
1
Gynecology
د.احمد جاسم
Lec-7
FERTILITY CONTROL
Men and women have used contraception, in one form or another, for thousands of years.
There is no one method that will suit everyone, and individuals will use different types of
contraception at different stages in their lives
The characteristics of the ideal contraceptive method are:
• highly effective
• no side effects
• cheap
• rapidly reversible
• widespread availability
• acceptable to all cultures and religions
• easily distributed
• can be administrated by non- health care personnel
Virtually all methods of contraception occasionally fail and some are much more effective
than others.
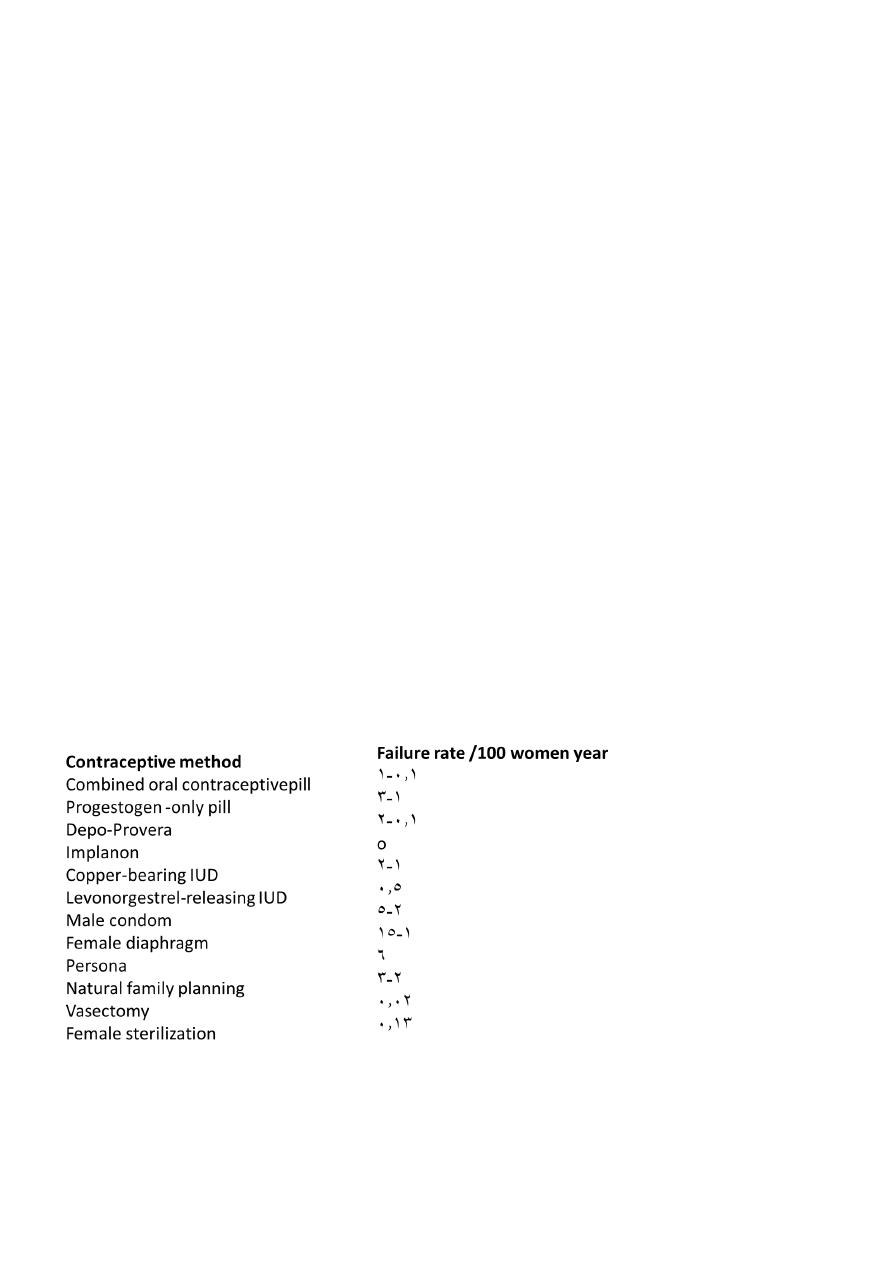
Failure rates are traditionally expressed as the number of failures per 100 woman-years
(HwY ), i.e. the number of pregnancies if 100 women were to use the method for 1 year.
