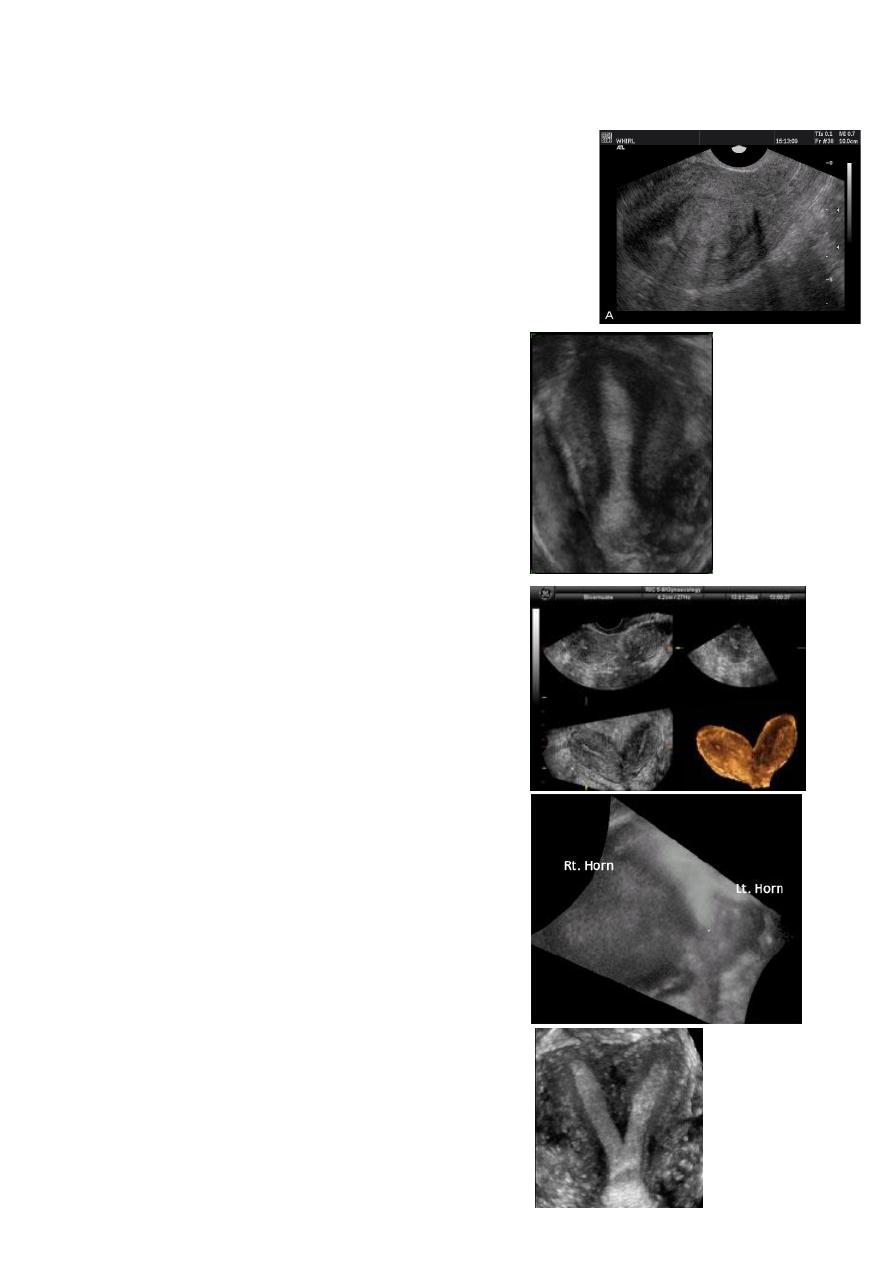
Ovarian hyperstimulation syndrome (OHSS):
This young adult female patient was examined to
evaluate the uterus and ovaries. She was under treatment
for infertility and was using gonadotropins. Ultrasound
images of the ovaries show grossly enlarged ovaries with
large cysts (measuring 2.6 to 3 cms.) in both ovaries.
