Urology
For
5
th
stage
http://goo.gl/rjRf4F
I
LOKA
©
http://www.muhadharaty.com/urology
I
Content
Topics:
Page:
Symptoms of urinary tract
3
Bladder outflow obstruction
6
Hematuria
8
Urinary stones
11
Management of renal colic
14
Uremia
16
Urinary injury
18
Scrotal pathology
20
Folly's catheter
23
Imaging study "KUB"
25
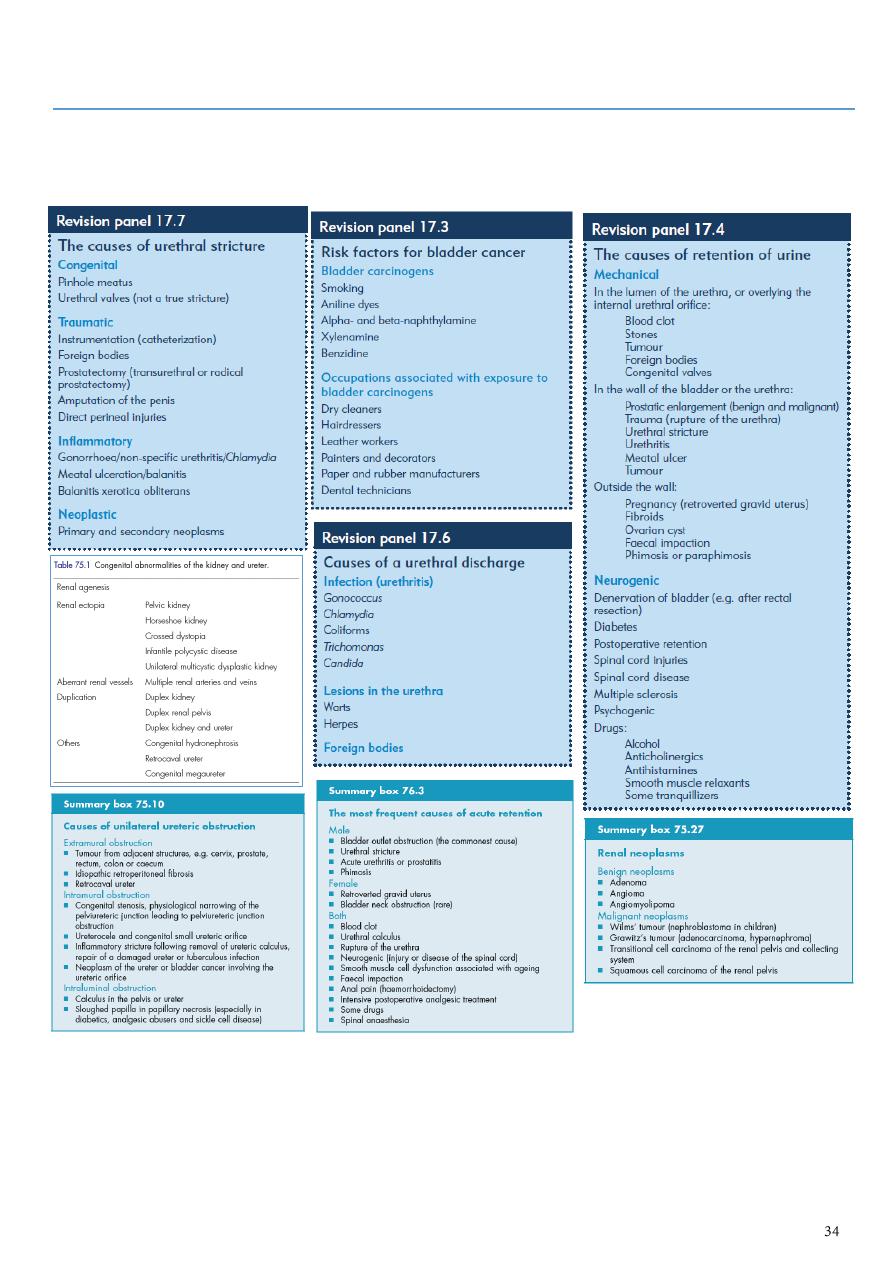
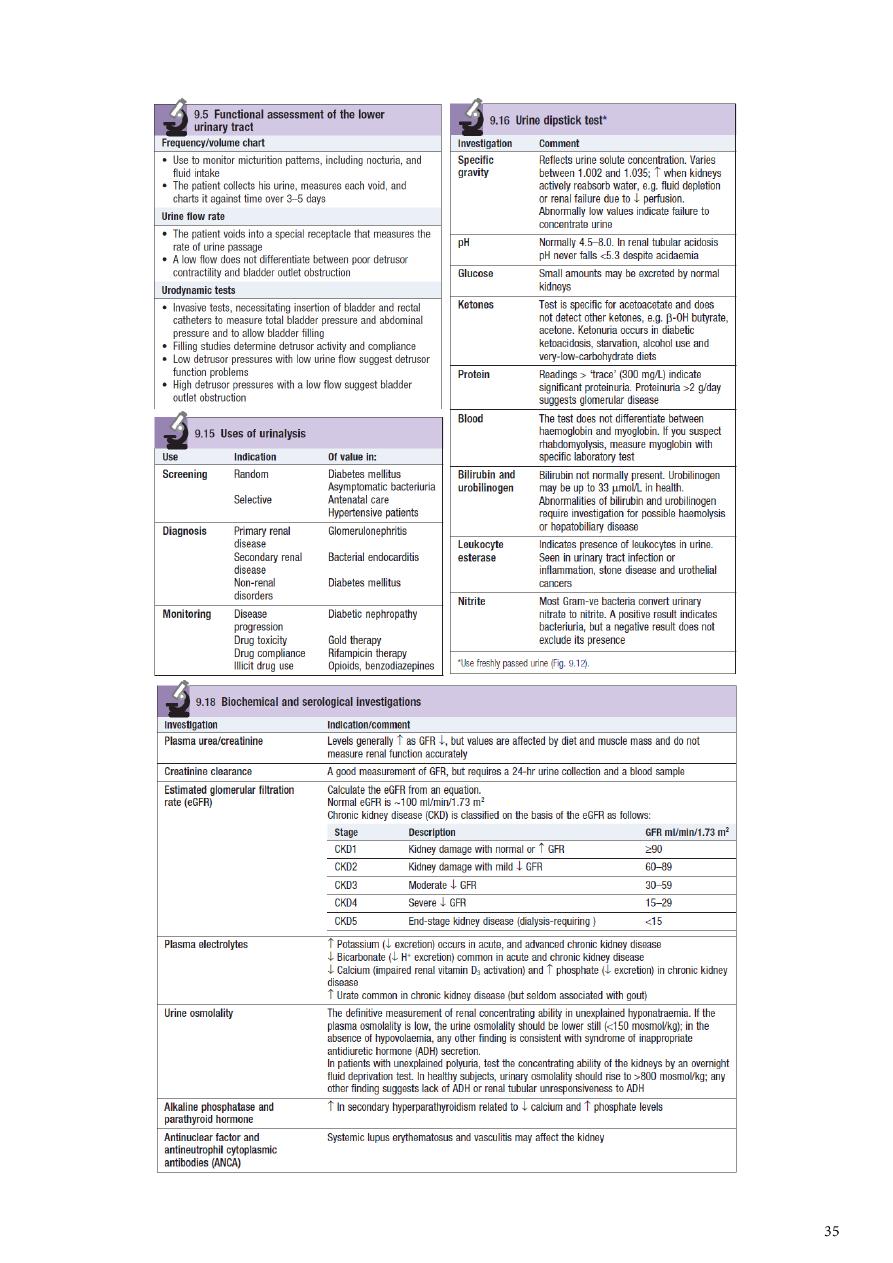
Extra
34

Part1
: Symptoms of urinary tract
1- Pain:
Renal pain:
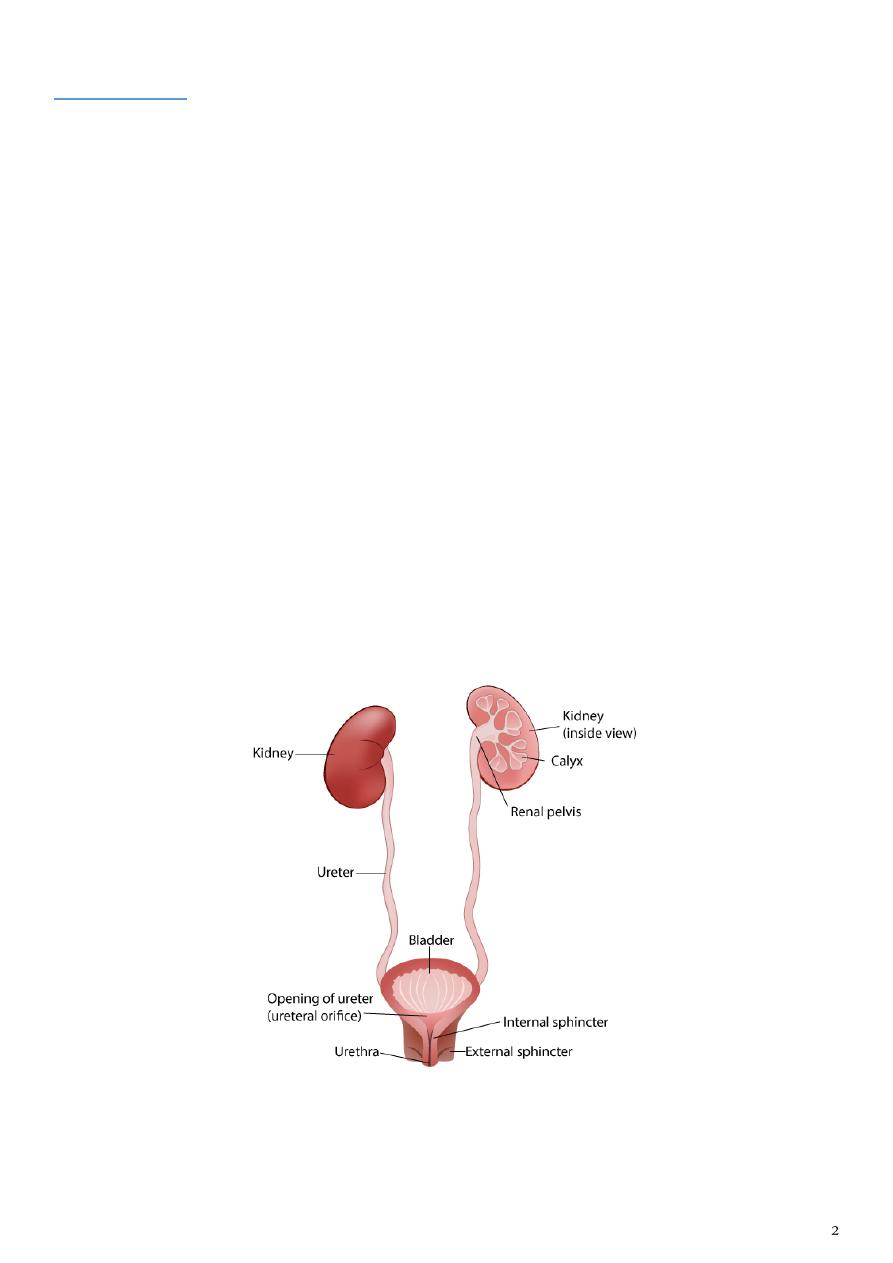
o Pain from the kidney is typically felt in the loin (the space below the 12th rib
and the iliac crest), renal angle (the angle between the 12th rib and the edge of
the erector spinae muscle)
o Renal pain can be a continuous dull ache or be sharp and very severe.
o Do not use the term ‘renal colic’.
Ureteric colic:
o Pain from the ureter is felt along the line of the ureter.
o It is a true colic, griping in nature and coming in waves, with pain-free periods
between attacks.
Bladder pain is a suprapubic discomfort worsened by bladder filling.
Perineal pain this is experienced as a penetrating ache in the perineum and
rectum, sometimes with associated inguinal discomfort.
Urethral pain is a scalding or burning felt in the vulva or penis, especially during
voiding.
Pain is urology is classified into:
Dull aching pain is a fixed continuous pain varies from mild to severe according to
the onset and severity of the condition, usually felt in the renal angle and may radiate
to the hypochroderium or epigastrium. This pain is caused by stretching of the renal
capsule e.g. hydronephrosis, polycystic kidney, tumor and trauma.
Colicky pain is a severe pain initiated in the lion, radiate to the groin, because of
the peristalsis it comes and go in attacks. It is severe enough to make the patient
rolling around, associated with nausea and vomiting. Usually it is caused by ureteric
obstruction, and the causes of ureteric obstruction are: Crystaluria, Calculus, Cluster
of bacteria, Clots, Cancer, Constriction of ureter, Compression of ureter, Conception,
Papillary necrosis.
2- Irritative symptoms:
Frequency micturition more often than a patient’s expectations.
Nocturia waking up at night to void urine.
Dysuria painful urination, often described as burning, scalding or stinging, and
commonly accompanied by suprapubic pain.
Urgency sudden severe desire of feeling need to urinate that patient can not stop.
3- Obstructive Symptoms:
Hesitancy difficulty starting or maintaining a urine stream.
Straining.
Intermittency.
Decreased force or caliber of stream.
Prolonged voiding.
Post-void dribble.
Incomplete emptying feeling of incomplete evacuation of the bladder.
