
بسم الله الرحمن الرحيم
1
2
3
4
5
6
7
SYMPTOMS
PAINSTIFFNESS
DEFORMITY
SWELLING
LIMPING

8
Normal Knee – Anterior, Extended
9
Surface Anatomy - Anterior, Extended*
10
Patella
Hollow
IndentedNormal Knee – Anterior, Flexed
11
Surface Anatomy - Anterior, Flexed
12
Head
Of
Fibula
Patella
TibialTuberosity
Palpation – Anterior*
13Patella:
Lateral and Medial Patellar FacetsSuperior
And
Inferior
Patellar Facets
Patellar Tendon**
Lateral Fat PadMedial Fat
Pat
Surface Anatomy - Medial

14
Medial
Femoral
Condyle
Patella
JointLine
Medial
Tibial
Condyle
Tibial
TuberosityPalpation - Medial
15Medial Collateral Ligament (MCL)*
Pes anserinebursa**
Medial joint
lineSurface Anatomy – Lateral

16
Patella
Head
OfFibula
Tibial
TuberosityQuadriceps
Palpation – Lateral*17
Lateral joint
lineLateral Collateral
Ligament (LCL)**How to Start
• IPEEP
• INTRODUCE.
• PERMISSION.
• EXPLANTION.
• EXPOSURE.
• POSITION.
18
The Apley System
All joint examinations follow this system:Look
Feel
Move : Active then Passive
Special Tests
Radiograpgy.
19
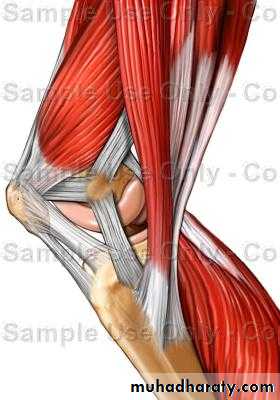
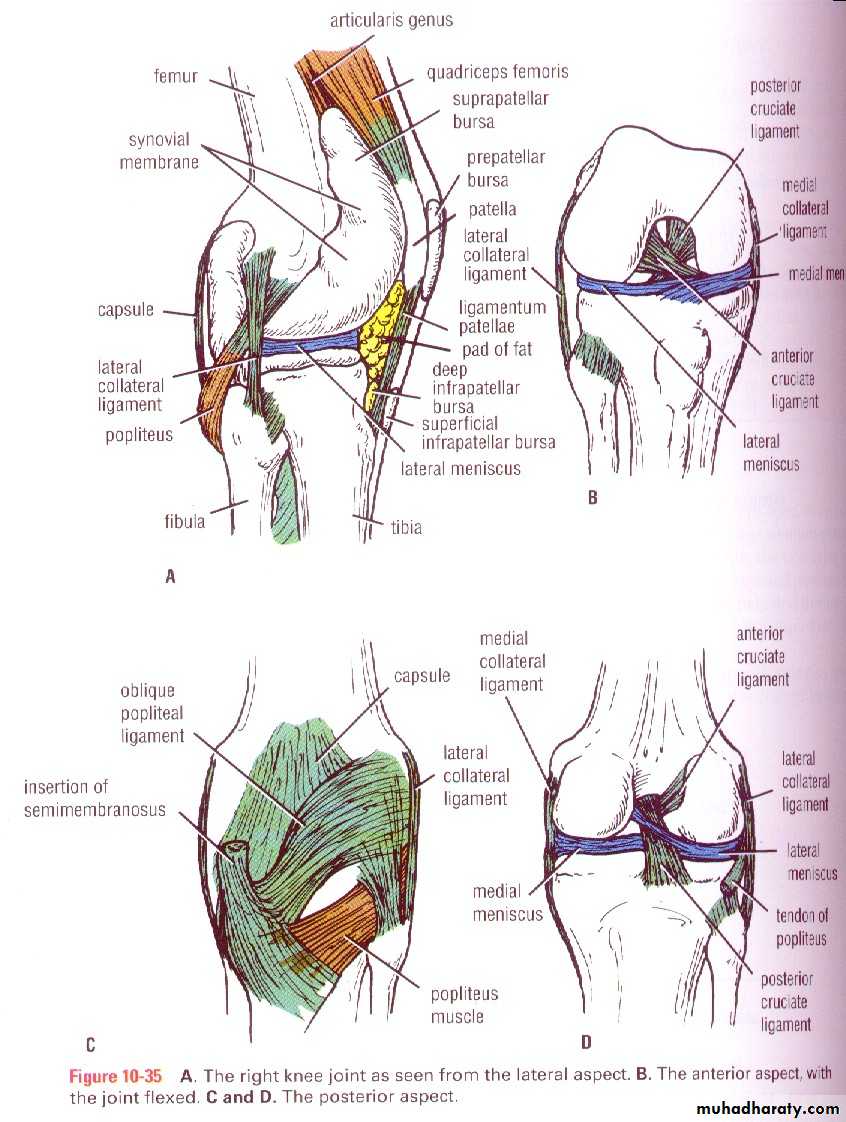
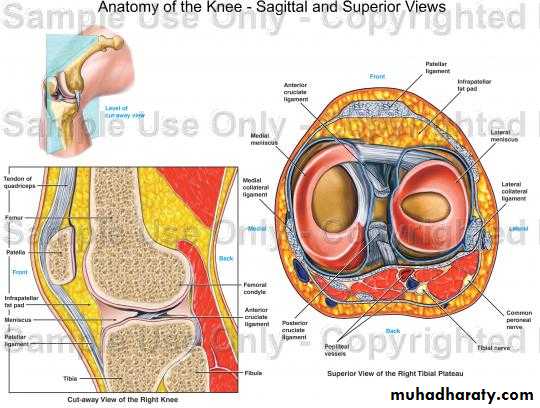
LOCAL EXAMINATION OF THE THIGH AND KNEE
20Inspection (LOOK)
Bone contours and alignment
Soft-tissue contours
Colour and texture of skin
Scars or sinuses
21
22

