
1
Fifth stage
Medicine
Lec-4
.د
فاخر
24/11/2015
RHEUMATOID ARTHRITIS
Treatment
Goal of treatment
reduce inflammation and pain,
preservation of function,
prevention of deformity.
Nonpharmacological therapy
Education
Exercise
Aerobic conditioning
Strengthening
Reduction of adverse mechanical factors
Pacing of activities
Weight reduction if obese
Pharmacological therapy
*simple analgesic drugs
*NSAIDs
*Topical creams
*Opioid analgesics
*Amitriptylin:
'disease-modifying antirheumatic drug' ((DMARD
*Corticosteroids
Local injections
Surgery
2
General Principles
Undelayed use of DMARDs
The major goal is full remission
Remission is infrequent with a single DMARD
DMARDs combinations can add benefits with little or no increase in adverse effects
SIMPLE ANALGESIA
Paracetamol (1 g 6-8-hourly) is the oral analgesic of choice because of its efficacy, lack of
contraindications or drug interactions, long-term safety, low cost and availability.
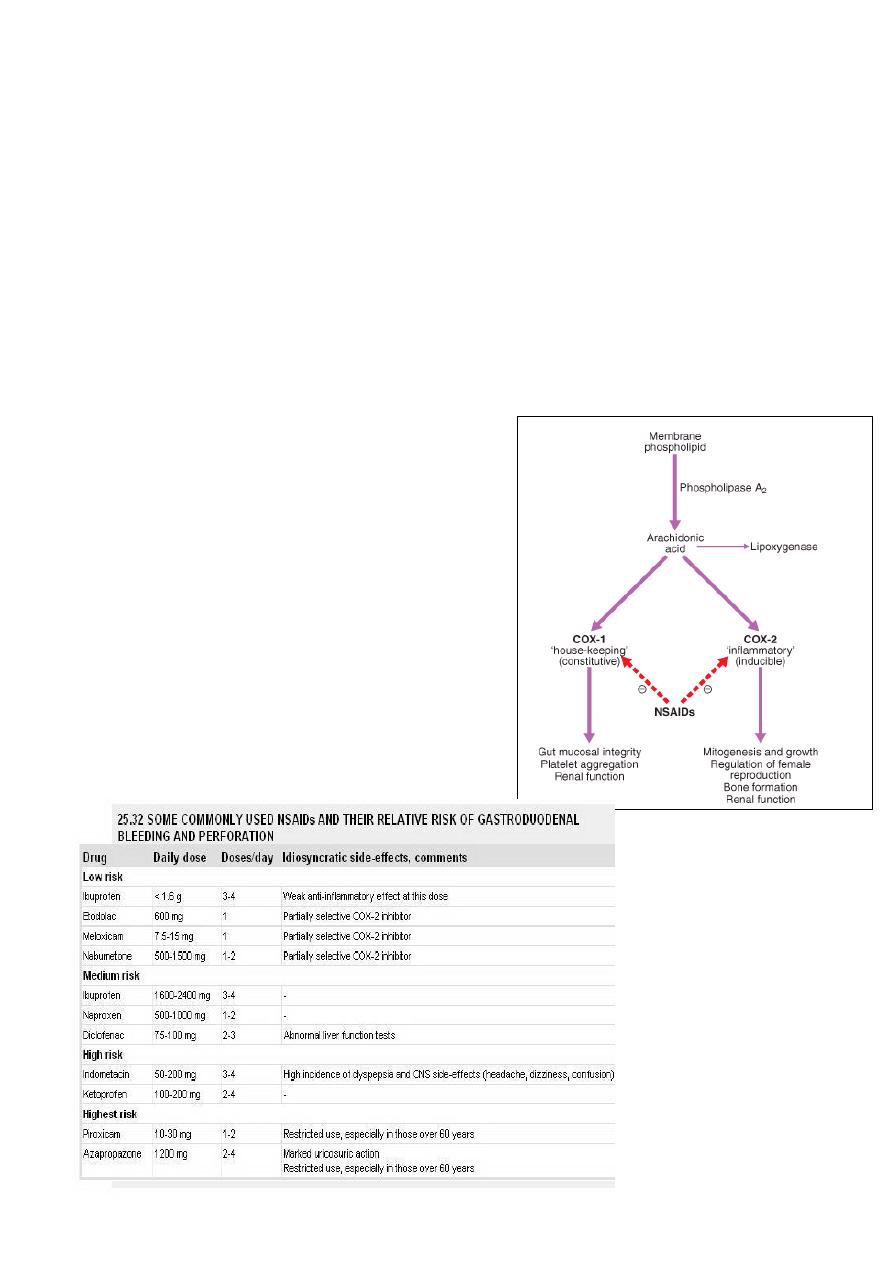
Paracetamol inhibits prostaglandin synthesis
centrally in the brain but has little effect on
peripheral production of prostaglandins
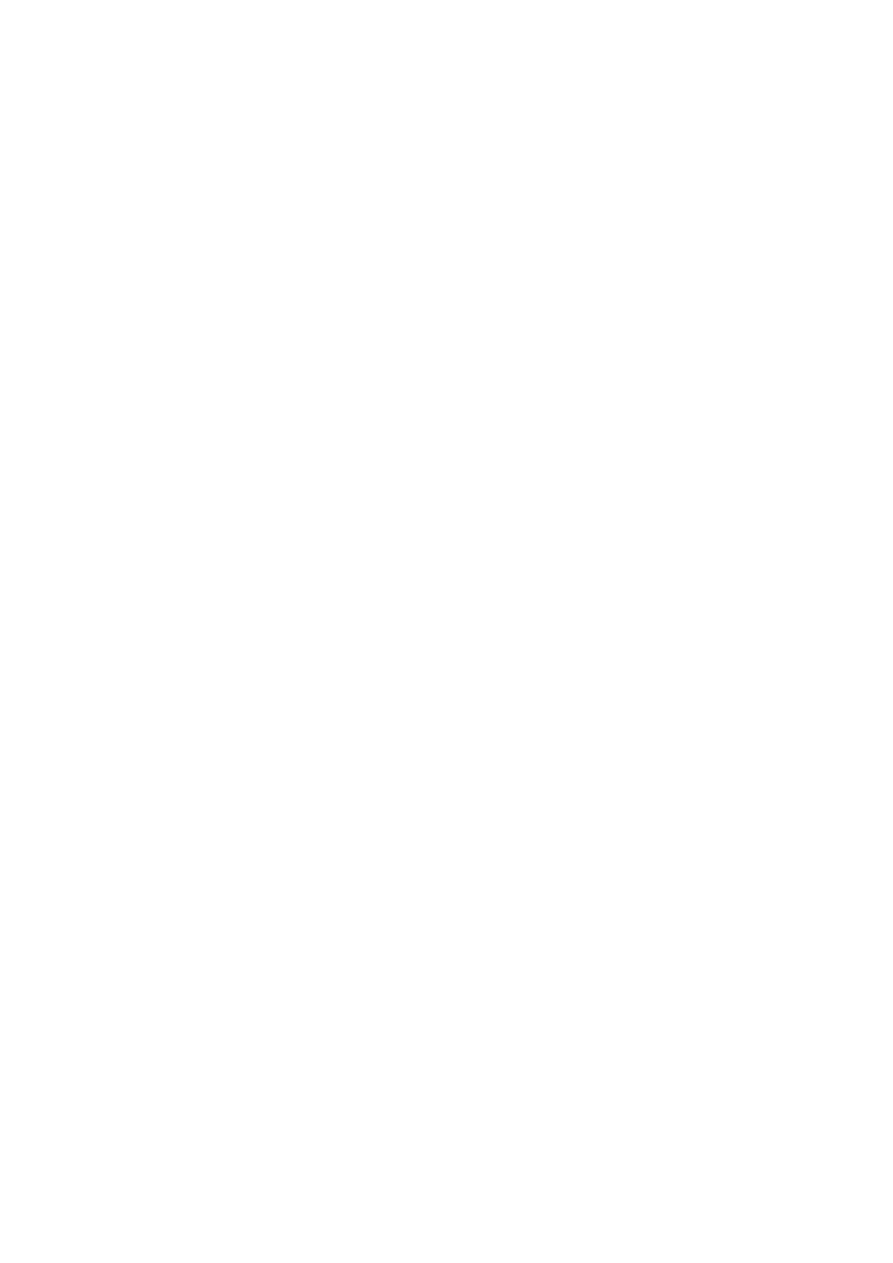
NON-STEROIDAL ANTI-INFLAMMATORY
DRUGS (NSAIDS)
These are among the top five most prescribed drugs
in many countries. Oral NSAIDs are often effective
for the pain and stiffness of inflammatory disease.
Long-acting NSAIDs given at night are particularly
helpful for marked inflammatory early morning
stiffness. NSAIDs may also reduce bone pain due to
secondary malignant lesions.