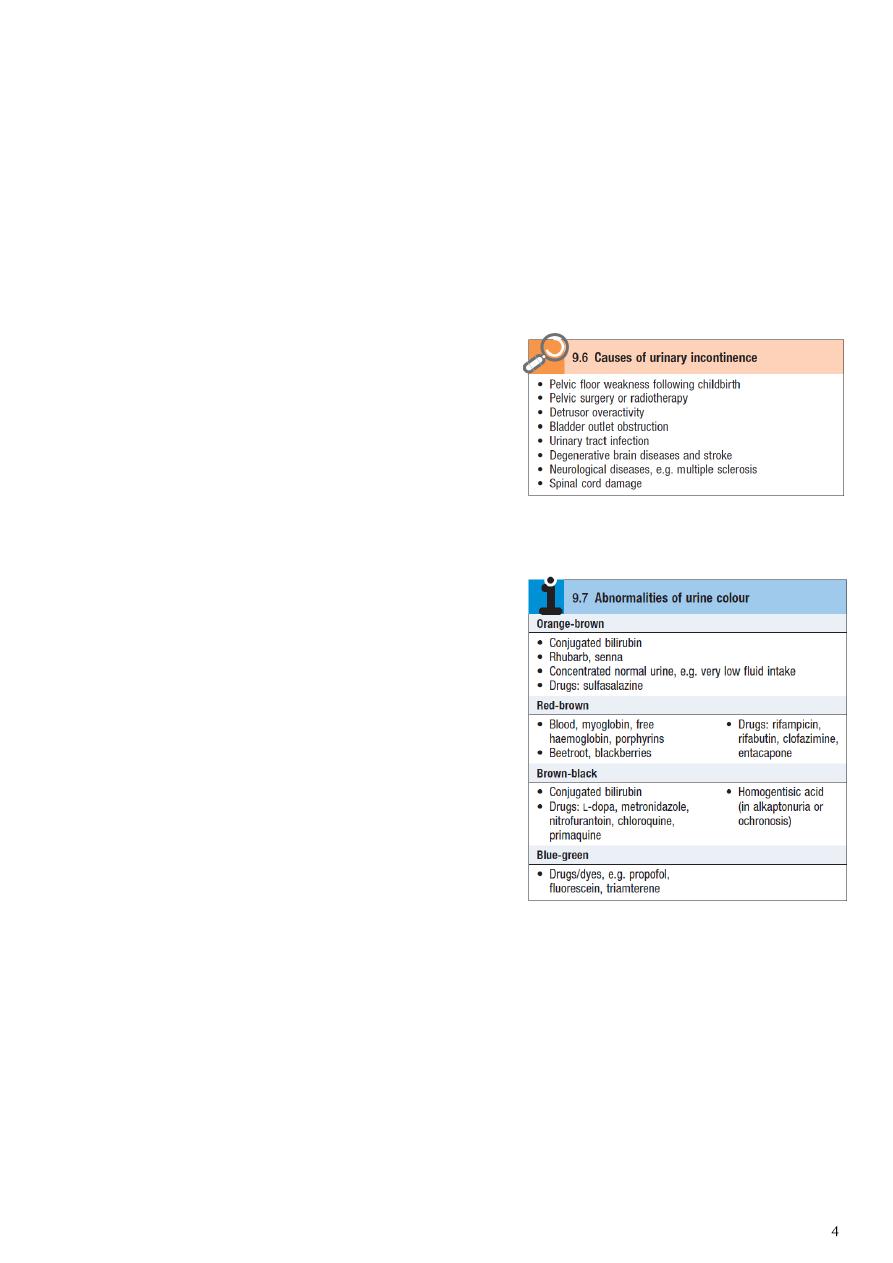
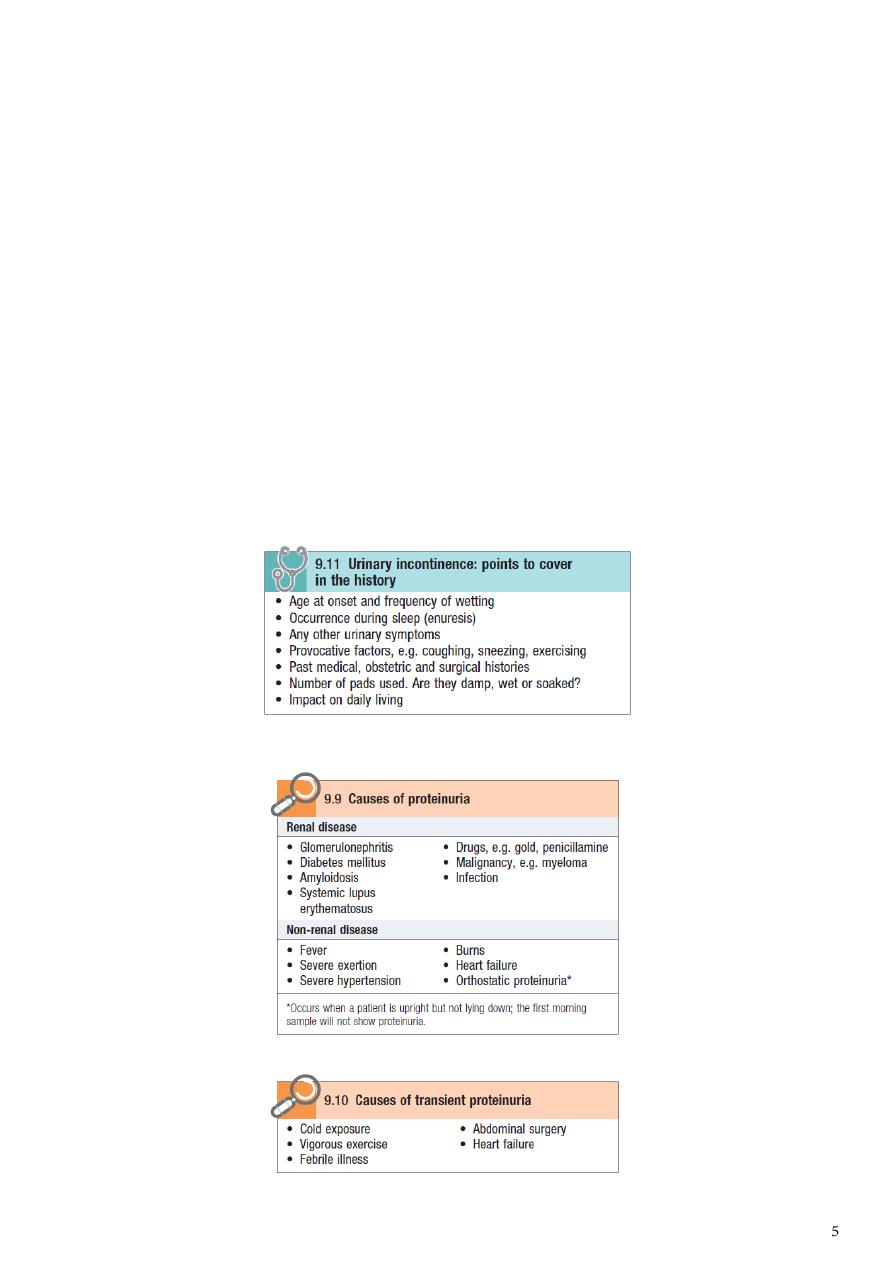
4- Incontinence:
Stress incontinence.
Urge incontinence.
Overflow incontinence.
History of neurological problems, past
pregnancies and method of delivery, past
abdominal-pelvic operations.
5- Urine:
Polyuria is an abnormally large volume of
urine, and is most commonly due to excessive
fluid intake.
Oliguria is a reduction in urine volume to
<800 ml/day.
Anuria is the total absence of urine
production.
Pneumaturia passing gas bubbles in the
urine.
Proteinuria is excess protein in urine and
indicates kidney disease.
Foul smell.
Hematuria.
Color cloudy, white, orange.
6- Constitutional symptoms:
Fever.
Chills.
Nausea.
Vomiting.
7- Cachexic symptoms:
Fatigue.
Weakness.
Significant loss of appetite.
8- Other symptoms:
Urethral discharge color, amount, smell.
Infertility.
Erectile dysfunction.
Note: In urology we depend on detailed history and investigations because the
signs and symptoms are similar in a lot of diseases.
Part2
: Bladder outflow obstruction
Differential diagnosis of obstructive symptoms:
In elderly:
Benign prostatic hyperplasia (BPH).
Prostatic cancer.
Urethral or vesical stone.
Urethral stricture.
Neurogenic bladder.
Bladder neck contracture.
Tumor in the neck of bladder.
Meatal stenosis.
In adult male:
Stricture.
Urethral stone.
Prostatitis.
Neuropathic bladder.
Bladder neck contracture.
In adult female:
Retroverted gravid uterus.
Urethral stenosis (no stricture in female).
Bladder stone.
Bladder tumor.
In children:
Posterior urethral valve.
Meatal stenosis.
Congenital urethral stricture.
Phemosis a scaring prepuce which becomes tight & can't be retracted over the glans,
occur in in un- circumcised male and lead to infection and obstructive urinary
symptoms.
Para-phemosis A tight retracted foreskin that act as a ring & is difficult to return back
normally over the glans, occur in in un- circumcised male and cause obstructive urinary
symptoms.
Note: The prototype of bladder outflow obstruction is prostate problem.
Benign prostatic hyperplasia (BPH)
Prostatic cancer
History:
Present in old age males.
BPH not risk factor for CA prostate.
Incidence increase with age.
Painless.
History:
Present in old age males (big older).
Incidence increase with age.
Painless unless it is advanced or
complicated.
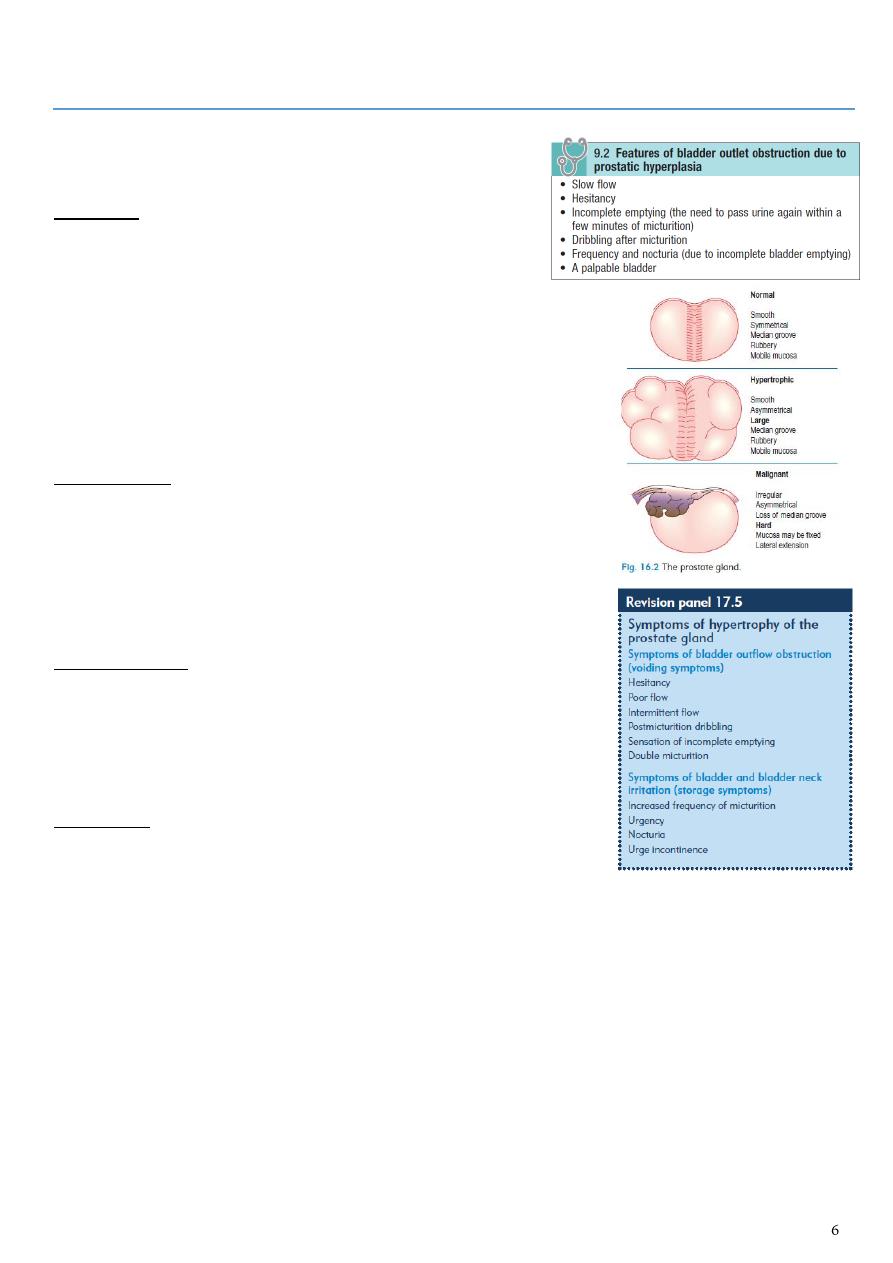
PR exam:
Smooth surface.
Firm in consistency.
Enlarged.
Preserved median sulcus.
Free mobile rectal mucosa on the
surface of the prostate.
PR exam:
Irregular surface.
Hard in consistency.
Enlarged.
Could loss of median sulcus.
Tethered rectal mucosa to the prostate.