23

24
Instability - Example

25
http://www.carletonsportsmed.com/Libraria_medicus/PF_patella_dislocation.JPG
Patellar dislocation

26

27
diffuse swelling of the knee can
arise only from three fundamentalcauses:
I) thickening of bone;
2) fluid within the joint;
and
3) thickening of the synovial membrane

28
Distinction between effusions of blood, serous fluid, and pus is
madepartly from the history,
partly from the clinical examination.
29
(haemarthrosis)
Aneffusion of blood appears within an hour or two of an
injury and rapidly becomes tense.
30
clear fluid
An effusion developsslowly (twelve to twenty-four hours) and is never so tense as a blood.
An effusion of pus is associated with general illness and
31
Palpation (FEEL)
Skin temperatureBone contours
Soft-tissue contours
Local tenderness
32

33

34

35

36
Measurement of thigh girth
Comparative measurements at preciselythe same level In each limb.
(Note particularly the bulk of the quadriceps muscle)
37
Movements (active and passive)
against normal knee for comparison)38
? Pain on movement
? Crepitation on movement
39
Flexion.
patients can flex enough to bring the heel in contact with the buttock.The range of the sound knee must be taken as the normal for the individual.
40
41

42
43
Extension
It is wrong to accept 0 degrees as the start in point of movement:therefore the range on the sound side must be taken as the yardstick of
44
Power
(tested against resistance of examiner)Flexion
Extension
45
Stability
Medial ligamentLateral ligament
Anterior cruciate ligament
Posterior cruciate ligament
46
Tests for stability
47Testing the medial and lateral ligaments.

48
Collateral Ligament Assessment
49
Patient and Examiner
Position*
Valgus Stress Test for MCL*
50Note Direction Of Forces
Varus Stress Test for LCL*51

• Note direction of forces
Rotation tests (McMurray)(Of value mainly when a torn
meniscus is suspected)
52

53

54
The maneuver is carried
out by repeatedlyI) flexing the knee, first fully but in succeeding tests progressively less fully
then
2) rotating the tibia upon the femur, first laterally but in further tests medially;
and finally
3) extending the knee while the rotation of the tibia is still
maintained.
55
A loud click,
distinct from the normal patellar click and usually associated with pain,suggests a tag tear (not a 'bucket-handle‘ tear) of a meniscus.
56Testing the anterior and posterior cruciate ligaments.
57Anterior Drawer Test for ACL
Physician Position & Movements*Patient Position
58

• Note direction of forces
Posterior Drawer Testing- PCL*
59• Note direction of forces

60
Stance and gait
61EXAMINATION OF POTENTIAL EXTRINSIC SOURCES OFTHIGH OR KNEE SYMPTOMS
This is important if a satisfactory explanation for the symptoms is not found on local examination.The investigation should include:
I) the spine.
2) the hip.
62
GENERAL EXAMINATION
General survey of other parts of the body.The local symptoms may be only one manifestation of a widespread disease.
63
CLASSIFICATION OF DISORDERS OF THE THIGHAND KNEEDISORDERS OF THE THIGH
64INFECTIONS
Acute osteomyelitisChronic osteomyelitis
Syphilitic infection
65