3
The major drawback of NSAIDs is gastrointestinal toxicity. Prostaglandins of the E series
play a major role in gastroduodenal defence mechanisms. By depleting mucosal
prostaglandin levels, aspirin and NSAIDs impair this 'cytoprotection', resulting in mucosal
injury, erosions and ulceration. NSAIDs are an important aetiological factor in up to 30% of
gastric ulcers.
IMPACT OF NSAID-INDUCED GASTRIC BLEEDING
Endoscopic evidence of peptic ulceration is found in 20% of NSAID users even in the
absence of symptoms
1% of patients with RA or OA are hospitalised each year with gastrointestinal bleeding
Annual mortality in people in the US and in the UK higher than deaths from diseases such as
myeloma, asthma, cervical cancer or Hodgkin lymphoma )
RISK FACTORS FOR NSAID-INDUCED ULCERS
*Age > 60 years
*Past history of peptic ulcer
*Past history of adverse event with NSAIDs
*Concomitant corticosteroid use
*High-dose or multiple NSAIDs
*Individual NSAID-highest with piroxicam, ketoprofen; lower with ibuprofen
PRINCIPAL INDICATIONS FOR ORAL OR PARENTERAL CORTICOSTEROID
1-For rapid, short-term (1-3 months) control of marked synovitis or systemic inflammation
while awaiting efficacy from slow-acting antirheumatic agent
2-For life-threatening (e.g. vasculitis) or organ-threatening (e.g. kidney, lung, eye)
inflammatory multisystem disease
3-For primary treatment of polymyalgia rheumatica
4-For control of inflammatory disease during pregnancy
LOCAL INJECTIONS
Intra-articular injections Injection of a long-acting corticosteroid may be useful adjunctive
therapy for short-term pain relief (OA, inflammatory arthritis) and for temporary control of
synovitis of just one or a few joints. The duration of benefit varies according to joint size

4
and the nature and severity of the arthritis, but is in the order of 2-8 weeks. Frequently
repeated injections may result in joint tissue atrophy and Cushing's syndrome .
Disease-modifying antirheumatic drug "DMARDs"
Slow-acting drugs are commonly indicated for rheumatoid arthritis, seronegative
spondarthritis, juvenile idiopathic arthritis and connective tissue diseases .The main
indications for use are:
persistent synovitis (> 6 weeks)
severe extra-articular disease (e.g. vasculitis, scleritis, renal involvement)
steroid-sparing effect (e.g. polymyalgia rheumatica resistant to low-dose corticosteroid)
inflammatory myositis.
Classification of DMARDs
1-Non-Immunosuppressive agents (“joint effective agents”)
2-immunosuppressive agents (“joint & systemic effective”)
3-Biological agents