These ultrasound findings are diagnostic of OHSS or
ovarian hyperstimulation syndrome.
Ovarian hyperstimulation syndrome (OHSS):
The ultrasound image again show hyperstimulated
ovaries. Both ovaries are grossly enlarged and cystic.
This young adult female patient showed multiple large
theca lutein cysts of both ovaries, arranged in spoke-
wheel pattern (ultrasound images above) which were the
result of use of gonadotropins in the management of
infertility. The cysts vary in size from 2 to 4 cms. with the
ovaries massively enlarged (each ovary measures up to 7
cms. in size). This can be classified as grade-2
hyperstimulation of the ovaries (ovarian diameter from 5
to 10 cms.). There is not evidence of ascites. The color
Doppler image of the ovaries shows vessels passing along
the margins of the cysts. One of the complications of such
enlarged ovaries in OHSS is torsion and in certain cases rupture of the ovaries, both of
which are medical emergencies. Ovarian hyperstimulation syndrome is known to occur
more frequently in patients of pre-existing Polycystic ovaries (PCO).
6
PERSISTENT ANOVULATORY FOLLICLE
Failure of ovulation and development of “cystic” follicle. The
follicle typically grows larger than the mean preovulatory
follicle diameter of 23 mm, thin atretic follicle walls are
observed and small flecks of particulate matter are
frequently seen in the lumen or aggregated at the side of the
structure.
BENIGN OVARIAN NEOPLASIA
Images of a small intraovarian dermoid cyst (A, B). The cyst is
completely embedded in the ovary and is surrounded by
focal areas of hyperechoicity. Small follicles are observed in
the surrounding stroma. Folliculogenesis and ovulation were
impaired in this ovary. The contralateral ovary demonstrated
compensatory hypertrophy.
Premature ovarian failure.
Image from a woman in premature ovarian failure. Only the
stroma of the ovary is identified. A very few follicles of less
than 1 mm diameter can be observed on the inferior aspect
of the ovary.
POLYCYSTIC OVARY SYNDROME
Images from women with differing expressions of the four
major subtypes of the metabolic syndrome associated with
polycystic ovary syndrome (A–D). The images exhibit quite
differing ultrasonographic appearances in the size and
distribution of follicles within PCOS ovaries. A recent corpus
luteum is clearly visible in the ovary in panel (D).
7
The Oviduct (Fallopian Tube)
Normal Oviduct
An image of an oviduct visualized from the uterine cornu to the
fimbria. The ampulla, infundibulum and very fine interfaces
representing the fimbria may be appreciated on the superior
aspects of the ovaries.
The fimbria of the oviduct are clearly visualized in free fluid
surrounding the ovary following ovulation or
hysterosalpinography.
Hydrosalpinx
Hydrosalpinx is usually easily diagnosed as well-constrained
fluid accumulation in the adnexae. In some cases, adhesions
between the oviduct and ovary may be visualized.
Uterus
Reconstructed coronal view of the uterus demonstrating
cornuas (arrow) and cervix, with a normal uterine contour
Normal Uterus
Planar views of normal uterus using volume contast imaging
8
Uterine Pathology
Fibroids (leiomyomata)
Intramural leiomyomata are frequently visualized. Examples
of fibroids which compromise the contours of the
endometrial cavity are shown (A–D). Refraction artifacts
resulting from tissue density interfaces and the texture of the
fibroids often aid in their identification.
Congenital anomalies of uterus
—
Unicornuate uterus
—
Bicornuate Bicollis Uterus
—
Didelphic uterus with Left sided hematometra
—
Subseptate Uterus
9
—
Complete Septate
—
Arcuate uterus
Endometrium
Post menstruation
Trilaminar appearance during proliferation
11
Secretory phase
Premenopausal Endometrium
Sagittal US image of the uterus obtained during the
secretory phase of the menstrual cycle shows a
thickened, echogenic endometrium (cursors).
