
1
Fifth stage
Surgery
Lec-2
د.بسام
8/11/2015
Anorectal malformations
Introduction:
-Assurbanipal library: (when a woman bears a child whose anus is closed then the whole
land will suffer the want of food).
- becoming less common.
-imperforate anus wrong name ? Most have fistulous connection.
- Correction is difficult :-
1- loss of relation to sphincter.
2- abnormal muscle development.
3- abnormal nerve supply.
Incidence :
- About 1-3000 to 1-5000 live birth.
- Males affected slightly more than female.
- high lesion =male/low lesion =female
- Most cases sporadically.
- Risk of inheritance only 1%.
Classification :
Different sub type classified according to:-
1-relation of terminal bowel to pelvic floor of (levator ani muscle ).
2- presence or absence of fistula(skin or uro genital).
3- conditions needs colostomy , others not need.
1- High type : blind end rectum above levator ani muscle
a-with fistula to
-bladder or urethra in male
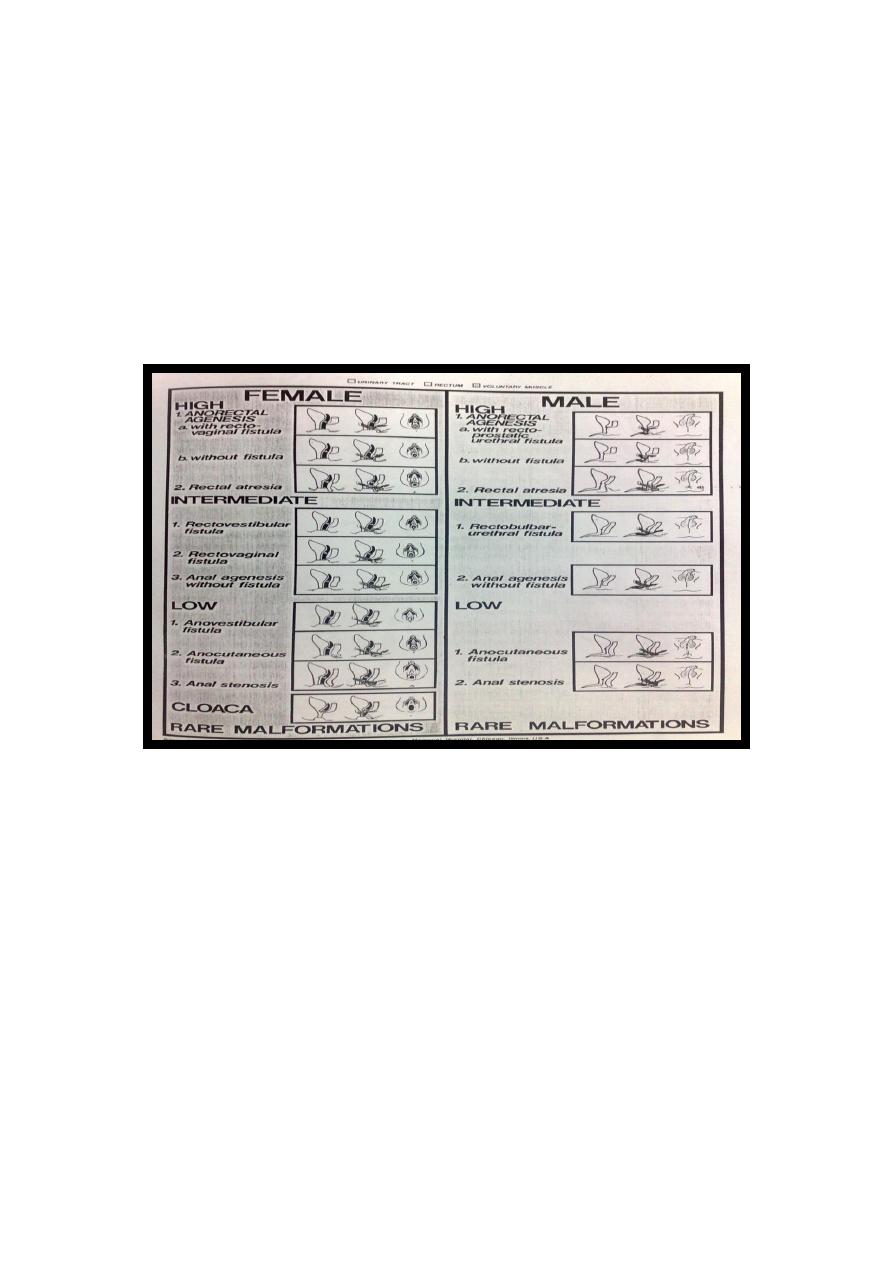
2
-vagina in female.