1-Non-Immunosuppressive agents (“joint effective agents”)
Sulfasalazine
Hydroxychloroquine
Gold salts (e.g. sodium aurothiomalate)
D- penicillamine
2-immunosuppressive agents (“joint & systemic effective
Methotrexate
Azathioprine
Leflunomide
Ciclosporine
Other cytotoxic drugs
Methotrexate inhibits dihydrofolate reductase, interfering with DNA synthesis and cell
division .It has high efficacy, relatively low toxicity,, among this group, most rapid onset of
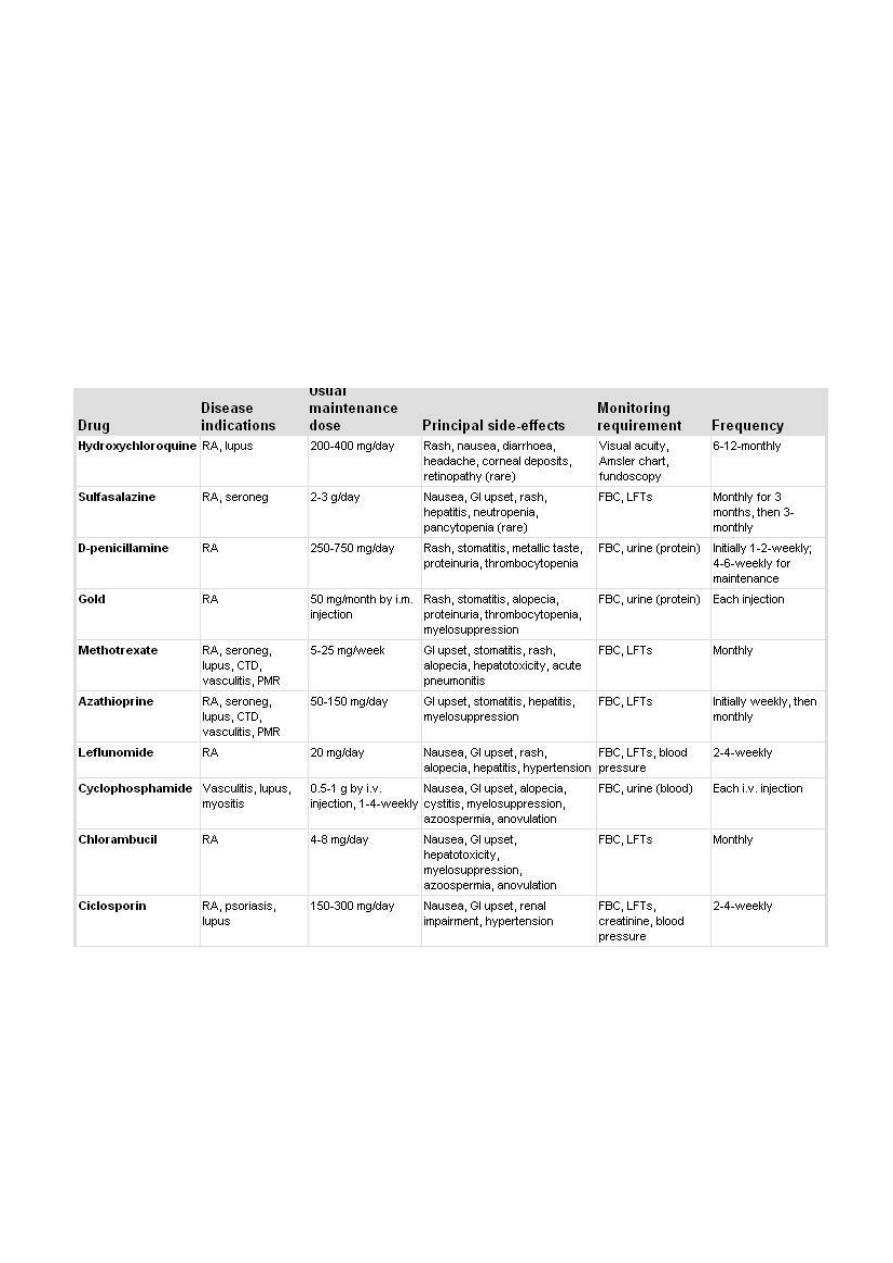
5
action (as early as 4 weeks). This drug has hematologic, pulmonary, and hepatic side
effects,. Folic acid (5 mg/day) reduces the incidence of adverse effects without reducing
efficacy.
Cyclophosphamide, azathioprine, and cyclosporine are immunosuppressive drugs that are
effective agents in treating RA. In addition to the risk of both common and unusual
infections, cyclophosphamide carries a risk of bladder and late lymphoid malignant disease;
the latter risk may also be present with azathioprine.
Among the oldest of are gold salts. Given as weekly injections, gold thiomalate or
thioglucose is effective in controlling disease in many patients; a few patients go into true
and complete remission. However, many patients experience side effects, including bone
marrow suppression, glomerulonephritis, and rash.
3- Biological Treatment (Anticytokines)
These drugs are more effective than standard DMARDs (with a faster onset of action,
greater clinical efficacy and sustained benefit) but because of their cost many countries
have set restrictive guidelines for their use. Current UK recommendations are that they
should be initiated only in active RA when an adequate trial of at least two other DMARDs
(including methotrexate) has failed.
6
• (TNF-α) and interleukin-1 (IL-1) play an important role in the pathogenesis of RA and
are therefore prime therapeutic targets
• Infliximab
• anti-TNF-α monoclonal antibody which is administered by intravenous infusion every
1-2 months..
Recombinant IL-1 receptor antagonist
Anakinra
Competitively blocks binding of IL-1 to its receptor
Monoclonal antibody that binds CD20 antigen on B-cells surface (Rituximab)
Each course of rituximab consisted of two courses of either 1,000 mg or 500 mg given iv
two weeks apart.
Prior to each rituximab infusion, all patients received methylprednisolone 100 mg iv; most
patients also received paracetamol and an antihistamine.
EXAMPLES OF COMMON USEFUL SURGICAL PROCEDURES FOR MSK DISORDERS
Soft tissue release decompression
Carpal tunnel(Median nerve) compression
• Synovectomy
• Joint replacement arthroplasty