1
Fifth stage
ENT
Lec-11
د.سعد
7/12/2015
Investigations of laryngeal diseases
History: age, sex, occupation, mode of onset and duration of illness, habits and associated
symptoms...etc. Any hoarseness persisting for more than 3 weeks deserves examination of larynx.
Malignancy should be excluded in patient above 40 years.
General examination: complete ENT examination including neck and chest. Examination of the
larynx: by laryngeal mirror (indirect laryngoscopy), to asses mobility of the vocal cords, any
swelling or ulceration.
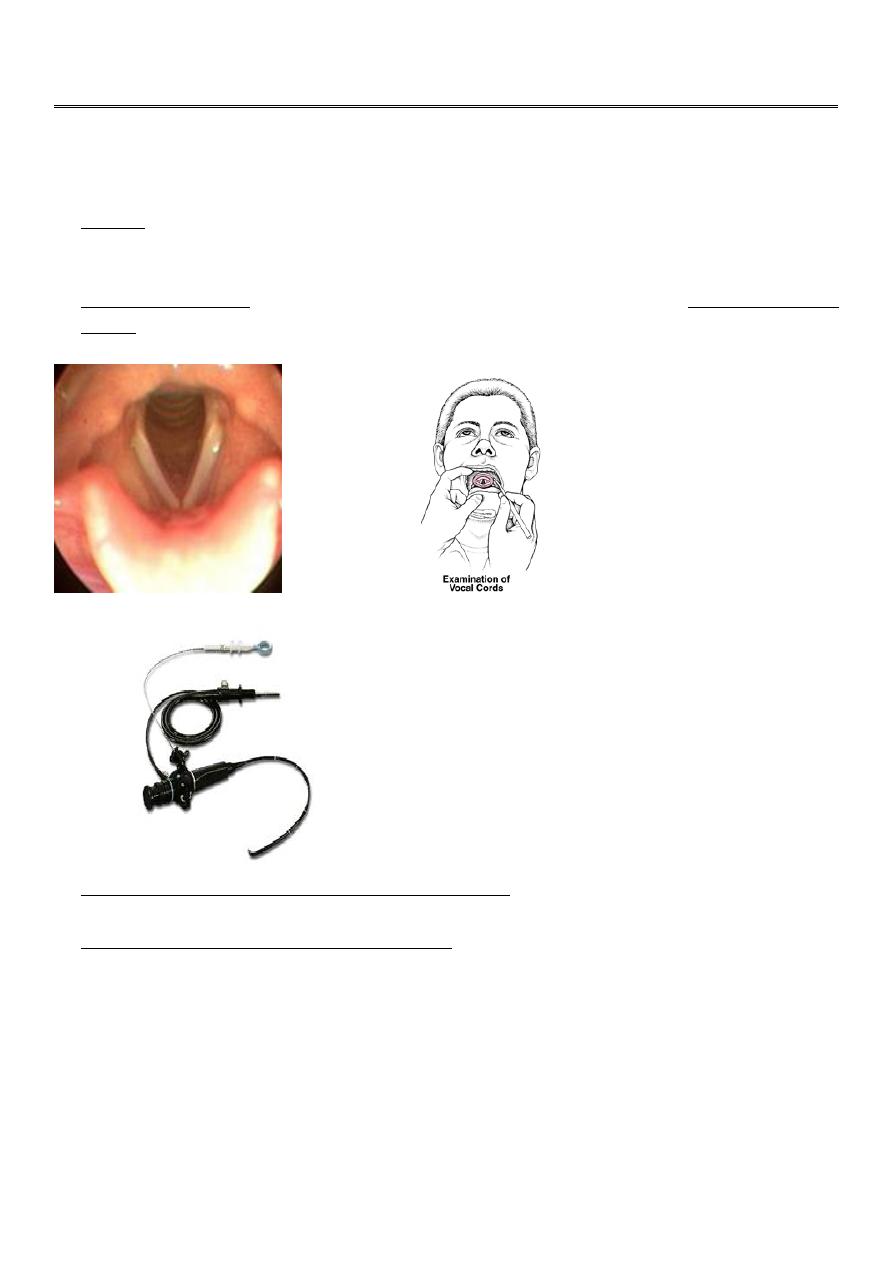
Normal Larynx
The flexible laryngoscope is probably the
tool that most otolaryngologists rely upon
in the evaluation of the dysphonic
patient. It is the sole method that allows
examination of the nasopharynx, palate,
larynx, and pharynx in a near physiologic
position. It can be performed relatively
easily even in patients with hyper-
responsive gags and pediatric patients.