Investigations:
PSA: Usually normal level in BPH.
Transrectal US guided biopsy (TRUS).
Lab investigations: GUE, RFT, CBC,
bleeding profile, culture and sensitivity.
Imagining: CT, KUB, IVU, US (US of
urinary tract + prostate + post void
residue) (US of the kidney to check the
complications).
Investigations:
PSA: Elevated in prostatic cancer.
Transrectal US guided biopsy (TRUS).
Trade of diagnosis of CA prostate:
1- PR exam
2- PSA
3- TRUS guided biopsy.
Treatment of BPH:
Note: the size of prostate not correlate to the symptoms of patient, and we treat the
symptom not the size!
1- Watch full waiting:
Done in patient with mild symptoms like mild nocturia and hesitancy.
Never postpone uritnation.
Avoid constipation (precipitate retention).
Avoid anti-cholinergic and anti-histamine (precipitate retention).
See the patient within 3-6 months or when something goes wrong.
2- Medical therapy:
Alpha 1 blockers (like Doxazosin) that bound to Alpha 1 a receptors in the bladder
neck and cause relaxation of bladder neck so reduce the obstruction.
5-alpha reductase inhibitors and dihydro-testosterone inhibitors that reduce the
growth of prostate, need 3-6 months, and it is useful in big prostate 40 g and more
(normal prostate size is 20-25 g).
Herbal therapy: Pumpkin Seeds.
3- Surgical therapy:
Indications:
Non-responding patient (in fibrotic prostate).
Recurrent UTI.
Recurrent and severe hematuria (lead to varicose veins around the prostate that
rapture and cause bleeding).
Renal impairment.
Stone diseases.
Patient preference and cost effectiveness.
Bladder diverticulum.
Types:
Endoscopic: Transurethral resection of the prostate (TURP) useful in 90% of cases.
Laser therapy.
Microwave therapy.
Open prostatectomy (abdominal or perineal) done in big prostate, big stone,
bladder diverticulum.
Notes
Residual urine volume is important in the treatment and follow-up.
Bladder capacity is 500 ml.
Residual urine volume in elderly: 50-100 ml is accepted.
Residual urine volume in young adult: 0 ml, should be empty bladder.
Residual urine volume in children: is not important because they cannot empty their
bladder.
Retention:
Definition inability to pass urine despite of full bladder.
Normal kidney function.
It is lower tract problem (bladder or prostate) but uremia is upper tract problem
(kidney or ureter).
Acute retention
Chronic retention
Painful.
Painless.
Happens within few hours.
Long duration.
Normal kidney function.
Renal impairment
US normal or distended kidney.
US hydro-uretero-nephrosis.
Folly's catheter: immediate release of
urine.
Folly's catheter: gradual release to avoid
hematuria.
Bladder size normal or increase 1 liter.
Bladder size increased by liters.
Part3
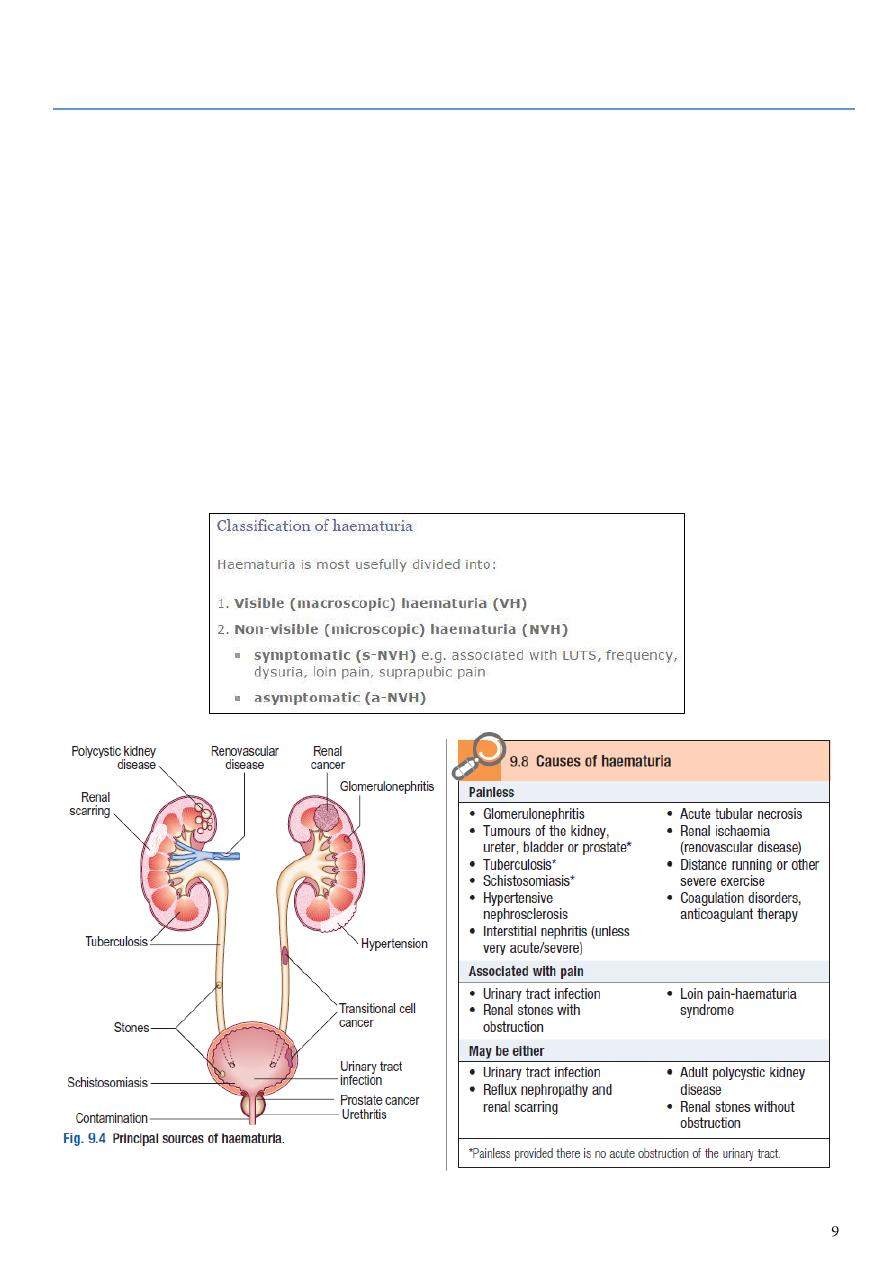
: Hematuria
Definition:
More than three red blood cells are found in centrifuged urine per high-power field
microscopy ( > 3 RBC/HP).
Normal urine: no red blood cell or less than three red blood cell
Hematuria is a symptom of many disease, it is not a diagnosis.
Severe hematuria could be presented with clots.
Classifications:
Painful or painless (in elderly could be cancer).
Initial or total or terminal.
Microscopic (normal color with eyes) or Gross hematuria (tea-colored, cola-colored,
pink or even red)
Differential diagnosis of red urine:
1- Hematuria.
2- Hemoglobinuria.
3- Myoblobinuria.
4- Porphyrins.
5- Bleeding tendency.
6- Physiological (beetroot, blackberries).
7- Drugs (rifampicin).
Causes of hematuria:
In elderly:
Malignancy (most common is bladder cancer).
UTI.
Stone.
Trauma.
BPH.
Bleeding tendency.
In adult:
UTI.
Stones.
Trauma.
Tumor.
Bleeding tendency.
Congenital anomalies (AV fistula).
Accompanied symptoms:
Hematuria with renal colic renal stone, ureter stone, if with dysuria, miction pause
or staining to void: bladder or urethra stone.
Hematuria with urinary frequency,urgency and dysuria bladder or lower urinary
tract (tuberculosis or tumor), if accompanied by high spiking fever, chill and loin pain:
pyelonephritis.
Hematuria with edema and hypertension glomerulonephritis, hypertensive
nephropathy.
Hematuria with mass in the kidney neoplasm, hereditary polycystic kidney.
Hematuria with hemorrhage in skin and mucosa hematological disorders, infectious
diseases.
Hematuria with chyluria filariasis.
Question: elderly patient who is smoker
presented with red color urine, how to
diagnose hematuria? What is the DDx?
How to diagnose by microscope.
DDx malignancy, UTI, stones,
trauma, BPH, bleeding tendency.
Part4
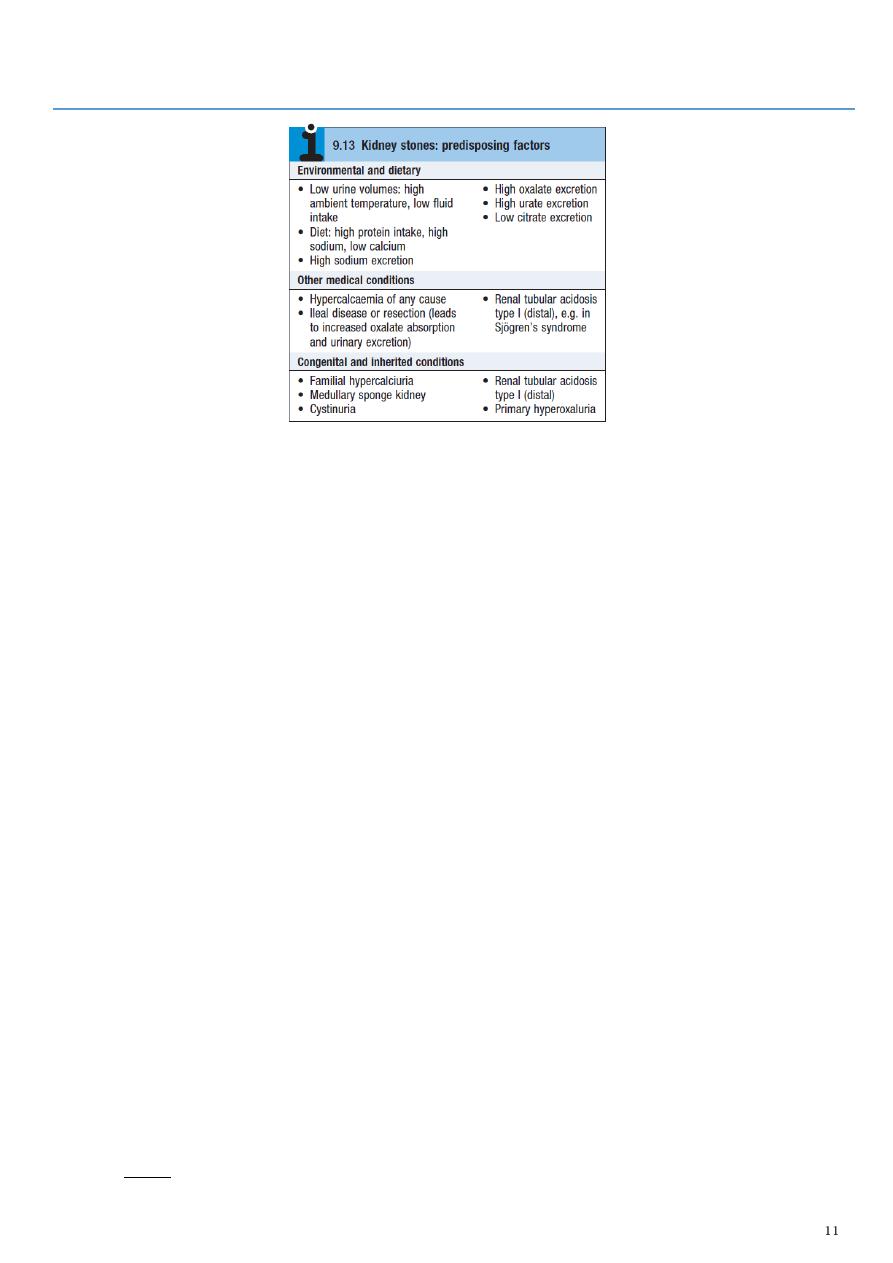
: Urinary stones
Clinical Presentation:
Urinary obstruction ––> distension ––> pain:
o Flank pain from renal capsular distension (non-colicky)
o Severe waxing and waning pain radiating from flank to groin due to stretching of
collecting system or ureter (ureteral colic)
o Never comfortable, always moving.
Nausea, vomiting.
Hematuria, usually microscopic, occasionally gross (90%).
Symptoms of trigonal irritation (frequency, urgency), diaphoresis, tachycardia,
tachypnea.
+/– fever, chills, rigors secondary to pyelonephritis.
Location of Stones:
Calyx:
o May cause flank discomfort, recurrent infection or persistent hematuria.
o May remain asymptomatic for years and not require treatment.
Pelvis:
o Tend to cause UPJ obstruction.
Renal pelvis and one or more calyces:
o Staghorn calculi.
o Often associated with infection.
o Infection will not resolve until stone cleared.
o May obstruct renal drainage.
Ureter:
o < 5 mm diameter will pass spontaneously in 75% of patients.
o Note: the three narrowest passage points for upper tract stones include: UPJ, pelvic
brim, UVJ.