Pathology of Endometrium
Endometritis. US image demonstrates multiple
echogenic foci within the endometrium (arrow)
representing gas.
Endomaterial polyp
Submucosal fibroid. (a) Transvaginal US image reveals a
uterine mass (arrows) with posterior acoustic
shadowing.
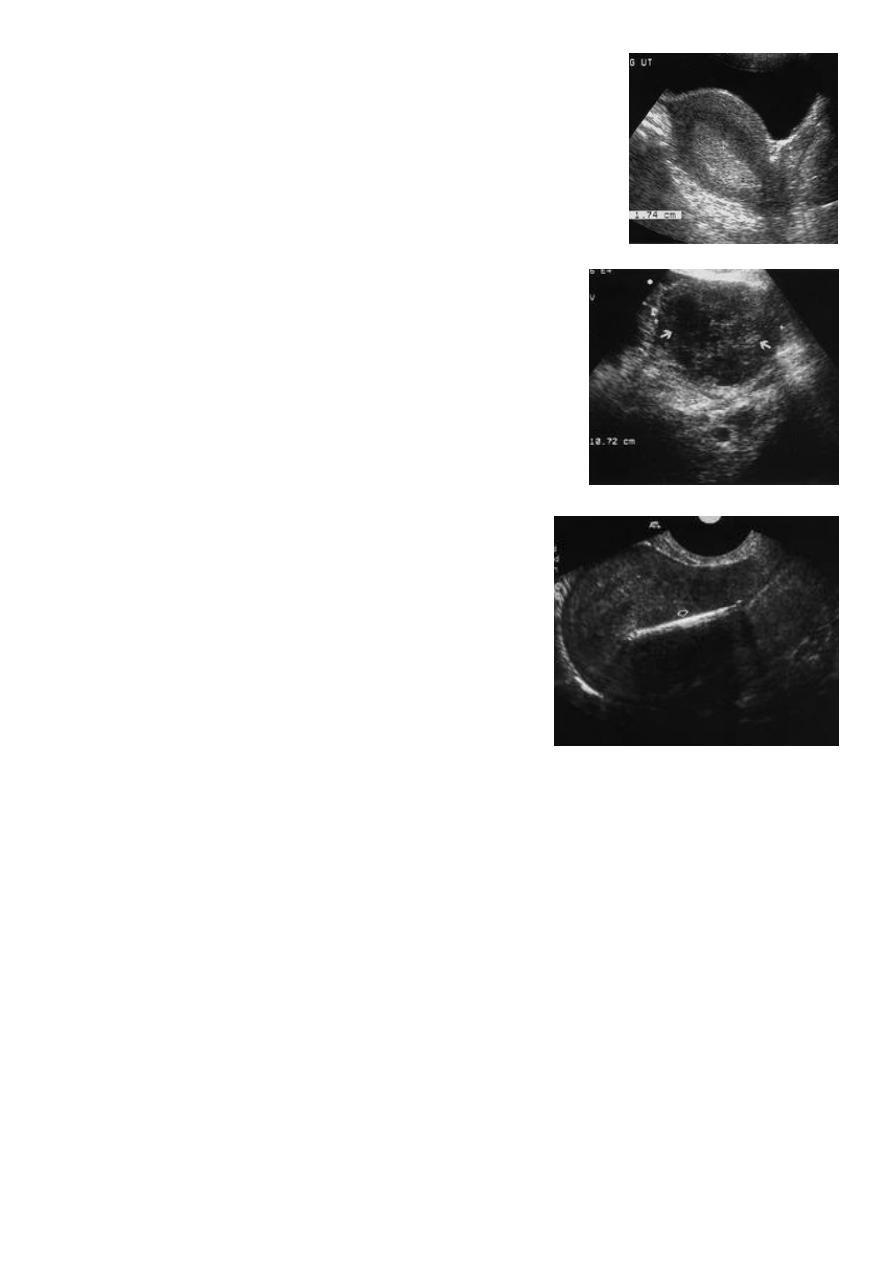
11
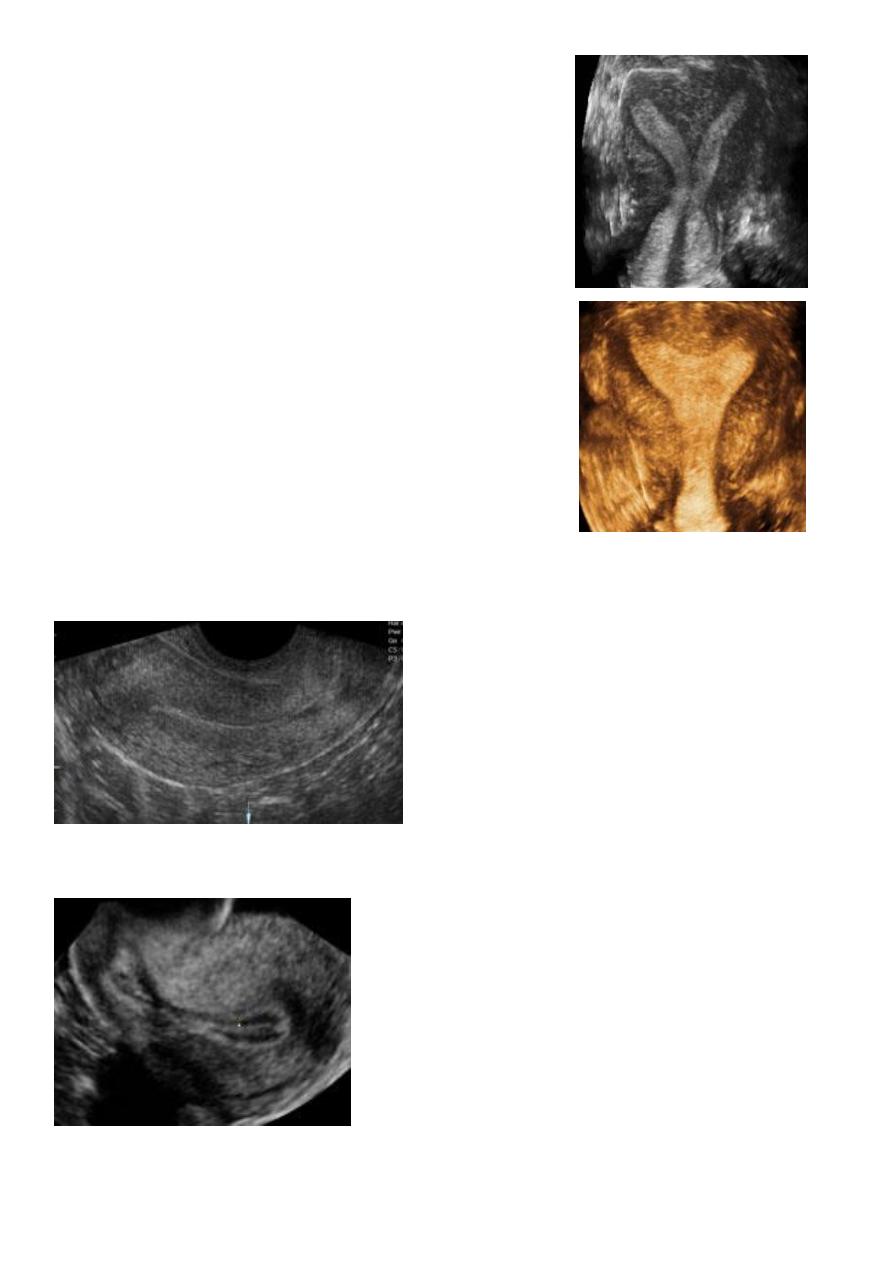
Endometrial hyperplasia. US image shows an endometrium with
diffuse thickening (maximum thickness, 1.74 cm) due to
hyperplasia (cursors). This finding was confirmed at biopsy.
Endometrial adenocarcinoma.