Laboratory investigations and radiological examination should be done as per dictates of the cause
suspected on clinical examination.
Direct Laryngoscopy and Hypopharyngoscopy: done under GA for two purposes:
1. Diagnostic: in young children and in adults when indirect laryngoscopy is unsatisfactory, and
to take biopsy when there is a suspicion of tumor.
2. Therapeutic: removal of F.B., small benign and malignant tumors, Singer's nodule…
Symptoms of laryngeal disease:
1. Hoarseness
2. Stridor
3. Cough
4. Expectoration.
5. Pain(local and referred)
6. Dysphagia
2
Hoarseness: this is a change of voice from high to low pitch (roughness of voice), and may even ends
with aphonia.
Stridor: A noisy breathing or abnormal sound produced through partially obstructed airways.
Types of stridor:
1. Inspiratory: the cause is usually in the larynx.
2. Expiratory: the cause is below the larynx.
3. Mixed: The cause is laryngeal and bronchial (as laryngotracheobronchitis).
Cough: a frequent complaint in laryngeal diseases. Cough is either dry or productive. In case of
foreign body inhalation cough comes in paroxysms of convulsive nature. In hysterical cases it is
repeated and effortless.
Expectoration: may be mucous (catarrhal laryngitis), mucopurulent or blood stained (malignant
tumors).
Pain: Cancer, arthritis and perichondritis give rise to pain. Laryngeal pain is usually referred to the
ear (via auricular branch of the vagus (Arnold's nerve).
The larynx may also ache in voice strain.
Dysphagia: (1) swelling of arytenoids leads to partial obstruction of the mouth of oesophagus. (2)
When vocal cords fail to meet with the result that food tends to enter the trachea giving rise to bouts
of coughing. (3) Severe laryngeal pain (e.g. laryngeal TB) is associated with dysphagia. (4) A tumor
of the larynx may extend to the hypopharynx causing dysphagia.
Hoarseness
is the most important symptom of laryngeal disease. It always originates in the larynx
so that any patient who is hoarse must have something wrong with the larynx.
For production of normal voice, vocal cords should:
1. Be able to approximate properly with each other.
2. Have proper size and stiffiness.
3. Have the ability to vibrate regularly in response to air column.
Cause of Hoarseness
a. Congenital : laryngeal web , cyst , laryngocele
b. Paralysis : paralysis of recurrent laryngeal nerve, superior laryngeal or both nerves
c. Inflammation : acute & chronic laryngitis, laryngo-tracheo-bronchitis, diphtheria, acute
epiglottitis
d. Neoplastic: vocal cord polyps, nodules, granuloma, cysts, laryngeal carcinoma, leukoplakia.
