بسم الله الرحمن الرحيم
Atopic Dermatitis
Erythematous , macule and plaques around the cheeks and peri-oral

Atopic Dermatitis
Erythematous , macules , vesicles and plaques around the cheeks and peri-oral, there is scaly layer
Atopic Dermatitis
Erythematous macules , patches and lichenfication( thickness of skin ) on the dorsum aspect of the hand

Atopic dermatitis

This disorder is a severely pruritic reaction in individuals with a personal or family history of allergic manifestations. It is characterized by flares
of congestion resulting in deep and superficial blisters, followed by peeling, scaling, and a dry, reddened surface. Flares generally result from contact with irritants, but stress is also a significant factor.
Atopic dermatitis
Erythematous patches around the popliteal fossa
Atopic dermatitis
Erythematous patches around the popliteal fossa
Acne
Macule , papules and pastule (pus + papule),hyperpigmented, and scar. If there is only comedom and white heads. It is considered mild degree of acne, drug induce keratiniaztine (isotrismne). The bacteria affect the face during acne colled (propino bacterium acne) can give the patient topical antibiotics like azithromycin, clindamycin.with white heads on the face

Acne
Macule , papule , pustules with white headAnd hyperpigmented area

Acne
Comedon ( primary lesion of acne “ black heads “ ) , pustules, papules
Acne
C losed comedon
Acne
Comedon
Bacterial infection
Leishmaniasis : Single or multiple Brown nodular lesion (indurated) with scale, crust and central erosion or ulceration. Not tender +/- satellite lesion, any site of sand fly bite. Rx (pentavalent antimonial compound (intralesional Na+ stibogluconate
Bacterial infection
Imptigo :Erythematous macules and pathes around the mouth Ddx imptigo staph infection Superficial honey-colored serous crusts are characteristic of this disorder. It is usually caused by a staphylococcus infection. Culture israrely reliable.

Bacterial infection
Erythematous patches on the right side of cheeks and around eye and onThe external surface of ear

Bacterial infection
Erythematous Macules and patches near metatarsal line oin the dorsum of the left foot

Bacterial infection
Erythematous , macules or patches and pustules
Fungal infection
Erythematous patches and plaques with active border around umbilicusAnd on the anterior surface of abdomen

Fungal Infection
Erythematous patches and plaques with active border around umbilicusAnd on the anterior surface of abdomen

Fungal infection
Scaly lesion on the both feet affect all the dorsal aspectDx : tinea pedis

Fungal infection
Fissured macerated skin on the plantar surface between 2nd and 3rd toes
Fungal infection
Tinea capitis Fungal infection in the head causing patchy hair loss. Well-demarcated erythematous plaque with thick scales and +ve pulling test (the hair is easily pulled) usually in older children or in adults. DDx alopecia areata Rx systemic antifungal (terbinafine).
Fungal infection
Tinea capitis Fungal infection in the head causing patchy hair loss. Well-demarcated erythematous plaque with thick scales and +ve pulling test (the hair is easily pulled) usually in older children or in adults. DDx alopecia areata Rx systemic antifungal (terbinafine).

Fungal infection
Yellowish discoloration of the dorsal surface and oncholysis
Fungal infection
Yellowish discoloration of distal subungal ascpect of nailDx: Tinea pedis

Fungal infection
Erythematous nail fold with scaly layer and distal subungul involvement
Fungal Infection
Nail atrophy with nail bed depression

Fungual infection
Pityriasis vercicolor (hypopigmented macuels or patches with scales that is more prominent upon stretching. Caused by Malassezia furfur (a normal fungus that inhabit the skin), after swimming. Occur in trunk, proximal extremity, in exposed and non-exposed areas (usually non-esposed). Increased in hot weather and after puberty. Treatment Topical antifungal (ketoconazole 2 week), selenium shampoo. may need systemic antifugal.
Fungal infection
Pityriasis vercicolor (hypopigmented macuels or patches with scales that is more prominent upon stretching. Caused by Malassezia furfur (a normal fungus that inhabit the skin), after swimming. Occur in trunk, proximal extremity, in exposed and non-exposed areas (usually non-esposed). Increased in hot weather and after puberty. Treatment Topical antifungal (ketoconazole 2 week), selenium shampoo. may need systemic antifugal.
Lichen planus
Confulent papular lesion under the breast and on the anterior surface ofAbdomen craeating a plaques of lichen planus with scaly

