Urology
عملي - كتابة الطلابanatomy :
the kidney extend from L1-L3
kidney and ureter is retroperitoneal
uretropelvic junction{UPJ} :between the ureter and the kidney [ if obstructed will cause UPJ obstruction and hydronephrosis]
uretrovasical junction : between the ureter and bladder{ if dilated will cause uretrovasical reflux}
the the urethra is 2 part :
posterior urethra : prostatic – membranous
anterior urethra : bulbar – penial
the epithelial lining the urinary system is transitional cell
the kidney is consist of cortex and medulla ( the thickness of cortex reflect the function …much thickness more function )
the pelvic and ureter and bladder is low pressure system to alow the urine to descent into the bladder .the urine is descent by gravity and peristalsis of the ureter( if the pressure increase inside the bladder or ureter this will prevent the urine from descend and cause hydronephrosis and gradually renal failure )
the capacity of the bladder is 350-500 ml
hydronephrosis
is aseptic dilatation of pelvicalecial system (no infection..no fever)
hydronephrosis will cause pressure on the cortex and cause gradual atrophy of the cortex and decrease in thr renal function (thining of the cortex ---less function )
in hydeonephrosis
increase pressure will decrease the urine entering the bladder so develop renal failure
decrease cortical thickening by the pressure lead to renal failure
if the cause is from the ureter –unilateral hydronephrosis
if the cause in the bladder –bilateral hydronephrosis
most common cause of hydreonephrosis is obstruction by calculi (stone)
investigation in urology
general urine examination
we see :the color -pus cell - cast - RBC
the food and drug (rifampicin-flagel ) may change the color of the urine
us :advanteges : a. simple b.not coasty
disadvanteges : cant see the function of the kidney .cant see the most of the ureter …
KUB : { kidney. Ureter. Bladder}
It is a plane X-ray taken from the level of L1 to bladder
In the KUB we can see :
bone
Soft tissue shadow like …. liver. Kidney.psoas muscle
Radio opaque shadow …..stone ( normal KUB doesn't mean absent of stone . it may be radiolucent)
Gas appear as a black
IVU: is to confirm the diagnosis
IVU is for functional and anatomical
We must do an KUB before the IVU
Contraindication is sensitivity and RF
If we want to exam the renal function we must do urea and createnin .but if we want to exan a single kidney we must do a IVU and renal isotop scan
CT scan : it will show anatomy .it is the definitive diagnosis .but have a high radiation
Redionucli study : for te function of the kidney
MRI : give anatomy and pic .no radiation
MRU: for patient with sensitivity to IVU
MCUJ :( macturating cystourethrogram ) for diagnosis of uretro vesical reflux
RETROGRADE urethrograph : for the diagnosis of urethral problem
Stone
Type of stone :
Ca oxalate is the commonest
Ammonium magnesium & phosphate (staghorn stone)
Uric acid stone
Cestein stone
AMP stone تتجمع في الوسط القاعدي
Uric acid stone تتجمع في الوسط الحامضي