Common causes:
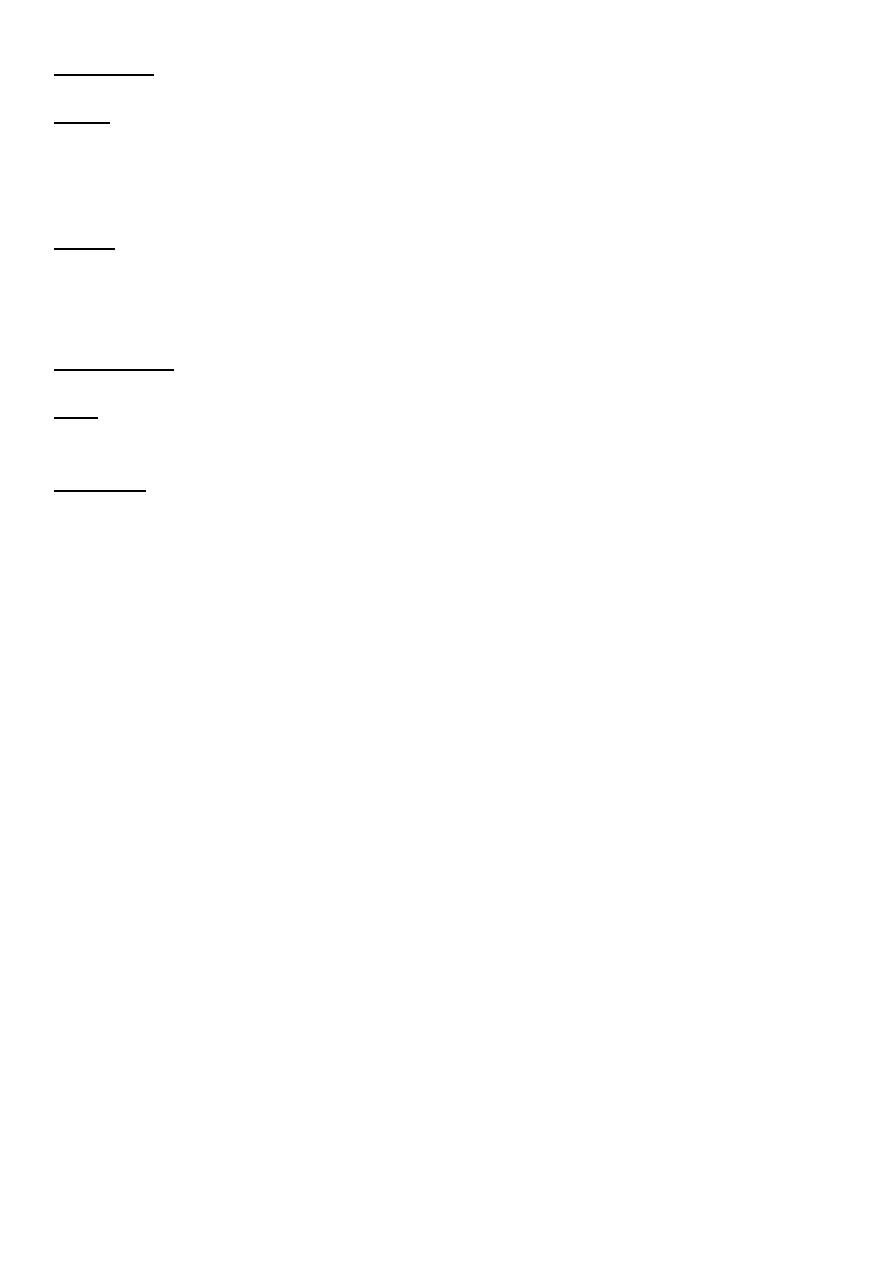
1. Singer's nodule (screamer nodule): these are bilateral small and grayish-white nodules at the
junction of the anterior 1/3 with the posterior 2/3 of the vocal cords due to voice abuse (as this is
the area of maximum vibration of the cord and thus subject to maximum trauma).
Traumaoedema&haemorrhage in submucosal spacethis undergoes hyalinization and fibrosis
and the overlying (stratified squamous) epithelium undergoes hyperplasia.
Treatment: Small nodule; speech therapy. Large nodule; endoscopic removal.
3
Singer' Nodule
2. Vocal cord polyp: It is probably the most
common laryngeal mass. Aetiology is not
well understood but it may be due to: vocal
abuse, allergy and smoking. Mostly, it
affects men in the age of 30-50. Treatment
is by endoscopic removal.
3. Acute laryngitis usually occurs as part of a generalized URTI. It often develops after common cold.
It is usually viral but bacterial infection may supervene. There is diffuse inflammation of the
laryngeal mucosa and oedema of its lax parts above and below the vocal cords. In young children
this may cause respiratory obstruction. Duration is short lived, 4-5 days. The patient c/o malaise, pain
on speaking, redness and swelling of the larynx.