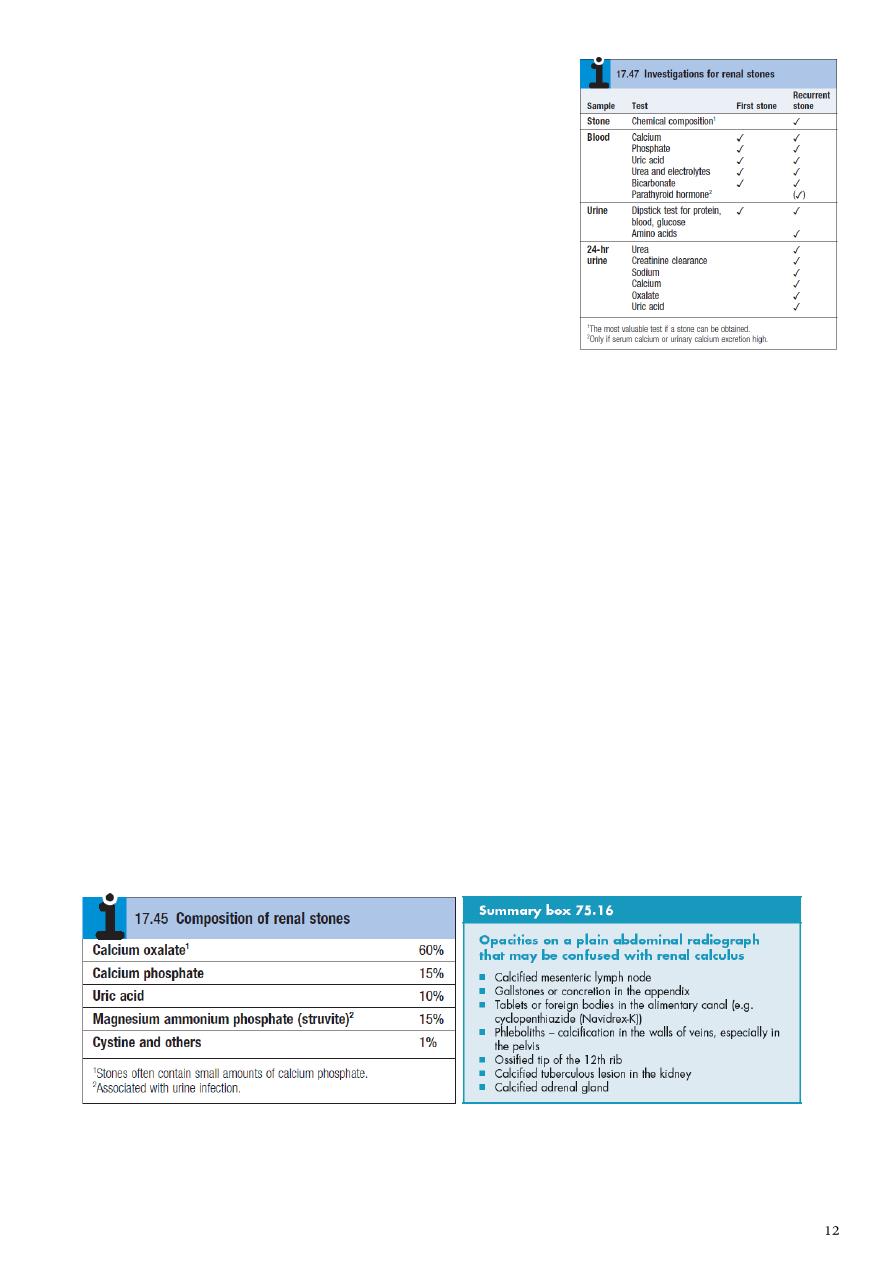
Investigations:
Screening labs:
o CBC ––> elevated WBC in presence of fever
suggests infection.
o Electrolytes, Cr, BUN ––> to assess renal function.
Urinalysis:
o Routine and microscopic (WBCs, RBCs, crystals).
o Culture and sensitivity.
KUB x-ray:
o 90% of stones are radiopaque.
Spiral CT:
o No contrast, good to distinguish radiolucent stone from soft tissue filling defect.
Abdominal ultrasound:
o May demonstrate stone (difficult in ureter).
o May demonstrate hydronephrosis.
IVP:
o Establishes diagnosis.
o Demonstrates anatomy of urine collecting system.
o Degree of obstruction.
o Extravasation if present.
o Renal tubular ectasia (medullary sponge kidney).
o Uric acid stones ––> filling defect.
Metabolic studies for recurrent stone formers:
o Serum lytes, calcium, phosphate and uric acid.
o PTH if hypercalcemic.
o Creatinine and urea.
o 24 hour urine x 2 for creatinine, Ca2+, PO4, uric acid, magnesium, oxalate and
citrate.
Treatment:
1- Medical therapy (expulsive therapy):
Increase fluid intake.
Avoid spicy.
Avoid any thing contain oxalate like coka and caffeine.
Alkalization of the urine (potassium sulfate, sodium sulfate).
Antibiotics.
Alpha blockers (help relaxation of urinary tract and expulsion).
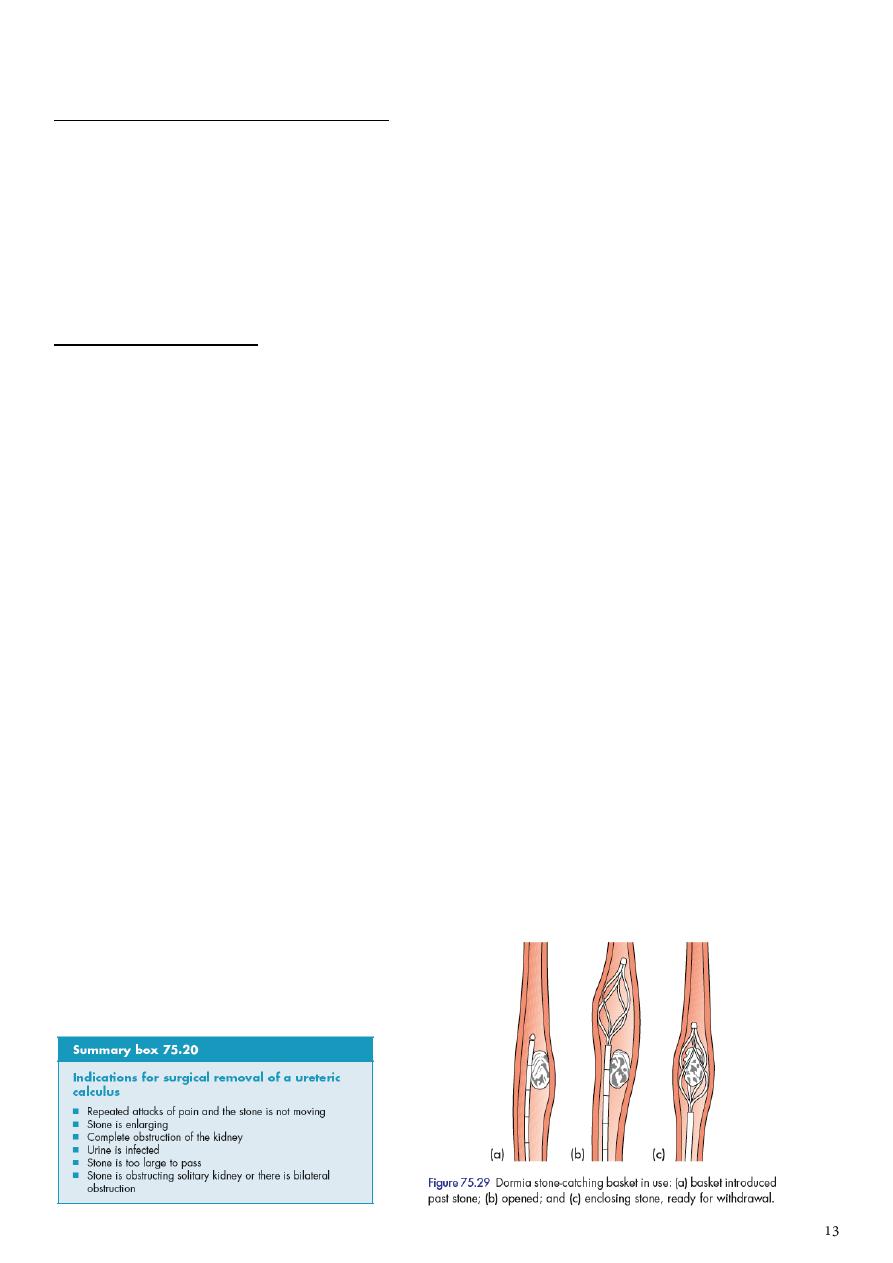
2- Surgical intervention:
Types:
Extracorporeal shockwave lithotripsy (it is ultrasonic waves not laser).
Endoscopy (cystoscopy, ureteroscopy, uretero-renoscopy).
Percutaneous nephrolithotomy (PCNL).
Laparoscopy.
Open surgery.
Contraindications of extracorporeal shockwave lithotripsy:
Pregnancy (the only absolute contraindication but the others are relative).
Bleeding tendency.
Uncontrolled hypertension.
Pacemaker.
Over-weight.
Congenital anomalies of urinary tract.
Too hard or too loose stone.
Distal obstruction like PUJ.
Complications of extracorporeal shockwave lithotripsy:
Perinephric hematoma.
Pain.
Severe hematuria.
Stine strussae (Stone Street).
Bruises.

Part5
: Management of renal colic
History:
1- Pain (acute flank pain):
Colicky pain:
o Last for minutes, increase then decrease to baseline pain level.
o Located in the flank.
o Usually it has radiation according to the site of obstruction (most common cause is
stone).
o Associated with interstitial problems like nausea and vomiting (due to sharing of
celiac plexus, and due to adjacent site to colon and stomach), fever (due to
superadded infection).
o Lead to irritable bladder (frequency, urgency, dysuria, hematuria).
Constant dull pain:
o Due to organic pathology, not due to obstruction.
o Gradual onset of gradual pain.
2- Tachycardia.
3- Dehydration.
4- Fever.
Local examination:
1- Tenderness in costorenal angle (Murphy pinse sign).
2- Genitalia.
3- PR exam.
4- Features of uremia.
Investigations:
1- General urine RBC, pus, bacteria, type and amount of crystals, cast to exclude DDx.
2- Culture and sensitivity pus and bacteria.
3- Renal function test urea and creatinine.
4- CBC WBC count.

5- Imaging study:
Note: render the patient pain free by analgesia before imaging study.
US used for exclude extra-renal problem, site, hydronephrosis, radiolucent stone
(uric acid, xanthine, drug stone).
KUB radio-opaque shadow, soft tissue enlargement.
IVU replaced by US due to time wasting and side effects of contrast.
Treatment:
1- Analgesia (injectable NSAID, morphine).
Note: pain severe not response to analgesia, fever, feature of uremia, bilateral obstruction,
extreme of age, pregnancy use other treatments.
2- Antibiotics.
3- Nephrectomy or renal surgery.
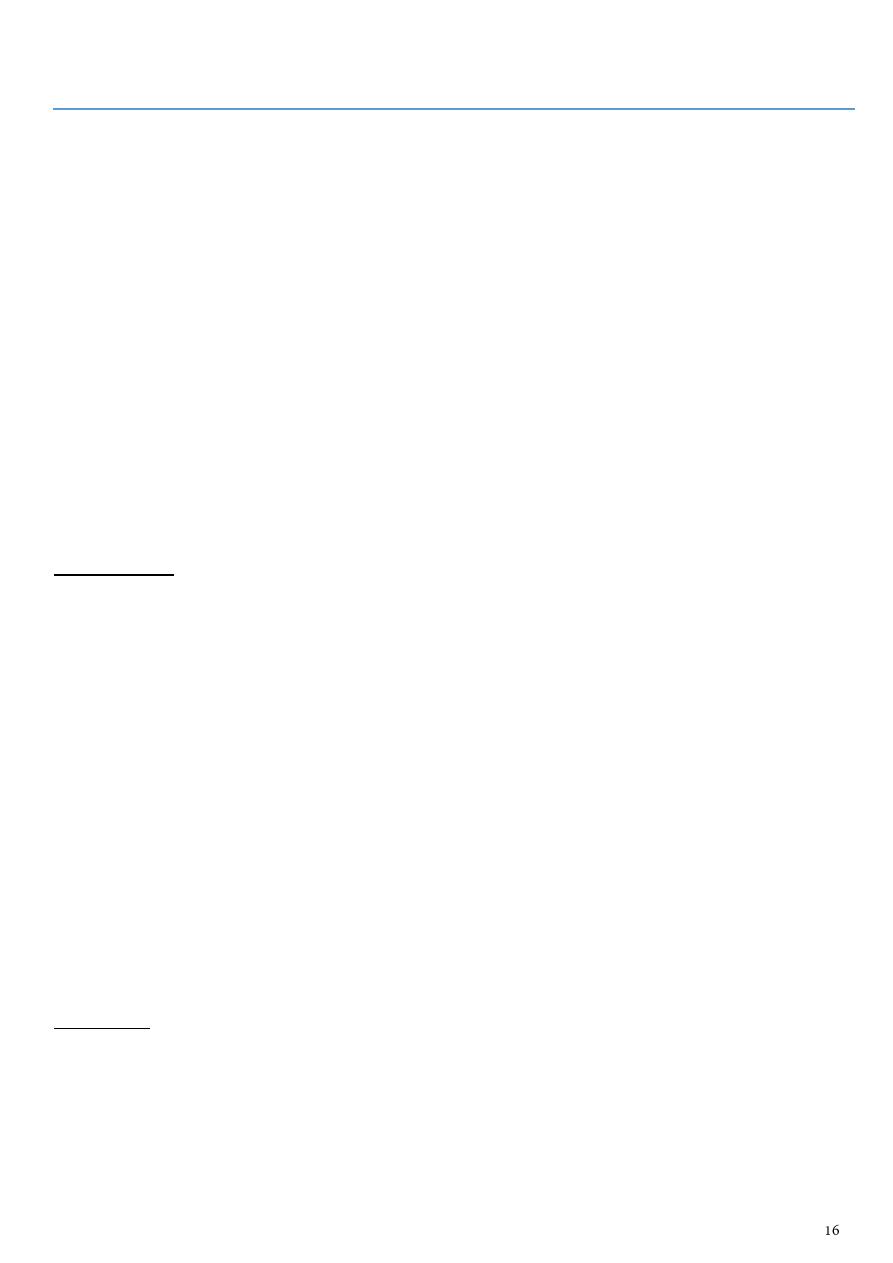
Part6
: Uremia
Symptoms:
Weakness.