Anuria :{ abscent of urine } is is emergency usually with single kidney or bilateral obstruction .we should put an nephrostomy( urinary divertion) and check the renal function test to know the severity of the case
Acute retention of urine : no urine with full bladder usually due to obstruction in the bladder or urethra .it is diagnosed clinicaly . and it resolved by butting a folly catheter
Acute retention of urin ---- folly catheter
Anuria ---- nephrostomy
Treatment of stone : depent on the size and type of stone
Renal stone :
1.from 4-5 mm do conservarive and follow up
Antibiotic – analgesic – water and fluid – movement
2.flexible uretroscope with laser ( if the conservative treatment fail and if the stone is large
3.large stone 0.7 – 1 cm we do ESWL (extracorporeal shock wave lithotripsy )
Contraindication :
It need multiple sation
It cause bleeding so it contraindicated in patient with bleeding tendency
If we have lower obstruction
Stone larger than 2 cm
4.PCNL (percutaneous nephrolithotomy )
5. surgery : if all above failed
6.nephrectomy : staghorn stone with nonfunctioning kidney
And treatment can be combination between these option
Uretric stone
Very painful and colicy unlike renal pain is dull ache
1.conservative treatment : for 4-5 mm stone
Analgesia –antibiotic – water drink – movement –follow up2. Surgery : indication
Single kidney
Fail of medical treatment
Hydronephrosis
Options :
Flexible uretroscope with lazer is better for lower uritric stone
ESWL is better for upper uretric stone
Uretrolithotomy
Nephrectomy
Pyelonephritis :
1 .pain 2. Fever 3. Rigor 4. Tenderness 5.pyuria 6.may associated with vomiting
It is usually occur unilateral and with D.M
If the U.S is normal – use simple antibiotic
If U.S show complication ( stone . hydronephrosis ):
1.hospital addmition .parentral antibiotic until fever is gone we change to oral antibiotic
2.I.V fluid for 10-14 day
Cystitis
Frequency
Dysuria
Nocturia
Urgency
Pus +RBCs in urine
Low grade fever
Suprapubic pain or discomfort
Vesicoureteral reflux
It could be primary due to abnormal entrance of the ureter in the bladder or due to othe cause
It present as child with repeated UTI
Could be uni or bilateral
The urin will continuous to retrograde to the kidney and cause renal failure
Any child with recurrent UTI ..we should exclude reflux
Diagnosis:
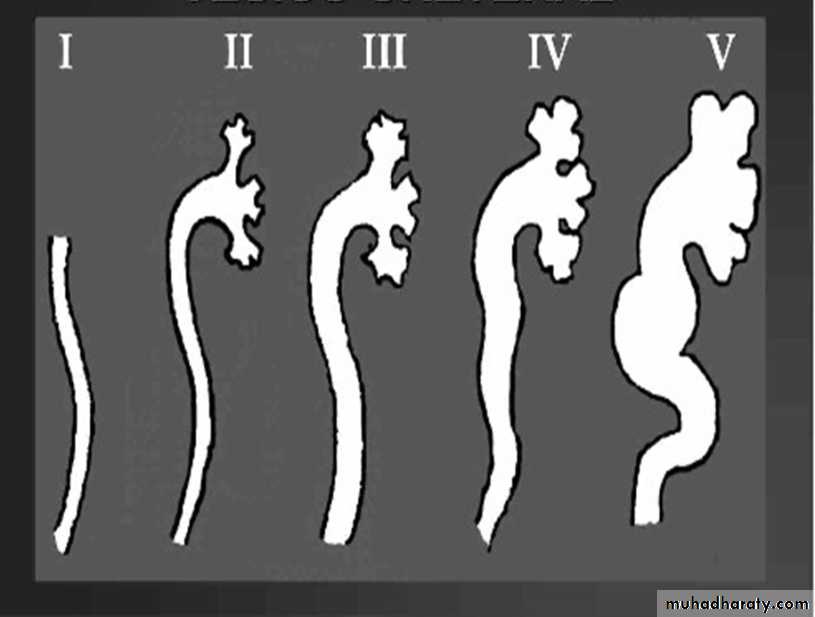
. MCUJ ( mucturating cystourethrogram )Grading
Grade 1 …. Urine reach the ureterGrade 2 ….. urine reach the kidney but no dilatation
Grade 3 ….. urine reach the kidney with mild dilatation
Grade 4….. urine reach the kidney with sever dilatation
Grade 5…. The urine reach the kidney with sever dilatation and tortuosity of the ureter
Treatment
If the case is mild we give prophylactic antibiotic( mithiprine) for lifelong and follow up and do MCUJ again .if not improve we change to surgerySurgery : cut from site of attachment then reimplantation
Sub trigonal injection of tiphlon or other substance
Grade 3.4.5 do directly to the surgery .
مع الشكر الجزيل ل
وسن نزار قبع و زينه محمد ادريس