Lichen planus
Confluent plaques on the dorsum of hand erythematous
Lichen planus
Erythematous papules and macules scattered on the dorsal surfaceOf both feet

Lichen planus
Erythematous papules and plaques on the flexor surface of the wrist with palmar erosion
Lichen planus
Atrophied nails of the fingers
Lichen planus
Distal oncholysis and nail brittling , scaly layer of skin around the nail
Lichen planus
Erythematous mucus membrabe with whitish patches and ulceration
Lichen planus
Erythematous mucus membrabe with whitish blisters and erosions
Lichen planus
mucus membrane with whitish patches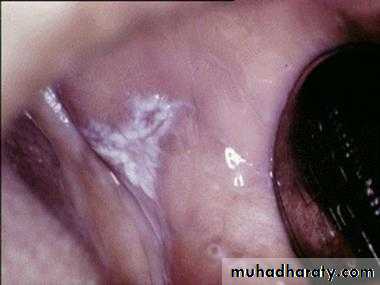
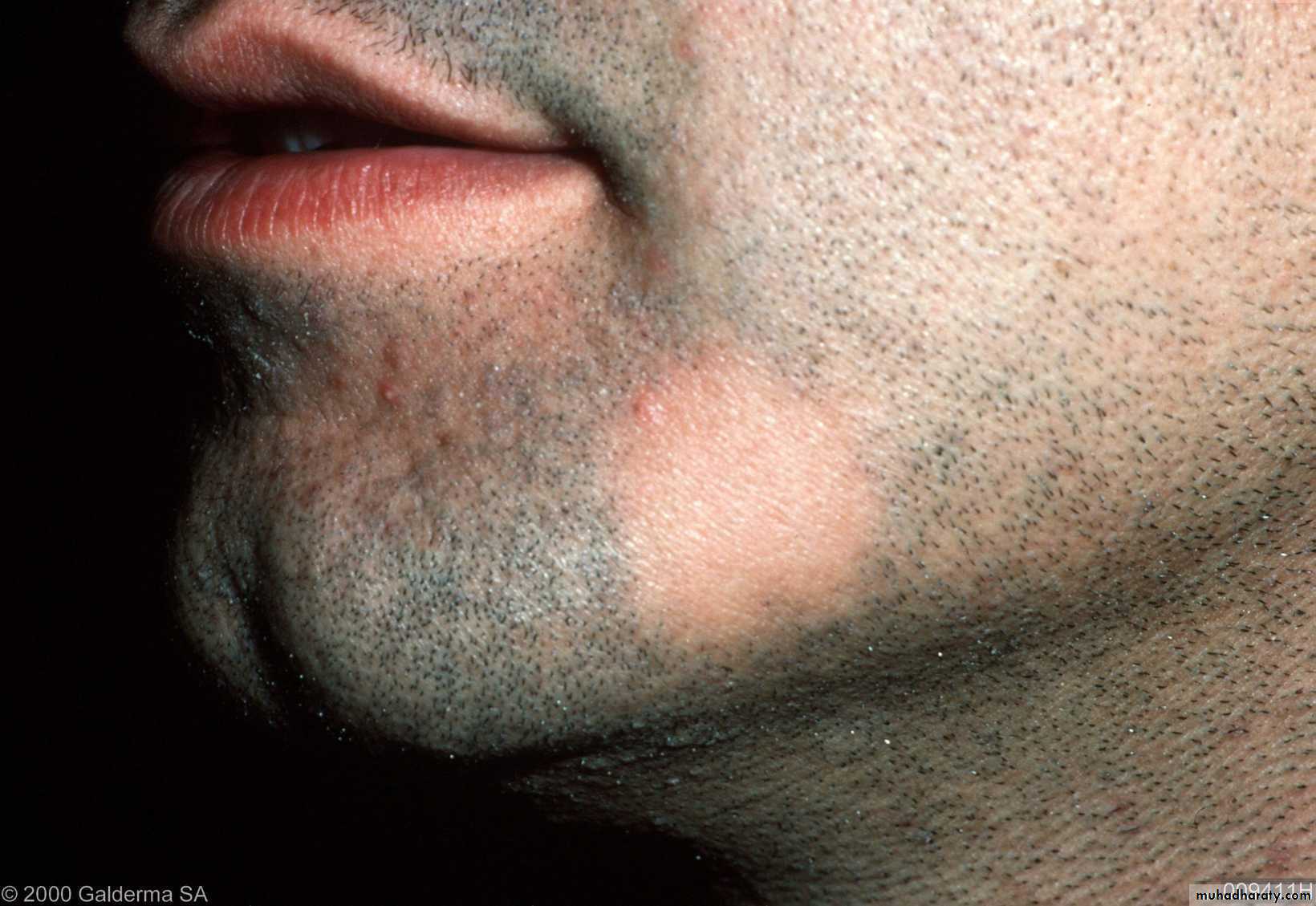
Alopecia areta
Patches of hair loss, normal skin, well demark affect the breadAutoimmune – anagen.
Treatment topical anthralin, topical or intral-lesional steroid, cyclosporin.
Alopecia areta
Patches of hair loss, normal skin, well demark affect the scalpAutoimmune – anagen.
Treatment topical anthralin, topical or intral-lesional steroid, cyclosporin.