(a) US image reveals a heterogeneous endometrial mass
(arrows) that is difficult to distinguish from the myometrium.
Cursors indicate the entire transverse width of the uterus.
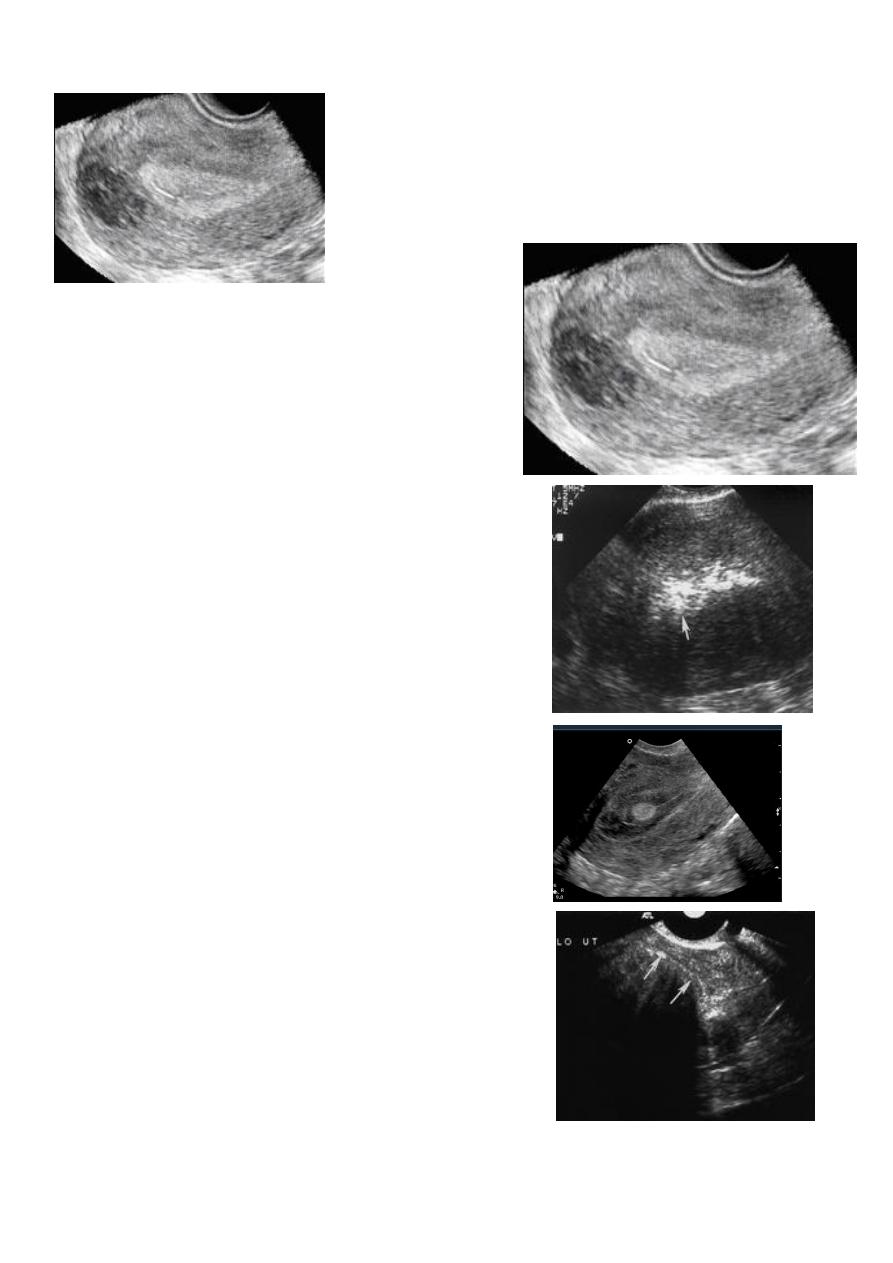
IUD. US image shows a hyperechoic linear structure
within the endometrial canal (arrow) representing an
IUD.