Tiredness.
Easily fatigability.
Nausea central cause (waste products in the blood stimulate the vomiting centers,
rise of ICP which called brain edema), local cause (GIT causes like gastric upset and
edema of gut wall).
CNS problems uremic encephalopathy.
Bleeding tendencies hematuria, GIT bleeding, skin bleeding all are due to
platelets dysfunction and affected liver function and fragility of blood vessels.
Sings:
General signs:
Earthy color due to deposition of urea metabolite and due to anemia (pallor).
Bleeding tendency in skin and mucus membrane.
Pallor of the hand.
Brown sign in nails.
Large volume pulse.
Flapping tremor.
Site of dialysis could lead to fistula (in radial artery).
Hypertension (cause and result).
Elevated JVP due to hypervolemia (could be normal if patient in acute failure or
dehydrated).
Central venous catheter in femoral, jugular, cervical veins,
Signs of anemia in the mouth cheilosis, atrophy of papillae.
Eye pallor, jaundice due to liver disease (cause or result or systemic disease).
Bilateral pitting edema.
Local sings:
Abdomen ascites, scar, small size kidney.
Genetalia scrotal edema, hydrocele, examine external urethral meatus.
PR palpate the prostate.
Per-vaginal examination.
Chest examination plural effusion, pericarditis, acute heart failure.
Notes:
Chronic renal failure with large kidney
occur in hydronephrosis, bilateral tumor.
Chronic renal failure with normal size kidney
occur in DM, PKD, multiple myeloma,
amyloidosis, HIV nephropathy, bilateral hydronephrosis.
Investigations:
US.
IVU contraindicated because there is contrast (nephrotoxic).
CT scan axial, coronal, sagittal plane.
Management:
Antihypertensive therapy.
Reduction of proteinuria.
Dietary and lifestyle.
Lipid-lowering therapy.
Treatment of anemia.
Maintaining fluid and electrolyte balance.
Treating renal bone disease.
Renal replacement therapy (by transplantation or dialysis).
Part7
: Urinary injury
Renal injury:
1- Penetrating trauma.
2- Open injury need exploration and combined team surgery.
3- Blunt trauma:
Start with ABC.
Detailed short history of accident is very important (height, kind of object fall on)
History of loss of consciousness is important.
Exposure (check other injuries, see bruises).
90% associated with other organs injury.
Severe trauma lead to renal injury because it is retroperitoneal organ.
Do GUE, CBC, Cross-match, RFT.
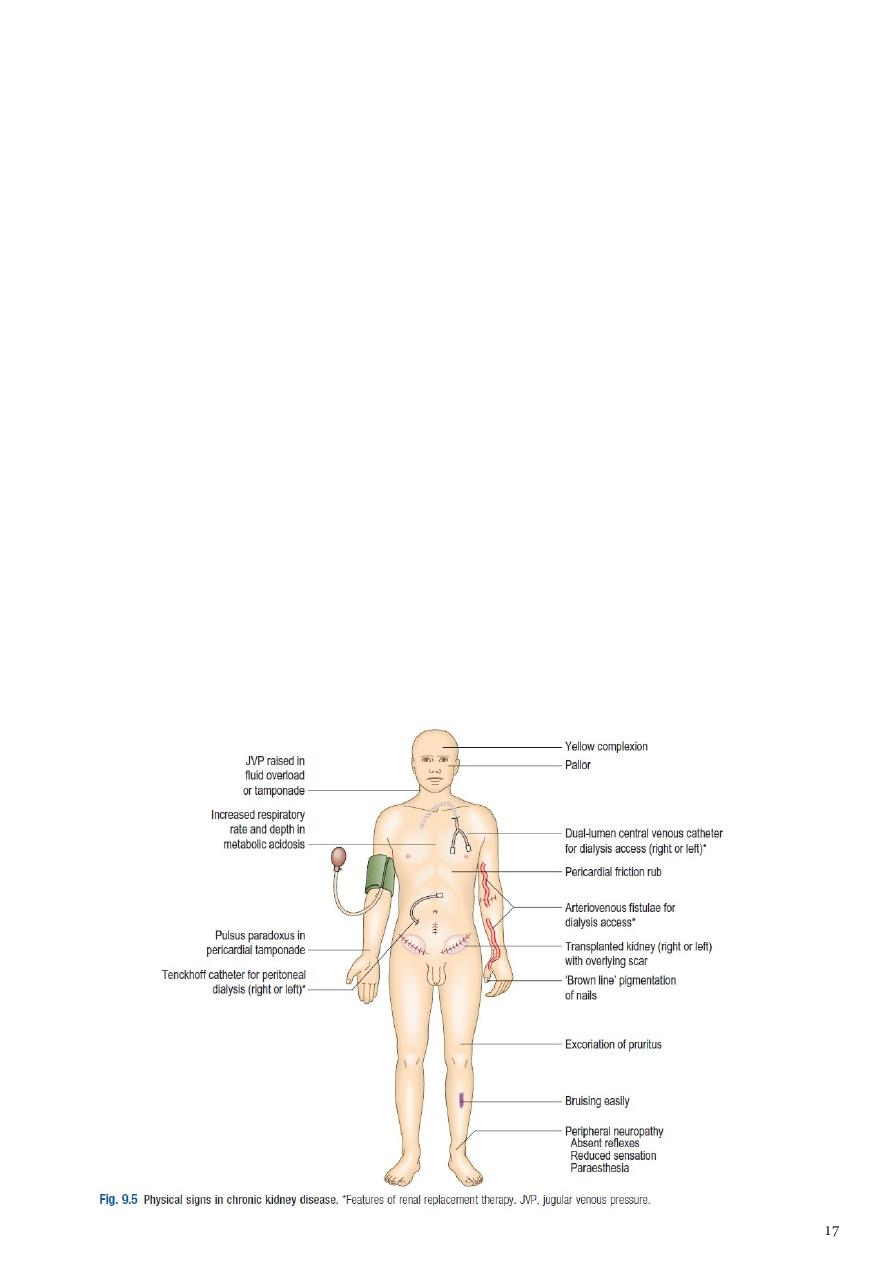
Contrast CT (corner stone investigation) give the stages of renal injury:
Stage1 simple peri-nephric hematoma.
Stage2 less than 1 cm cortical laceration, but
not reach the pelvicalyceal system.
Stage3 more than 1 cm cortical laceration, but
not reach the pelvicalyceal system.
Stage4 reach the pelvicalyceal system, and
there is urinary leak.
Stage5 complete shuttered or avulsed kidney
with avulsed ureter.
Conservative management:
Complete bed rest if there is any movement the paitnet may die, the rest should be
for 24 hours till the urine is clear then we can start simple movement, if hematuria
occur again we make complete rest for other 24 hours.
Antibiotics.
Antiemetic.
Analgesia.
Rehydration.
Folly's catheter.
Save the last urine sample and compare it with other samples to see if the hematuria is
decreased or not.
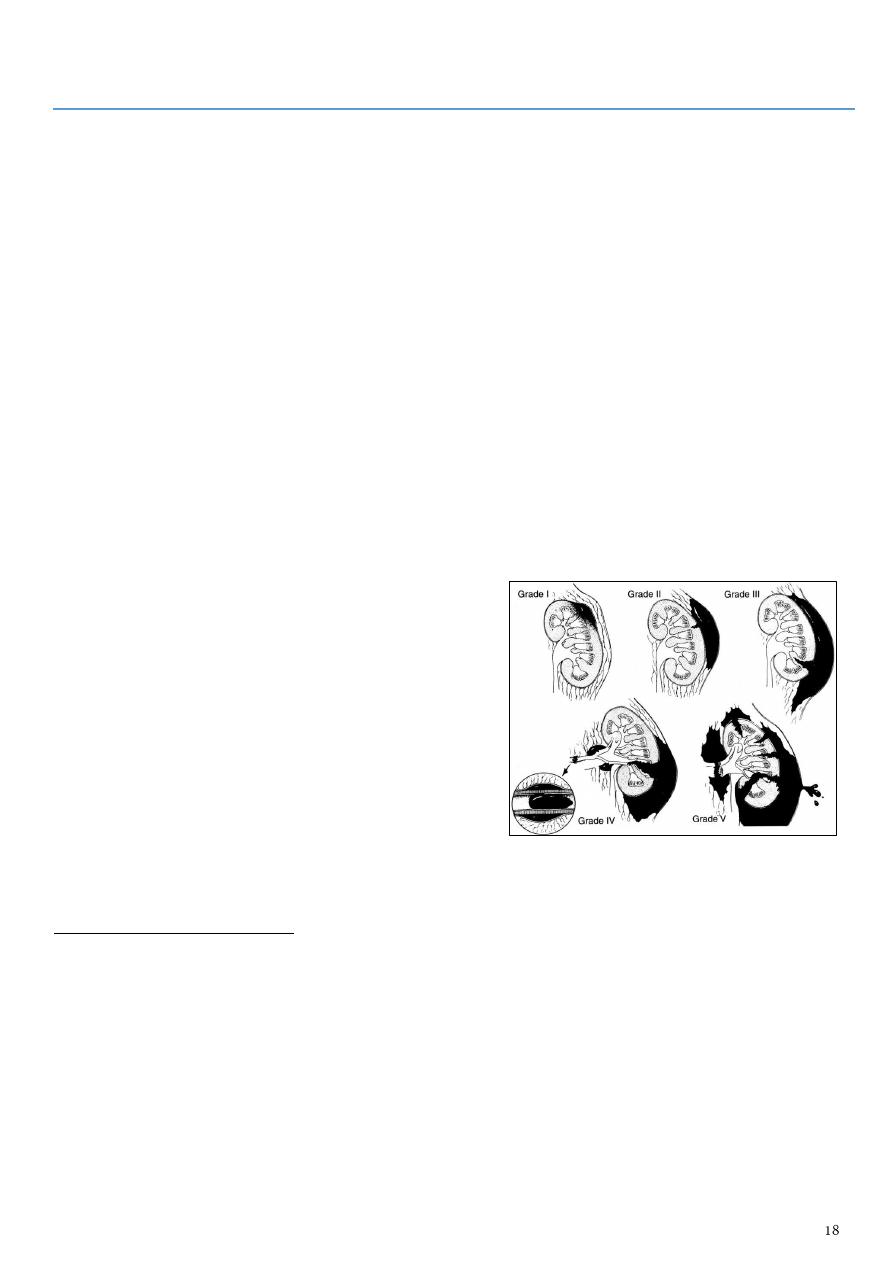
Ureteral injuries:
Causes: Pelvic surgery (uro, gyn, gen.s.), post renal trauma,
penetrating injury, severe blunt trauma, spine fracture.
Features: Flank pain, tenderness, Sepsis, Hydronephrosis,
Paralytic ileus, VV, UV fistula, watery discharge via vagina.
Treatment: nephrostomy, ureteral stenting, reconstructive
surgery.
Bladder injury:
Retroperitoneal injury treated conservatively by folly's catheter.
Intraperitoneal injury rarely in children, especially in open injury or blunt injury for
full bladder, there should be exploration because it lead to peritonitis.
Associated with pelvic injury (85%).
Urethral injury:
Partial or complete.
Contraindicated to put folly's catheter (lead to conversion from partial to complete
injury).
Bleeding per urethra (only blood without urine like hematuria).
Most commonly in males.