Alopecia areta
Patches of hair loss, normal skin, well demark affect the scalpAutoimmune – anagen.
Treatment topical anthralin, topical or intral-lesional steroid, cyclosporin.

Alopecia areta
Patches of hair loss, normal skin, well demark affect the breadAutoimmune – anagen.
Treatment topical anthralin, topical or intral-lesional steroid, cyclosporin.

Acute lupus erythematous
Butter-fly rash erythematous affect the cheeks and nose and until reach the lips
Acute lupus erythematous
Butter-fly rash erythematous affect the cheeks and nose and until
Basal cell carcinoma
Basal Cell Carcinoma This lesion represents 90% of skin cancers. Basalcell carcinoma is the most common cancer. On the face, it usually starts as a reddened papule or nodule with a smooth surface and a translucent, pear
quality. Because of a poorly formed stroma, it is fragile and often bleeds. On the torso, the lesion hasan irregular surface, bright red color, sometimes scaly, with a distinct edge. Histologic examination is required

Basal cell carcinoma
Basal Cell Carcinoma This lesion represents 90% of skin cancers. Basalcell carcinoma is the most common cancer. On the face, it usually starts as a reddened papule or nodule with a smooth surface and a translucent, pear
quality. Because of a poorly formed stroma, it is fragile and often bleeds. On the torso, the lesion hasan irregular surface, bright red color, sometimes scaly, with a distinct edge. Histologic examination is required