Treatment: Is symptomatic; Voice rest, steam inhalation and avoidance of irritant (alcohol smoking
and fumes) and analgesics. Antibiotics (e.g. amoxicillin is prescribed if secondary bacterial infection
is suspected.
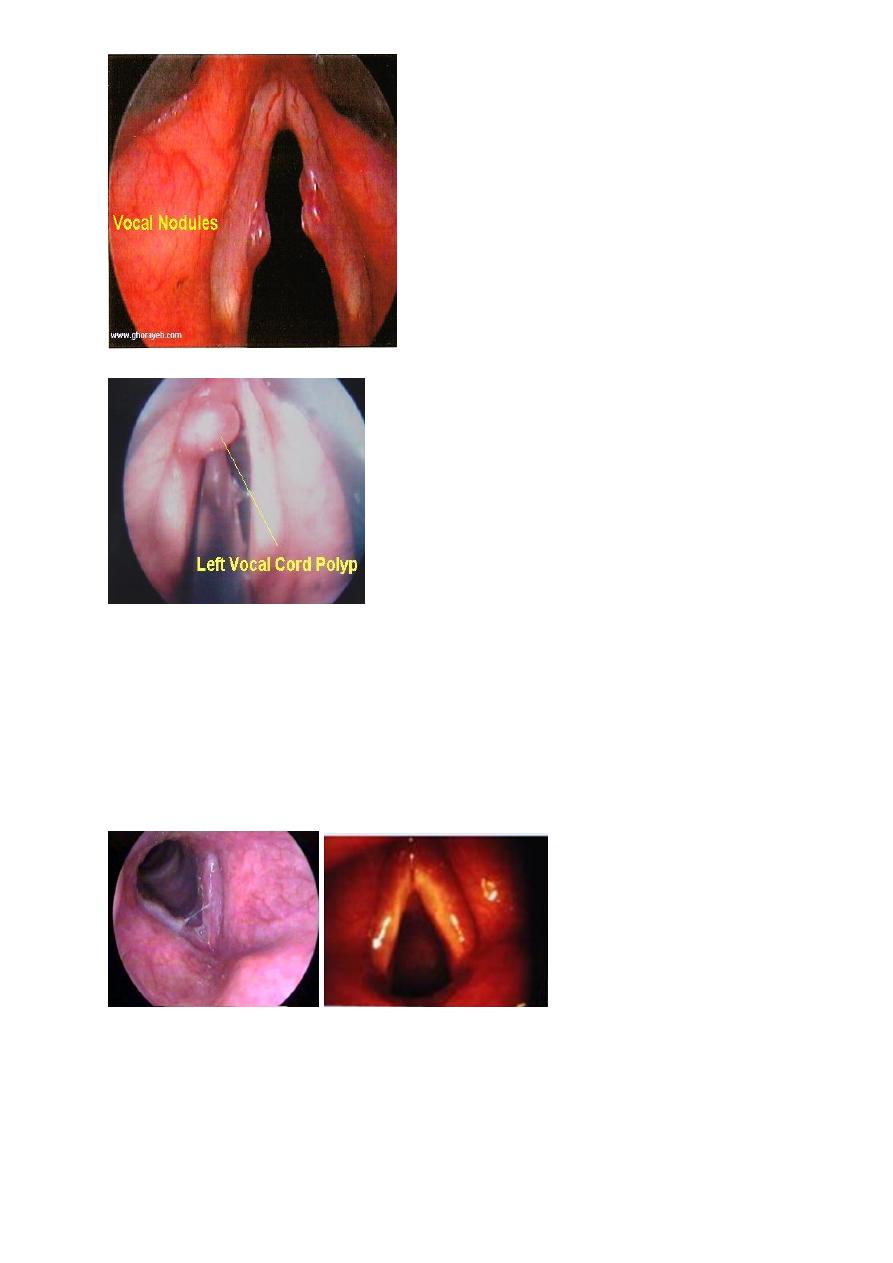
Acute Laryngitis
4. Chronic laryngitis:
A. Non-specific laryngitis: The larynx separate
the upper from the lower respiratory tract; it
may therefore be affected by diseases from
the upper and lower respiratory tracts.