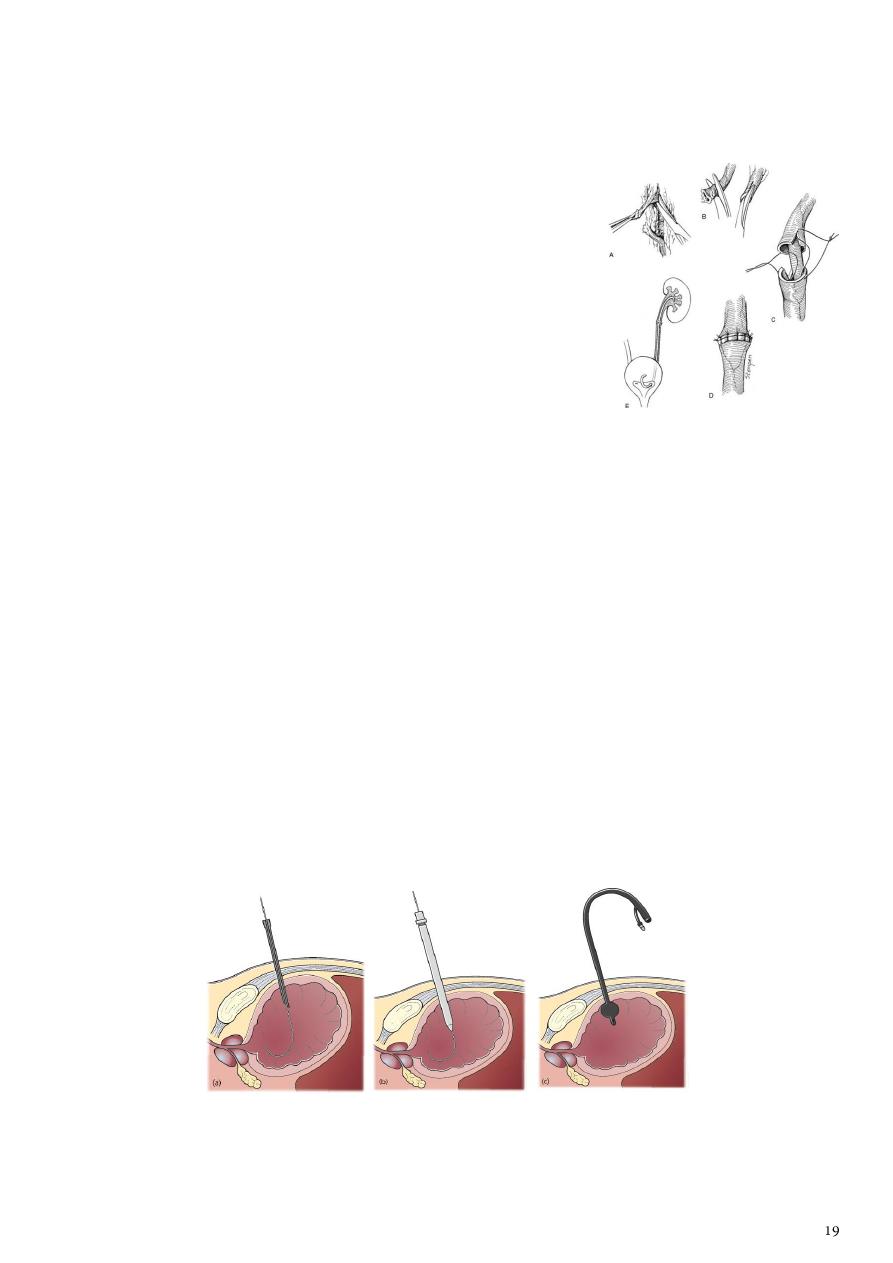
So use suprapubic cystostomy.
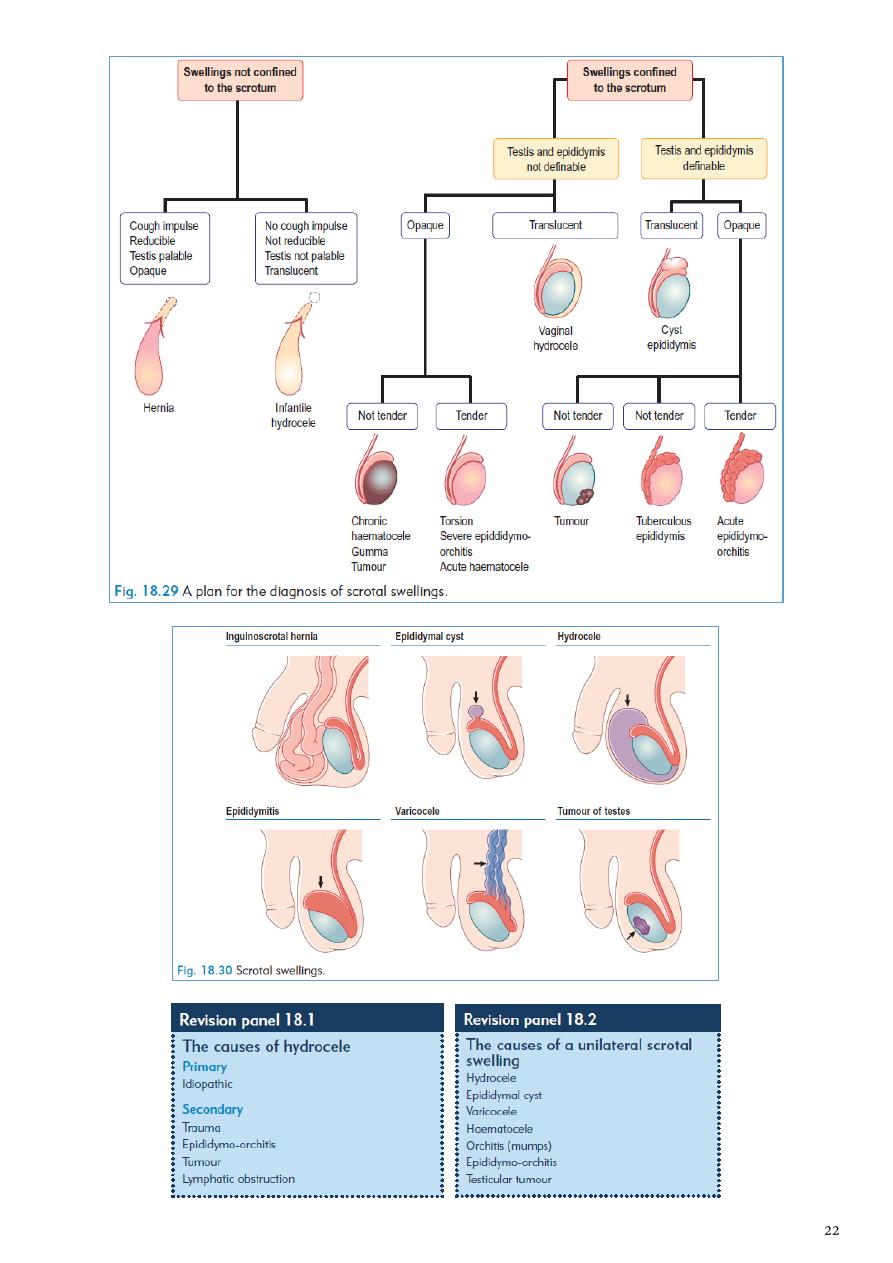
Part8
: Scrotal pathology
Painful scrotal pathologies
(associated with swelling or not)
:
1- Torsion of testes.
2- Epididymo-orchitis.
3- Torsion of the appendix of testes or epididymis.
4- Trauma to the testes.
5- 10% of testicular tumors (if complicated by necrosis or bleeding).
6- Strangulated inguinal hernia.
Torsion to the testes
Epidiymo-orchitis
History:
Sudden pain.
Awake patient from sleep.
Not associated with Constitutional
symptoms.
No Irritative symptoms.
History:
Gradual pain.
Associated with Constitutional
symptoms like fever, rigor, dysuria
because it is due to infection.
Irritative symptoms.
Exam:
Testes lie transversely at the neck or
scrotum.
No signs of inflammation.
Cremasteric reflex is lost.
Elevation of the testes not relieve the
pain (because it is ischemic pain).
Cause secondary hydrocele in late stage.
Exam:
Testes hang down.
There are signs of inflammation on the
scrotal skin.
Cremasteric could be preserved.
Elevation of the testes may relieve the
pain (because it is hanging pain).
Investigations:
GUE normal.
WBC normal.
US (most important investigation).
Doppler US (decreased blood flow).
Investigations:
GUE show UTI.
WBC elevated.
US (most important investigation).
Doppler US (increased blood flow).
Treatment:
Note: always torsion need exploration
due to gangerene (you have 6 hours
only).
Torsion = exploration.
If viable testis = do orcheopexy.
If gangrenous = do orchidectomy.
The other testis should also be fixed because
the anatomical predisposition is bilateral.
In the first hours it may be possible to untwist
the testis manually, then early orcheopexy to
avoid recurrent torsion
Treatment:
Conservative therapy.
Treatment of Epididymo-orchitis:
Admission (but simple one treat at home).
Antibiotics (third generation cephalosporin or quinolones).
Analgesia.
Antipyretic.
Rehydration.
Anti-emetic.
Culture and sensitivity.
Fever decrease in the first day, pain in the 2-3 day, swelling in 6 weeks.
If the culture and sensitivity is show that we give wrong antibiotic but the patient is
going well, we continue the antibiotic because we treat the patient not the paper.
If the culture is show that we give the right antibiotic but the patient become worse, so
we should start from the beginning as we see the patient at the first time and we should
repeat the history and examination and investigation and check for complications
(abscess) and check for the antibiotic (under-dose, expired) then change the type of
antibiotic.
Painless scrotal pathologies
(associated with swelling usually)
:
1- Hydrocele (vaginal hydrocele which is inside tunica vaginalis).
2- Indirect inguinal hernia.
3- Epidedmocele.
4- Spermatocele.
5- Hematocele.
6- Testicular tumor 90%.
Hydrocele
Indirect inguinal hernia
History:
Fixed swelling.
No reducibility.
History:
Could be appear and disappear.
It has reducibility.
Exam:
No reducibility.
Dragging pain.
Cough impulse -ve.
Can get above it (can reach the
spermatic cord).
Transillumination +ve.
Exam:
It has reducibility.
Dragging pain.
Cough impulse +ve.
Cannot get above it.
Transillumination -ve only +ve in rare
cases of early hernia in child.
Investigations:
US clear fluid.
Investigations:
US soft tissue or gases.
Treatment:
Excision.
Treatment:
Herniotomy, hernioplasty, herniorrhaphy.
Part9
: Folly's catheter
Self-retaining catheter, it is drain for bladder.
Classification:
1- According to size:
In French (F) or mm.
French scale = Charrie scale = circumference in mm diameter is size in F (Ch) divided by
( = 3.14) e.g. catheter 18 F has diameter 6 mm
Every 3 F equal to 1 mm.
There are folly's catheter form 6 to 26 F.
Diameter of urethra in adult = 1 cm = 10 mm = 30 F.
2- According to the ways:
One way catheter: for dilatation of urethral stricture, to discover residual urine (better
it is performed by ultrasound), to introduce contrast medium into the bladder.
Two way catheter: self-retaining balloon catheter = Foley catheter.
Three way catheter: for irrigation (lavage) of bladder (by bleeding to bladder after
prostatectomy, due to bladder tumor).
3- According to the substance:
Soft silicon coated latex (silicon is highly resistant to incrustation) , it can be introduced
up to 4 weeks.
100% silicon - it can be introduced up to 8 weeks (it is better, but more expensive).
Indications of folly's catheter:
Diagnostic:
o Cystogram, retrograde urography.
o Monitoring of urinary output in trauma, postoperative, major surgery, severely ill
patient.
o General urine examination (urine sample).
o Measurement of post-void residual urine.
Example: define this tool?
It is self-retaining folly's catheter, 18 F, 3 ways, 100% silicon.

Therapeutic:
o Urine retention.
o Irrigation (it only evacuate the bladder but not stop the bleeding).
o Input/output chart.
o Intravesical chemotherapy.
o Relieve of obstruction.
o After dilatation of urethral stricture.
o After surgery of urethra, bladder, prostate.
o Vesical stone.
o Used as a drain.
Contraindications of folly's catheter:
Absolute suspected urethral injury, acute prostatitis, prostatic abscess.
Relative bleeding tendency, UTI, urethral stricture and history of failure to insert
folly's catheter.
Complications of folly's catheter:
UTI urethritis, cystits, pyelonephritis, fistula, periurethral abscess, epididymo-
orchitis.
Traumatic insertion hematuria, stricture, fistula, premature inflation of folly's
catheter.
Crastational stone formation.
Allergy change the type to latex or silicon.
Failure of deflation of balloon push little amount of normal saline, overiflation of
the balloon, endoscopy, open surgery.
Question of exam: 60 years old patient at day 1 post.op presented with fever and right
hemi-scrotal swelling? epididymo-orchitis due to folly's catheter.
Instruction of usage:
Balloon is filled with distilled water (not air or glucose water).
Totally sterile procedure.
Inflation after checking urine is go out.
Insert it to the shoulder to avoid premature inflation.
In girls: simple insertion (short urethra) / In boys: perpendicular shaft of penis ,hold the
other end of the catheter over your hand (HOLD V BETWEEN YOUR FINGERS OF THE
INSERTION HAND) xylocaine gel, easy pass (not hard) up to end of V, wait until urine
pass put urine cyst, inflation of the balloon (distilled water), pull back to be sure it is in
the wright position.