b-without fistula (anorectal agenesis or atresia )
2-low type: blind end rectum below levator ani muscle.
a-with fistula to- skin (cutaneous fistula) - vestibule
b-without fistula (anal agenesis)
3- cloaca in female (rectum ,urethra and vagina in one opening or channal called (
urogenital sinus)
International classification :
Associated anomalies:-
Genito urinary anomalies
-50% of cases and its include:-
1-neuropathic bladder.
2-vesicoureteral reflux.
3-ureterocel.
4-ureteric duplication.
5-renal agenesis.
6-bladder or cloacal exstophy.
7-miscelaneous.

3
Skeletal anomalies:-
-20% of cases:-
1- vertebral.
2-spinal dysraphism.
3-sacral anomalies.
4-spinal cord and pelvic nerve dysfunction.
5- pelvic floor dusfunction.
Cardiovascular anomalies:
-
-12% of cases and it may be life threatening:-
1- V.S.D.
2-A.S.D.
3-A-V Canal.
4-Right aortic arch.
Gastro intestinal anomalies:-
- 10% of cases:-
1-Congenital cystic colon(C.C.C.).
2-Dudenal Artesia.
3-esophageal Artesia.
4-intestinal artesian.
Syndromes or associations:-
1- Down syndrome.
2- V.A.C.T.E.R.L. association.
3- Currarino triade.
Clinical presentations
{kind=link}
intestinal obstruction.
-simple inspection(diagnostic)/level(difficult).
- Condition of anal dimple(well formed=low/flat=high).

4
-voiding of meconium per urethra(in male) high type.
- sometime cutaneous fistula filled with meconium low type.
-in female carful genital examination essential (no.of opening).
3 opening: suggest vestibular fistula.
2 opening : suggest agenesis.
1 opening : diagnostic for cloacae with common channel(urogenital sinus).
Radiology
Determined:
1-relation of rectum to sphincter muscle.
2-associated anomalies.
1-x-ray of the spine and chest (sacral , VATER).
2-Lateral invertogram ( pubococcegeal line) 18-24hr.after birth.
-gas shadow above this line suggest high type.
- gas shadow below suggest low type.
3-lateral decubitus X-ray.
4-M.R.I.
5- ultrasound.
6-Echocardiography.
7- M.C.U.
Treatment and prognosis :
Satisfactory results=efficient continence.
general considerations:
1-perineal fistula=low lesion = good prognosis.
2-meconium in urine (in male) = high type = colostomy.
3-in female=search for fistula=mostly local surgery = good prognosis.
if no fistula = colostomy.
5
4-sacral anomalies + neurogenic bladder = poor sphincter action = poor prognosis
Surgical technique
Low lesion:
good long term outlook but tendency to constipation
- A perineal anoplasty =cutaneous fistula.
- anal stenosis &imperforate anal membrane=simple incision &dilatation.
-vestibular fistula =transpositioning anoplasty few monthes later.