Commonest disorders are chronic sinusitis,
nasal polyps, and severely deviated nasal
septum: the discharge pass down to irritate
the larynx and also cause mouth breathing
4
(with snoring). Lower respiratory disorder
associated with chronic laryngitis is chronic
bronchitis. Other causes are smoking,
drinking and GERD.
B. Specific laryngitis: TB, Syphilis and
Hyperkeratosis.
Chronic Laryngitis
5. Laryngeal tumors:
Benign: Papilloma (most common). Chondroma and haemangioma rarely affect the larynx.
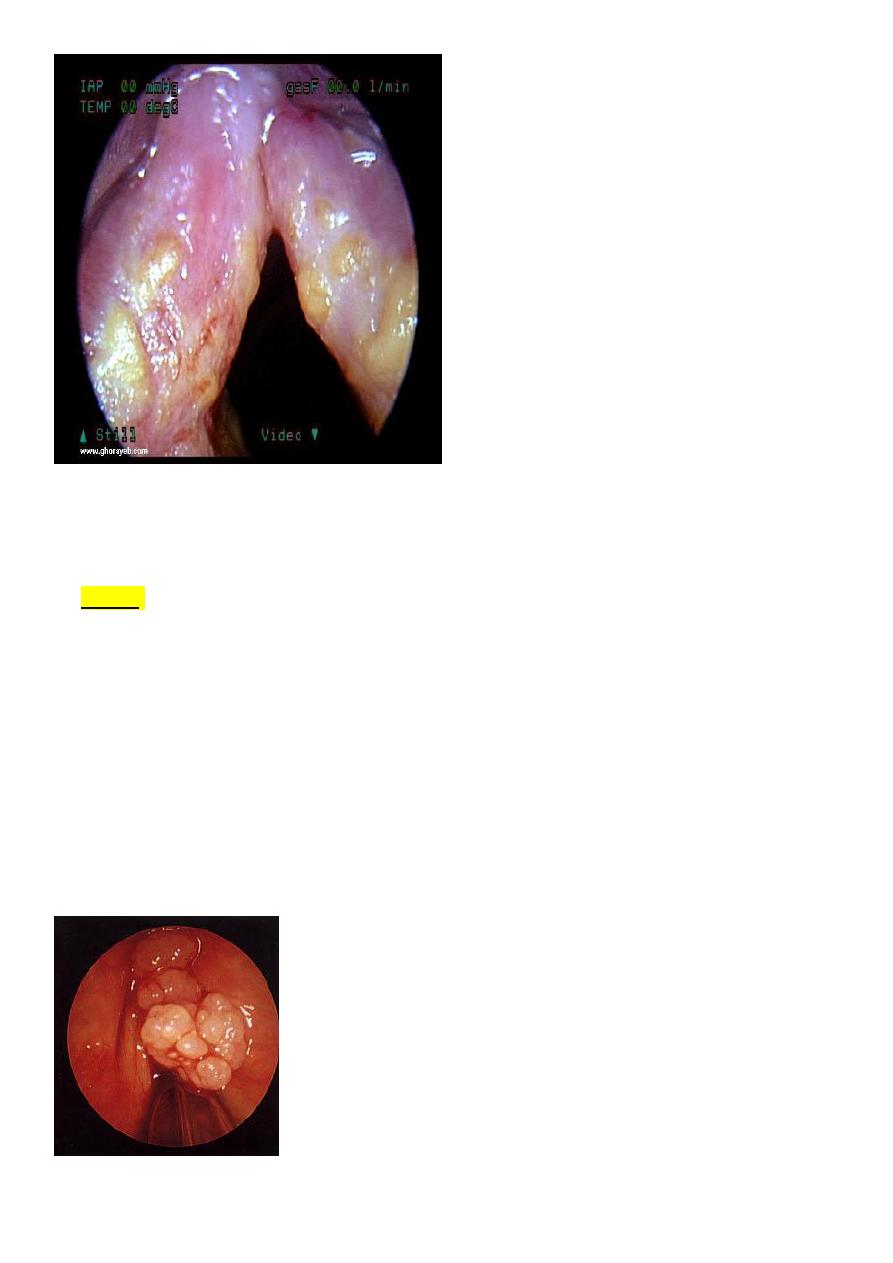
Laryngeal Papilloma
The most common benign neoplasms of the larynx (84% of benign tumors).