Failure rates for some methods vary considerably, largely because of the potential for
failure caused by imperfect use (user failure) rather than an intrinsic
Classification
Methods not requiring medical cosultation:
1-coitus interruptus
2-safe period[Natural family planning]
3-vaginal spermicides
4-barrier methods include :
• Male condom
• Female barriers
2
Methods requring medical supervision
1-Hormonal contraception:
• Combined oral contraceptive methods
• Progesterone-only preparations :include
A-progesterone only pills
B-injectables
C-Subdermal implants
D-Hormone-releasing intauterine system
2-Intauterine device
3-Post-coital emergency contraception
4-occlusive diaphragms&caps
Perminant methods[sterilization]
• Female tubal occlusion
• Male vasectomy
Failre rate for contraception

3
Hormonal contraception
Combined oral contraceptive pills
Combined oral contraception (COC) - 'the pill' – was first licensed in the UK in 1961. It
contains a combination of two hormones: a synthetic oestrogen and a progestogen (a
synthetic derivative of progesterone).
Since COC was first introduced, the doses of both oestrogen and progestogen have been
reduced dramatically, which has considerably improved its safety profile..
Combined oral contraception is easy to use and offers a very high degree of protection
against pregnancy, with many other beneficial effects. It is mainly used by young, healthy
women.
Formulations
Combined oral contraceptive pills contains both:
1-Synthetic Estrogen (Ethinyl estradiol mostly):
The dose of oestrogen varies from 50 to 15 μg (microgram).
2-Synthetic progestogens
Either one of these :
*First generation(e.g. norethindrone).
*Second generation progestins (e.g. levonorgestrel) .
*Third generation series including gestodene, desogestrel and norgestimate.
Monophasic pills contain standard daily dosages of oestrogen and progestogen.
Biphasic or triphasic preparations have two or three incremental variations in hormone
dose.
Current thinking is that biphasic and triphasic preparations are more complicated for
women to use and have few real advantages.
Most brands contain 21 pills; one pill to be taken daily, followed by a 7-day pill-free interval.
There are also some every-day (ED) preparations that include seven placebo pills that are
taken instead of having a pill-free interval. For maximum effectiveness, COC should always
be taken regularly at roughly the same time each day.

4
preparation
1. low-dose pills containing 30μg of ethinyl estradiol
2.high-dose pills contain contain 50 μg estrogen. Higher dosages of oestrogen are strongly
linked to increased risks ofboth arterial and venous thrombosis
3.Yasmin contains ethinyl estradiol and drospirenone.
Drospirenone has antimineralocorticoid activity. It can help prevent bloating, weight gain,
and hypertension, but it can increase serum potassium.
Yasmin is contraindicated in patients at risk for hyperkalemia and should not be combined
with other drugs that can increase potassium
Mode of action
Combined oral contraception acts both centrally and peri pherally .
•centrally Inhibition of ovulation is by far the most important effect. Both oestrogen and
progestogen suppress the release of pituitary follicle stimulating hormone (FSH) and
luteinizing hormone (LH), which prevents follicular development within the ovary and
therefore ovulation .
• Peripheral effects include
- making the endom trium atrophic and hostile to an implanting embryo
- altering cervical mucus to prevent sperm ascending into the uterine cavity.