Melasma
Hyperpigmentation area on the face with brownish patches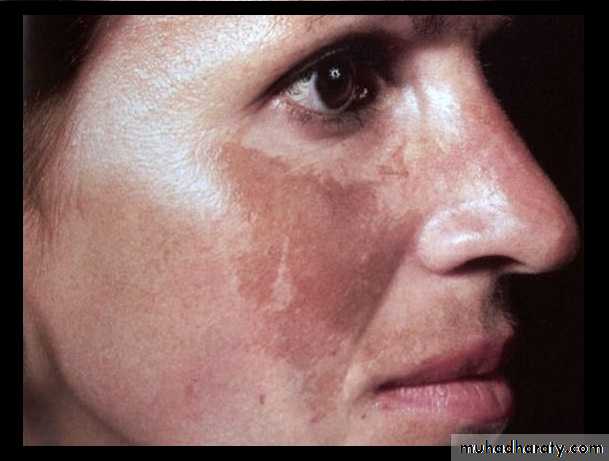
Vitiligo
depigmented patches, well demarcated with irregular margins. The affected skin is non-scarring with NO scale. May occur in hairy on non-hairy (difficult to treat)skin. It is an autoimmune disease affecting the melanocyte. DDx Pitryasis Alba, Tinea vercicolor, post. Inflammatory hypopigmentation. Treatment topical or systemic steroid (depend on surface area affected), photosensitizer (psoralin or PUVA), tacrolimus (immunomodulator).
Scabies
Erythematous papules, vesicle, pastule, burrows, crust, itching (at night). Mite infestation, sarcoptes scabes. DDx Contact dermtits, pitryasis rosea, psoriasis. Sites of predilection: genetalia, paraumbilical region, breast, gluteal region, flexor surface, axillae and finger webs (burrows). Note: the face palms and soles are spared in adults and only involved in infants. Treatment 1. Boiling, ironing or putting on sun light (for3-4 days) of clothes and bed mattresses. 2. Treat all family members (even if have NO itching) 3. Good hygienic measures 4. Topical steroids, systemic anti-histamine for itching 5. Scabicidals topical permithrin or 10% sulfer preparation for 3 days + vasalin. Failure of treatment may be due to inappropriate drug compliance, no family treatment, resistance, no hygiene, recurrent infection or exposure to the same cause.
Scabies
Erythematous papules, vesicle, pastule, burrows, crust, itching (at night). Mite infestation, sarcoptes scabes. DDx Contact dermtits, pitryasis rosea, psoriasis. Sites of predilection: genetalia, paraumbilical region, breast, gluteal region, flexor surface, axillae and finger webs (burrows). Note: the face palms and soles are spared in adults and only involved in infants. Treatment 1. Boiling, ironing or putting on sun light (for3-4 days) of clothes and bed mattresses. 2. Treat all family members (even if have NO itching) 3. Good hygienic measures 4. Topical steroids, systemic anti-histamine for itching 5. Scabicidals topical permithrin or 10% sulfer preparation for 3 days + vasalin. Failure of treatment may be due to inappropriate drug compliance, no family treatment, resistance, no hygiene, recurrent infection or exposure to the same cause.
Scabies
Burrow on the skin
Scabies
Erythematous papules, vesicle, pastule, burrows, crust, itching (at night). Mite infestation, sarcoptes scabes. DDx Contact dermtits, pitryasis rosea, psoriasis. Sites of predilection: genetalia, paraumbilical region, breast, gluteal region, flexor surface, axillae and finger webs (burrows). Note: the face palms and soles are spared in adults and only involved in infants. Treatment 1. Boiling, ironing or putting on sun light (for3-4 days) of clothes and bed mattresses. 2. Treat all family members (even if have NO itching) 3. Good hygienic measures 4. Topical steroids, systemic anti-histamine for itching 5. Scabicidals topical permithrin or 10% sulfer preparation for 3 days + vasalin. Failure of treatment may be due to inappropriate drug compliance, no family treatment, resistance, no hygiene, recurrent infection or exposure to the same cause.
Scabies
Erythematous papules, vesicle, pastule, burrows, crust, itching (at night). Mite infestation, sarcoptes scabes. DDx Contact dermtits, pitryasis rosea, psoriasis. Sites of predilection: genetalia, paraumbilical region, breast, gluteal region, flexor surface, axillae and finger webs (burrows). Note: the face palms and soles are spared in adults and only involved in infants. Treatment 1. Boiling, ironing or putting on sun light (for3-4 days) of clothes and bed mattresses. 2. Treat all family members (even if have NO itching) 3. Good hygienic measures 4. Topical steroids, systemic anti-histamine for itching 5. Scabicidals topical permithrin or 10% sulfer preparation for 3 days + vasalin. Failure of treatment may be due to inappropriate drug compliance, no family treatment, resistance, no hygiene, recurrent infection or exposure to the same cause.
Herpes simplex
Multiple vesicles
Herpes simplex
Grouped and painful vesicles with erythematous rim below the border of the lower lip
Herpes simplex
Grouped and painful vesicles with erythematous rim and edema in both surface of the upper and lower lips
Topical Infection