Aetilogy: mucosal infection by a papovavirus.
It is of 2 types:
1- Juvenile form:
Diffuse & extremely aggressive
hoarseness and stridor.
Resistant to treatment
frequent laryngoscopies. They are not premalignant but the larynx
may be severely damaged from repeated removals.
2- Adult-onset form: solitary, less aggressive, liable to recurrence and may undergo malignant
changes.
Treatment: CO2 laser, cryotherapy, XRT, interferon.
Laryngeal paplloma

5
Malignant tumors:
The most common type is squamous cell carcinoma. The larynx is the most common site for CA
in the upper aerodigestive tract (5per100 000).
Carcinoma of the larynx
Squamous cell Carcinoma (SCCA) is the most common laryngeal Ca (>90%).
Sex: Male: female = 6:1.
Age: middle-aged and elderly.
Aetiology:
1- Tobacco
2- Alcohol
3- Previous radiation to neck for benign lesions.
4- Occupational exposure to asbestos, mustard gas and other chemical or petroleum product.
Site of origin:
Glottic SCCA: most common (60%) > supraglottic SCCA (30%) > subglottis SCCA (<10%).
Clinical picture:
Symptoms:
1. Progressive and unremitting hoarseness
2. Dyspnoea
3. Stridor
4. Pain / Referred otalgia
5. Dysphagia
6. Cough and irritation
7. Neck swelling
8. Haemoptysis, Anorexia and Cachexia.
Signs:
A. Examination of laynx
External examination + Mobility
Indirect laryngoscopy.
Flexible laryngoscope.
B. Examination of the neck
C. Examination of ear, nose and throat
D. Systemic examination.
Investigation:
Direct larygoscopy & biopsy.
CT +/- MRI
Spread of tumor:
1- Local:
Involves other divisions of the larynx
Spread beyond the larynx to involve tongue, trachea, pyriform sinus, oesophagus, thyroid etc.
2- Regional: To the cervical lymph nodes
3- Distant: Lung, liver, brain and bone.
Treatment:
Radiotherapy has the advantage of preserving voice and it is indicated for small tumors with no
cervical lymph nodes. Larger tumors associated with cervical lymph nodes should be managed by
total laryngectomy and radical neck dissection with postoperative radiotherapy. Advanced tumors
need palliative treatment only.

6
Paralysis of the vocal cords:
The recurrent laryngeal nerve is the motor nerve to all the laryngeal muscles except the cricothyroid
muscles which is supplied by the external branch of the superior laryngeal nerve. This latter muscle
has an adductor effect on the vocal cords, and thus a lesion which spares the superior laryngeal
nerve will leave the cord lying nearer the midline than one which paralyses both the recurrent and
superior laryngeal nerves.
Types of paralysis:
Incomplete: the abductor group is paralyzed; position of vocal cords is near the midline e.g. thyroid
surgery.
Complete: both abductor and adductor muscles are paralyzed: position of vocal cords is half way
(cadaveric position).
The recurrent laryngeal nerve runs a different course between right and left: the right arises in the root
of the neck, while the left arises in the mediastinum at the arch of the aorta. The chance is twice for
the left recurrent nerve to be paralyzed than the right. Bronchogenic carcinoma is an important cause
of left recurrent paralysis and should always be excluded by X-ray chest, bronchoscopy and biopsy.

7