Contraindications
Absolute contra indications
• Circulatory diseases:
- iscihaemic heart disease- cerebrovascular accident
- significant hypertension
- arterial or venous thrombosis
- any acquired or inherited pro-thrombotic tendency
- any Significant risk factors for cardiovascularpisease
• Acute or severe liver disease
• Oestrogen-dependent neoplasms, particularly breast cancer
• -Breastfeeding <6 weeks post-partum

5
• -Smoking ≥15 cigarettes/day and age ≥35
• Focal migraine
Relative contra indications
• Generalized migraine
• Long-term immobilization
• Irregular vagli.nal bleedillg (until a diagnosis has been made)
• Less severe risk factors for cardiovascular disease, e.g. obesity, heavy smoking, diabetes
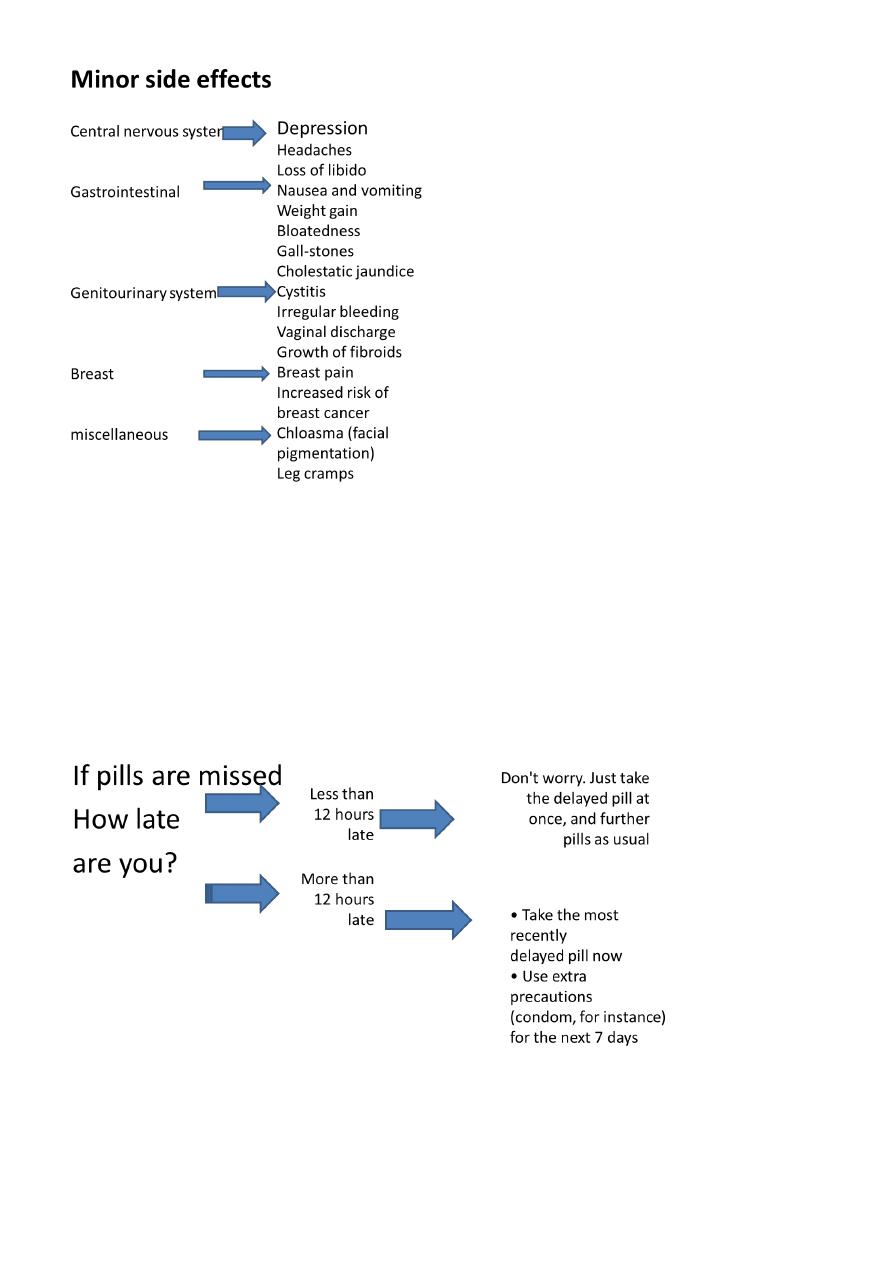
Side effects
major side effects
1-Venous thromboembolism
Oestrogens alter blood clotting and coagulation in a way that induces a pro-thrombotic
tendency, although the exact mechanism of this is poorly understood.