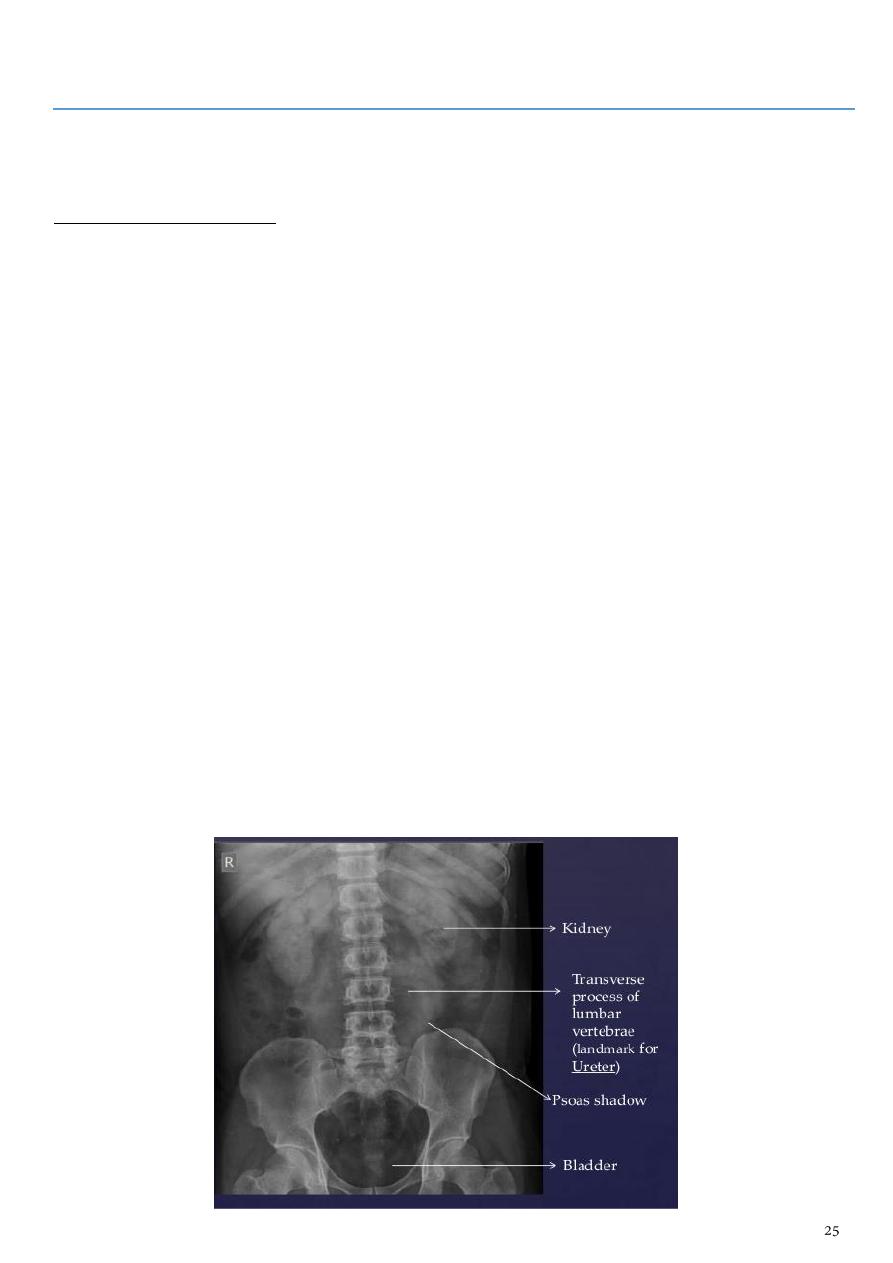
Part10
: Imaging study "KUB"
KUB reading:
Obtain these information:
1- Patient name and age.
2- Sex
by the shape of the pelvis.
3- Site (right or left)
depend on marker or liver shadow and gases in the stomach.
4- Soft tissue
subcutaneous soft tissue, ilio-psoas shadow, renal shadow, abnormal soft
tissue like mass or cyst.
5- Renal area
from lower border of L1 to lower border of L3.
6- Supine or prone position
measure the distance between symphysis pubis and coccyx,
in supine it is 4 fingers long, in prone it is 2 fingers long.
7- Skeleton
e.g. state of the hip bone and the head and neck of femur and the spines.
8- Radio-opaque shadow
DDx: stone, L.N, calcification, rib, gallstone, F.B, fracture of
transverse process.
Urine diversion:
External: e.g. nephrostomy (open or subcutaneous) indicated in post OP. patient and to
prevent hematuria.
Internal: e.g. JJ stent (double J) used to divert urine in patient with obstruction.
Advantages of JJ stent Keep the urinary tract intact, has lower infection rate.
Disadvantages of JJ stent require invasive procedure (scope) to be placed and
removal also require invasive procedure.
Normal KUB
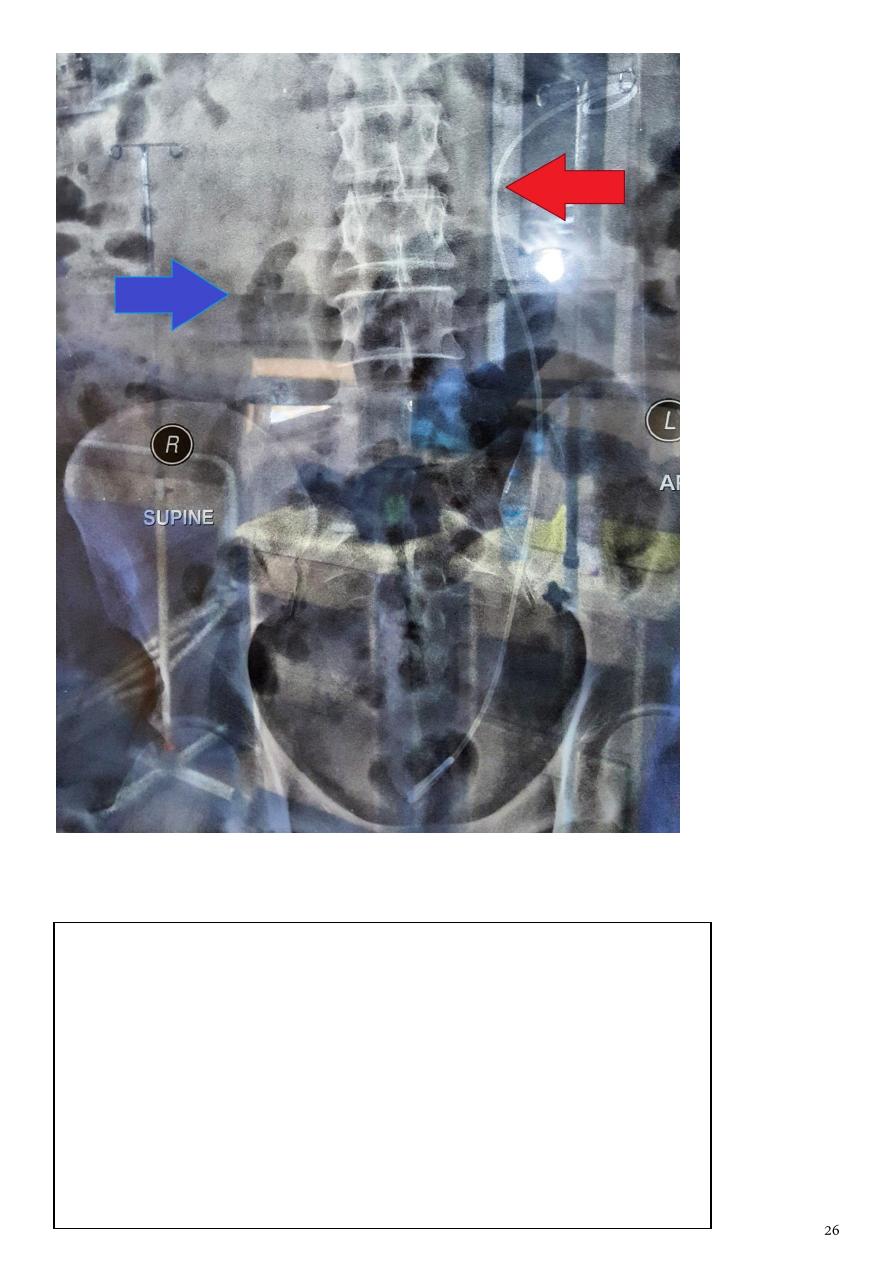
Red arrow: JJ stent
Blue arrow : this Bowl loop
DDx of radiopaque shadow in KUB:
1- Urinary stones (90%). 9- Fecolith in an appendix.
2- Parenchymal calcification in cyst or tumor. 10- Calcified coastal margin.
3- Nephrocalcinosis. 11- Chip fracture of transverse process.
4- TB of the kidney. 12- Calcified uterine fibroid.
5- Supra-renal calcification. 13- Calcification within ovary.
6- Phlebolith. 14- Prostatic calcifications.
7- Gall stone. 15- Aortic calcifications.
8- Calcified L.N. 16- Pancreatic calcifications.
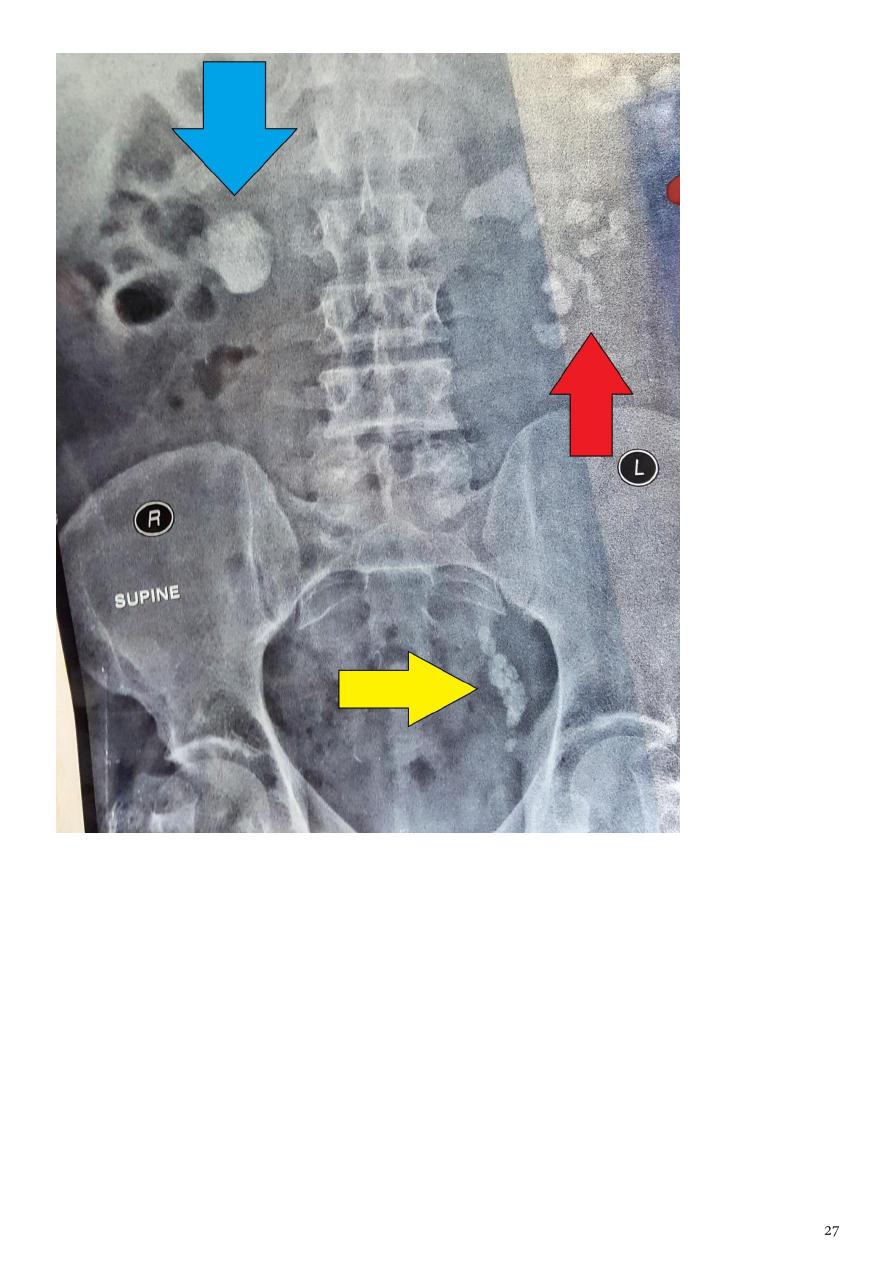
Blue arrow : Single large about 3-5 CM rounded radio-opaque shadowing in
the right renal area . ( large stone )
Red arrow : multiple small radio-opaque shadows in the left kidney area . (
multiple stone )
Yellow arrow : multiple small radio-opaque shadowing along the course of
lower ureter ( multiple lower ureteric stone )
Note: there is OA changes in the head of hummers, L4,L5.