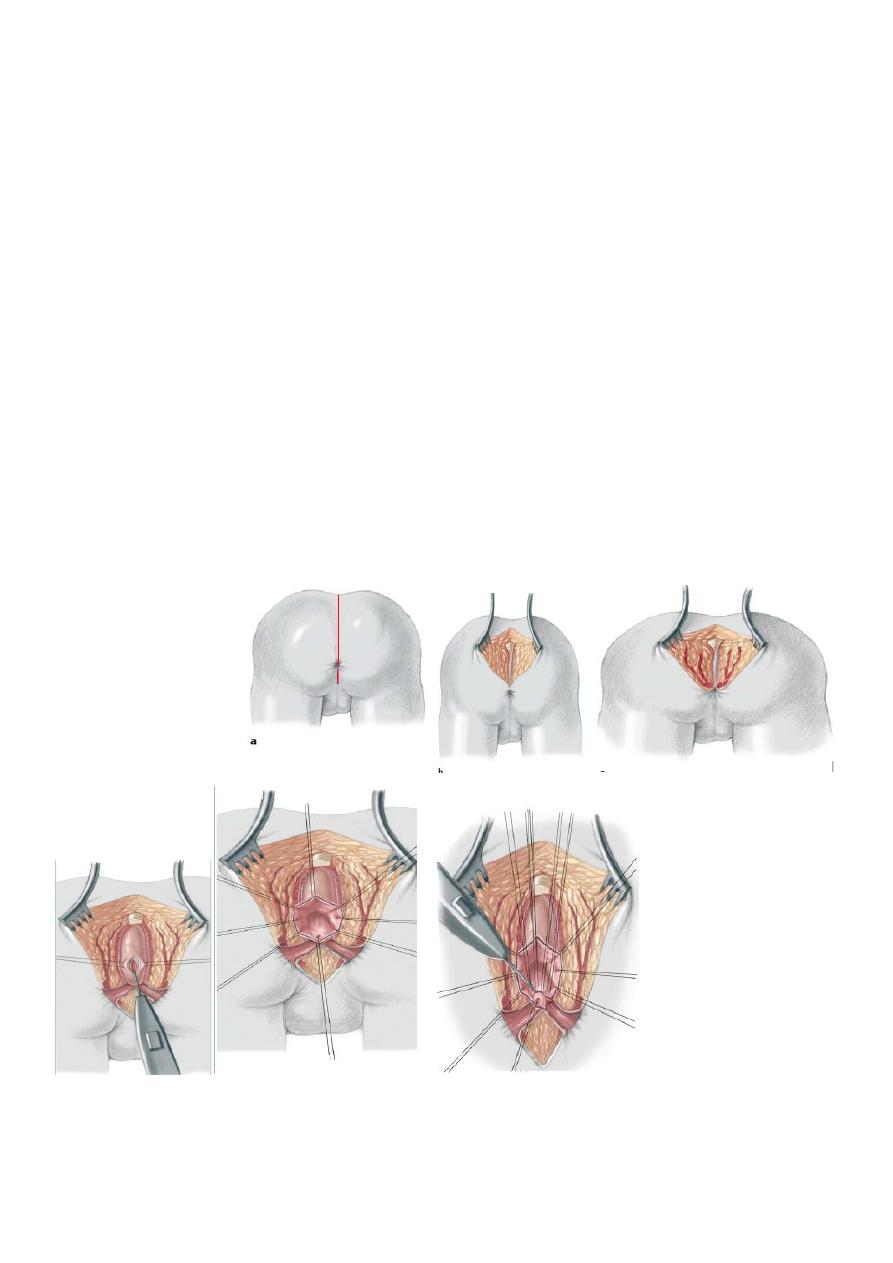
High lesion:
- Colostomy at birth.
-
3-4 month later definitive surgery using posterior sagital anorectoplasty(P.S.A.R.P.
pullthrogh) Or penna technique.