The higher the dose of oestrogen within COc, the greater the risk of venous
thromboembolism (VTE).
Type of progestogen also affects the risk of VTE, with users of COC containing third-
generation progestogens being twice as likely to sustain a VTE.
The risks ofVTE are:
• 5 per 100 000 for normal population,
• 15 per 100 000 for users of second-generation COC,
• 30 per 100 000 for users of third-generation COC,
• 60 per 100 000 for pregnant women
2-Arterial disease
*1 per cent of women taking coc will become significantly hypertensive and they should be
advised to stop taking COC
*The risk of myocardial infarction and thrombotic stroke in young, healthy women using
low-dose cac is extremely small.

6
*Cigarette smoking will, however, increase the risk, and any woman who smokes must be
advised to stop COC at the age of 35 years. Around
3-Mortality
There is increased mortality in women using the pills over women not using it.this is related
to age&smoking habits.Death is most often the result of pulmonary embolism,cerebral or
coronary thrombosis.
Women who are under 35 years,do not smoke or have hypertention or diabetes have no
exess mortality
In women over 35 years who are on pill the exess mortality rises&rises more in women who
smoke or have hypertention
4-Carcinogenic effect
• Breast cancer
Advising women about the association between breast cancer and COC is very difficult.
Most data do show a slight increase in the risk of developing breast cancer among current
COC users (relative risk around l. 24). This is not of great significance to young women, as
the background rate of breast cancer is very low at their age. However, for a woman in her
forties, these are more relevant data, as the background rate of breast cancer is higher. The
same data also showed that beyond 10 years after stopping coc there was no increase in
breast cancer risk for former coc users
• Cervical cancer
More than five years of pill use may be associated with small increase risk of cervical
carcinoma.
• Liver cancer
Benign hepatic adenoma is a rare consequence of COC use.
7
How to use pills
The patient begins taking the pills on the first day of menstrual cycle then in the next cycles
they are administered in fifth day of the cycle and continue for 21 days, each day at the
same time, then discontinued for 7 days to allow for withdrawal bleeding that mimics the
normal menstrual cycle which occur after 3-5 days from stopping pills

8
Drug interaction
*This can occur with enzyme-inducing agents such as some anti-epileptic drugs increase
activity of hepatic enzyme so reduce efficacy of COC . Higher dose oestrogen coc containing
50 Mg ethinyl oestradiol may need to be prescribed
*Some broad-spectrum antibiotics Ampicillin, Amoxicillin, Tetracycline , Neomycin can alter
intestinal absorption of COC and reduce its efficacy. Additional contraceptive measures
should therefore be recommended during antibiotic therapy and for 1 week thereafter
*Steroids ,Ascorbic acid (Vitamin C) and acetaminophen may elevate plasma ethinyl
estradiol so increse its efficacy
Positive health benefits
*COC users generally have light, pain -free, regular bleed and therefore COC can be used to
treat heavy or painful periods i .e menorrhagia & dysmenorrhea
*It will also improve premenstrual syndrome (PMS)
*reduce the risk of pelvic inflammatory disease (PID).
*decreased incidence of benign breast lump
*decrease number of functional ovarian cyst
*less endometriosis
*COC offers long-term protection against both ovarian and endometrial cancers.
*It can also be used as a treatment for acne.
Combined oestrogen and progesterone vaginal ring
It is soft ring that a woman can insert into vagina; and the Women who use Ring leave the
ring in place for 3 weeks during a month. During the 4th week, the ring is removed for 7
days. A new ring is used for each cycle.
Combined hormonal patches
A contracept ive t ransdermal patch containing oestrogen and progestogen has been
developed and releases norelgestromin 150 Mg and ethinylestradiol 20 Mg per 24 hours.
Patches are applied weekly for 3 weeks, after which there is a patch-free week.
Cont raceptive patches have the same risks and benefits as COC and, alt hough they are
relatively more expensive, may have better compliance.