Common warts
surface, papule, scales, some time digitated [filliform wart (finger like)]. Of many types common wart, plane wart, planter wart or filliform wart. Caused by HPV infection Site: anywhere DDx: planter wart (corn), common wart (Molluscum contangiosum). Treatment Depend on: site, size, number and pt. preference. Topical keratinolytic (salicylic acid), immunomodulator and curettage.
Common warts
surface, papule, scales, some time digitated [filliform wart (finger like)]. Of many types common wart, plane wart, planter wart or filliform wart. Caused by HPV infection Site: anywhere DDx: planter wart (corn), common wart (Molluscum contangiosum). Treatment Depend on: site, size, number and pt. preference. Topical keratinolytic (salicylic acid), immunomodulator and curettage.
Herpes simplex
Grouped and painful vesicles with erythematous rim below the border of the lower lip
Herpes zoster
Multiple erythematous papules and vesicles Red-ringed blisters occur in a dermatomal
distribution of a nerve root. Papules change
vesicles which become pustules before crusting.complication

Molluscum contagiousum
multiple fleshy or pearly white color large papule (sometimes erythematous) with central umblication (a depression seen by magnifier lens). Sites: face, trunk and gentilia. Caused by: parapox viral infection. Transmission (contagious) contact, STD. DDx warts. Treatment topical salicylate or curettage (depend on the number).
Plane wart
surface, skin or darker pigment, papule, well demarked. HPV 10, 3, 41, 28. Sites: forehead, face, arm. Occur: children, young adult (mostly due to immune suppression). DDx nevi, acne, 2ndry syphilis. Treatment topical keratolytic, retin A chemotherapy.
Plane warts
surface, skin or darker pigment, papule, well demarked. HPV 10, 3, 41, 28. Sites: forehead, face, arm. Occur: children, young adult (mostly due to immune suppression). DDx nevi, acne, 2ndry syphilis. Treatment topical keratolytic, retin A chemotherapy.
Urticaria
Small papules and patches on red skin Weal and flare Lesion with itchinG Elevation (edema), no scale, no scar, scratching marks.
Urticaria
Small papules and patches on red skin Weal and flare Lesion with itchinG Elevation (edema), no scale, no scar, scratching marks.
Urticaria
Small papules and patches on red skin Weal and flare Lesion with itchinG Elevation (edema), no scale, no scar, scratching marks.

Pityriasis rosea
Erythematous macules , plaques with scale appear in the center of the lesion the sclale form a collarate on the advancing edge of the border also called ( herald patch )
Pityriasis rosea
Erythematous macules , plaques with scale appear in the center of the lesion the sclale form a collarate on the advancing edge of the border also called ( herald patch )
Pityriasis rosea
Erythematous macules , plaques with scale appear in the center of the lesion the sclale form a collarate on the advancing edge of the border also called ( herald patch )
Psoriasis
Well demarcated highly erythematous small papules , plaques on the trunkDDx scabies, contact dermatitis and teania corporis

Psoriasis
Well demarcated erytematous papule and plaques and scaly on the back
Psoriasis
Well demarcated erytematous papule and plaques and scaly on the abdomen
Psoriasis
Well demarcated erythmatous plaques on the palmar surface of hand
Psoriasis
Cap-like very thick , scales covers the entire scalp with erythematous plaques extend to the forehead not associated with hair loss
Psoriasis
Cap-like very thick , scales covers the entire scalp with erythematous pl`ques extend to the forehead not associated with hair loss
Psoriasis
Well demarcated eythematous plaques with thick yellowish scale and desqumentation on the sites of pressure arising on the plantar surface
Psoriasis
Many depression ( nail pittings ) in the dorsum of the nail plate with distal oncholysis
Psoriasis
Many depression in the dorsum of the nail plate with distal oncholysis
Psoriasis
pink plaques, well demarcated with silver scales. Possible causes: Genetic, autoimmune, infection of unknown, increase keratinocyte. Sites of predilection: Extensor surfaces (especially elbows and knees), scalp and nails. Nail finding: coarse pitting, onycholysis, oily spot. DDx scabies, contact dermatitis and teania corporis. Treatment depend on severity, chronicity and age of pt. : 1. Topical therapy: steroid (Systemic steroid is contraindicated as it causes flaring up of the disease), Vit. D, retinoic acid and salicylic acid (kerationlytic).