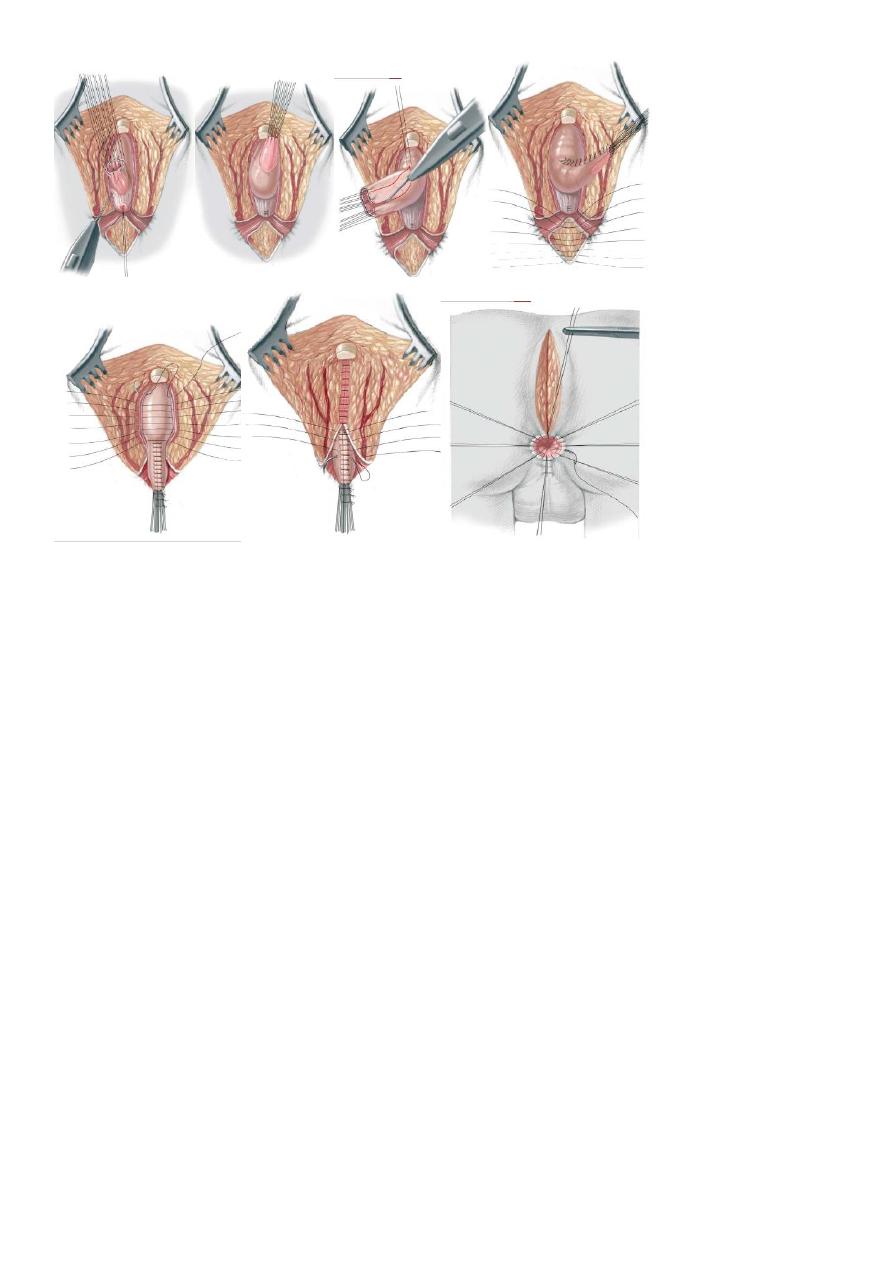
6
- Recently laparoscopic pull through using nerve stimulator to identify anal sphincter ,
-the sphincter is not well developed and nerve supply is deficient= continence not good.
- 2 months later colostomy closed.
- Regular anal dilatation.
Complications
Early:
1. wound infection.
2. colostomy complications.
3. recto urinary fistula .
4. neurogenic bladder.
5. anal stenosis.
6. rectal mucosal prolaps.
Late:
1. constipation.
2. megarectum.
3. soiling (incontinence)