66
TUMOURS
Benign bone tumorsMalignant bone tumors
67

68
ARTICULAR DISORDERS OF THE KNEE
ARTHRITISPyogenic arthritis
Rheumatoid arthritis
Tuberculous arthritis
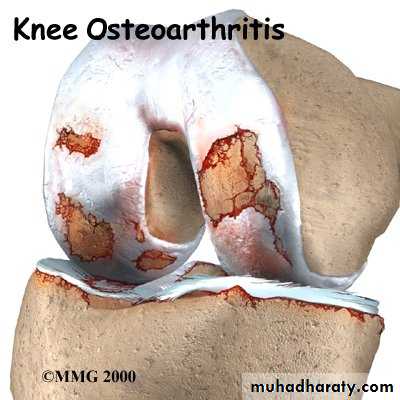
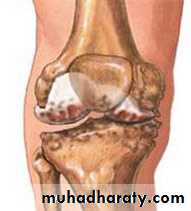
Osteoarthritis
Haemophilic arthritis
Neuropathic arthritis
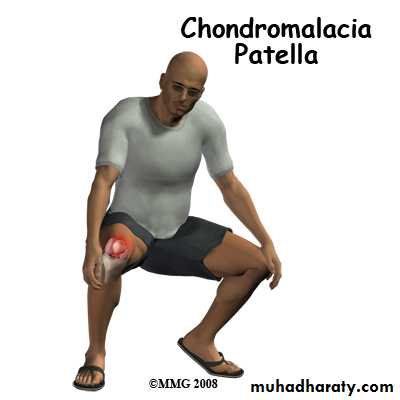
Chondromalacia of the patella
69

70
71

72
MECHANICAL DISORDERS
Tears of the menisciCysts of the menisci
Discoid lateral meniscus
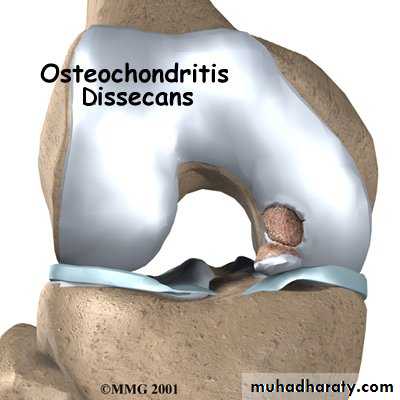
Osteochondritis dissecans
Intra-articular loose bodies
Recurrent dislocation of the patella
Habitual dislocation of the patella
73
74
http://www.carletonsportsmed.com/Libraria_medicus/PF_patella_dislocation.JPG
Patellar dislocation
75
EXTRA-ARTICULAR DISORDERS IN THE REGIONOF THE KNEE
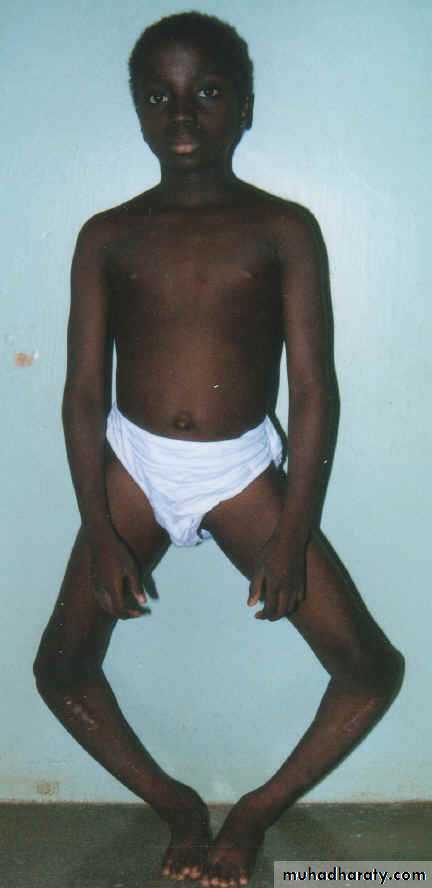
DEFORMITIESGenu varum
Genu valgum
76

77
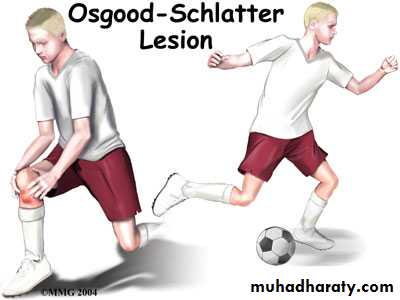
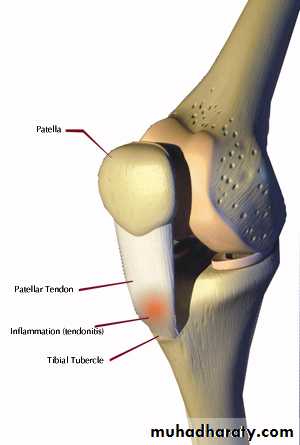
INJURIES
Rupture of the quadriceps apparatusOsgoodSchlatter's disease
78
79

80
81

82
83
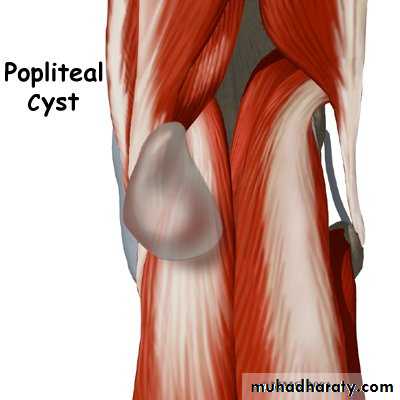
CYSTIC SWELLINGS
Prepatellar bursitisPopliteal cysts
84
85
POST-TRA UMA TIC OSSIFICATION
Pellegrini-Stieda's disease of the medial femoralcondyle

86