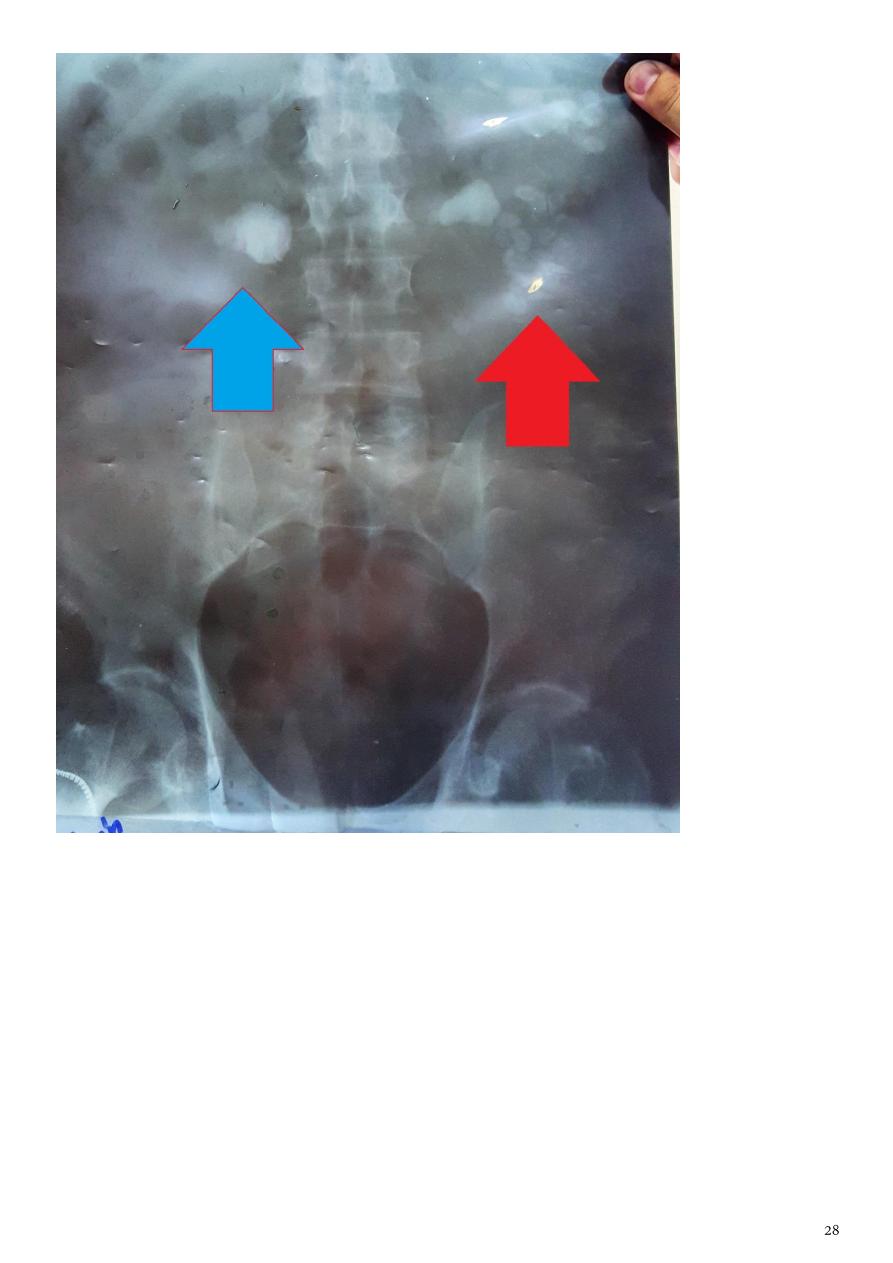
Red arrow : multiple small radio-opaque shadows in the left kidney area . (
multiple stone )
Blue arrow : Single large about 3-5 CM rounded radio-opaque shadowing in
the right renal area . ( large stone )

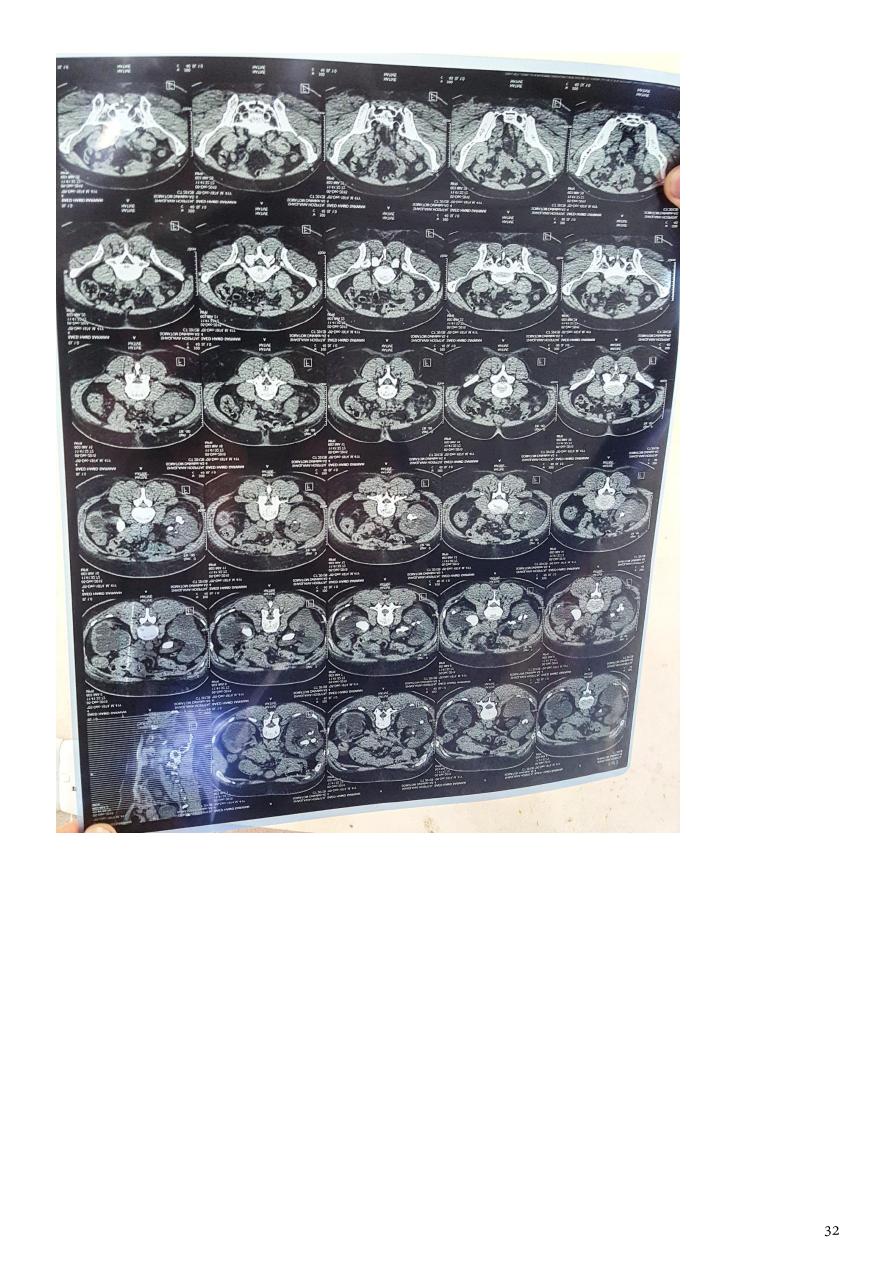
Coronal plane CT of the Abdomen .
Red arrow : multiple hyperdense area in the left kidney. ( multiple stone )
Blue arrow : Single large rounded hyperdense area in the right kidney . ( large
stone )
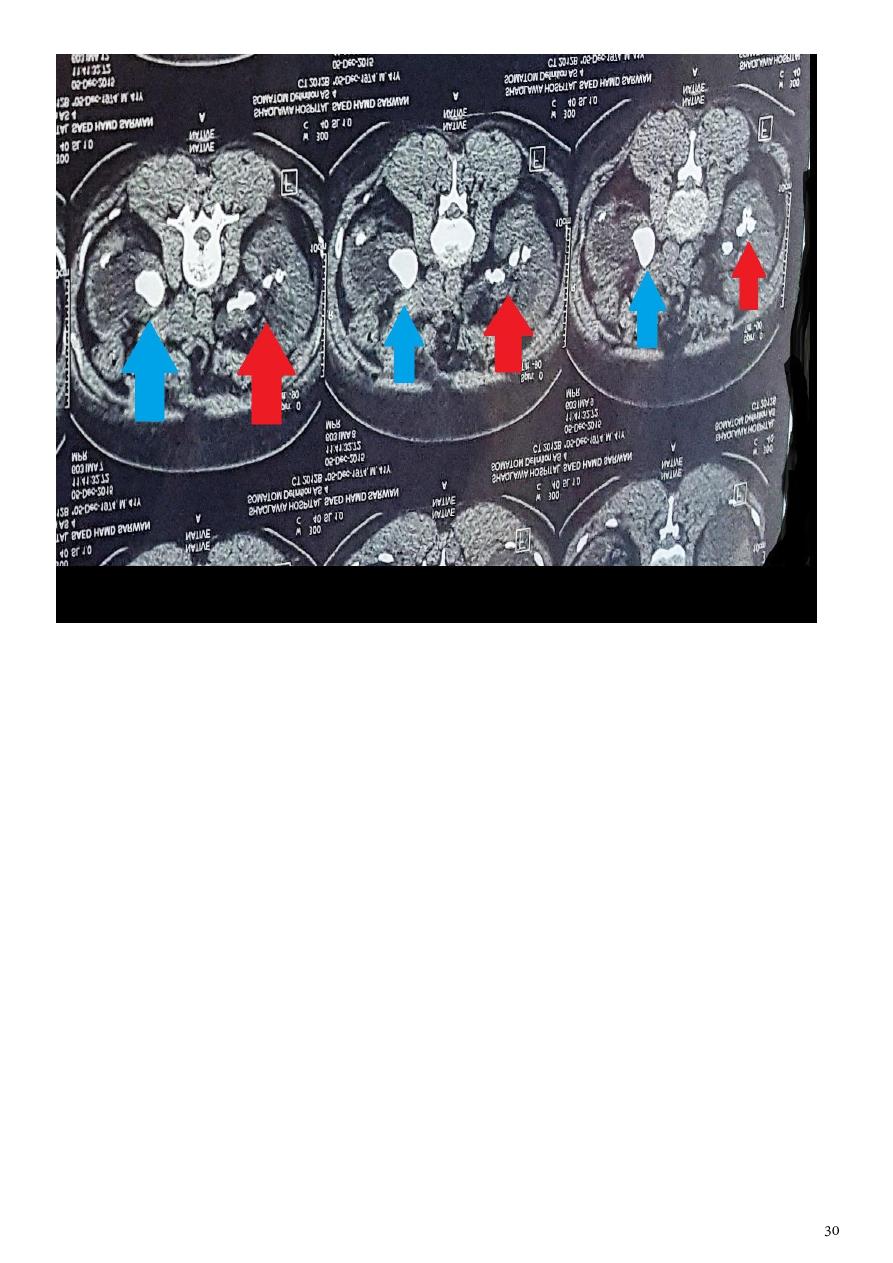
Axial plane CT of the Abdomen .
Red arrow : multiple hyperdense area in the left kidney. ( multiple stone )
Blue arrow : Single large rounded hyperdense area in the right kidney . ( large
stone )
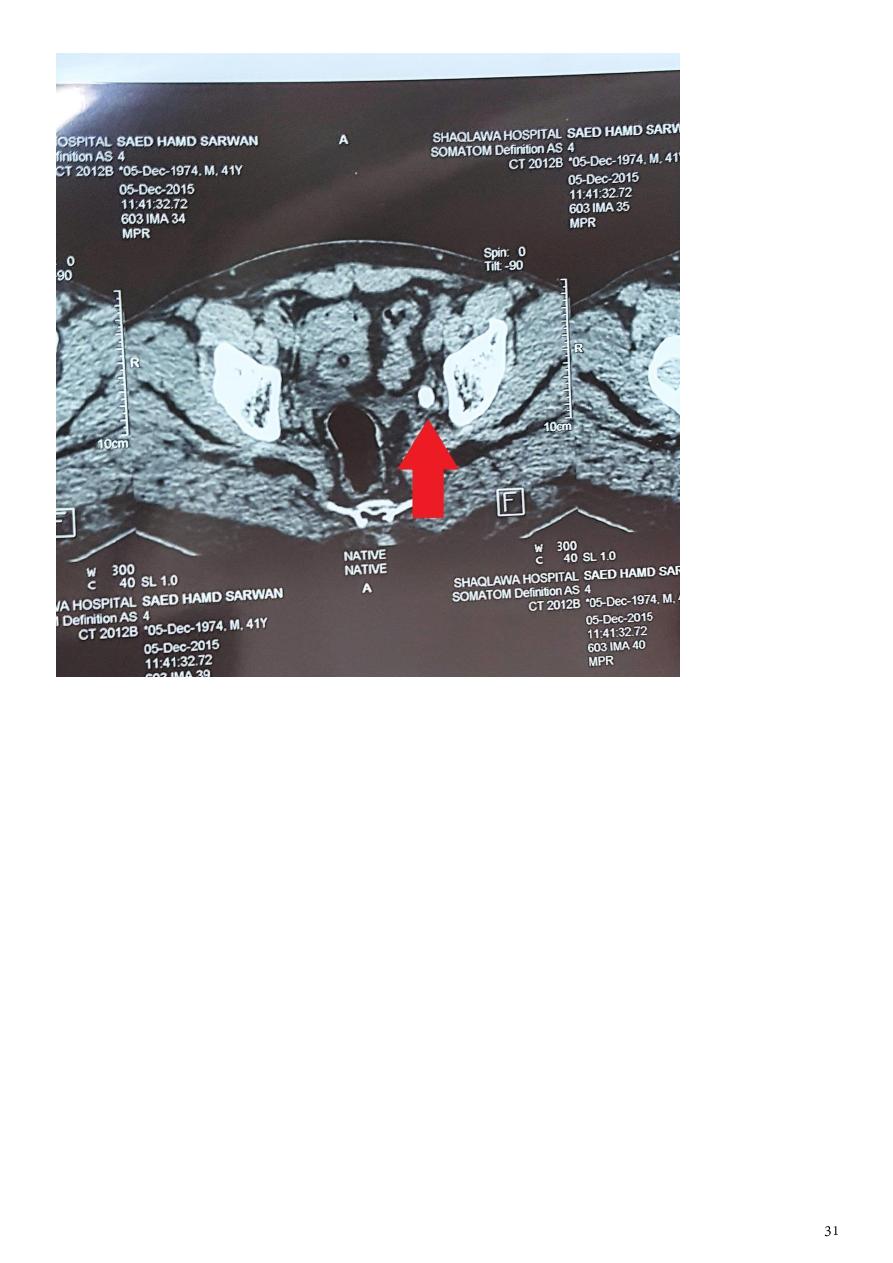
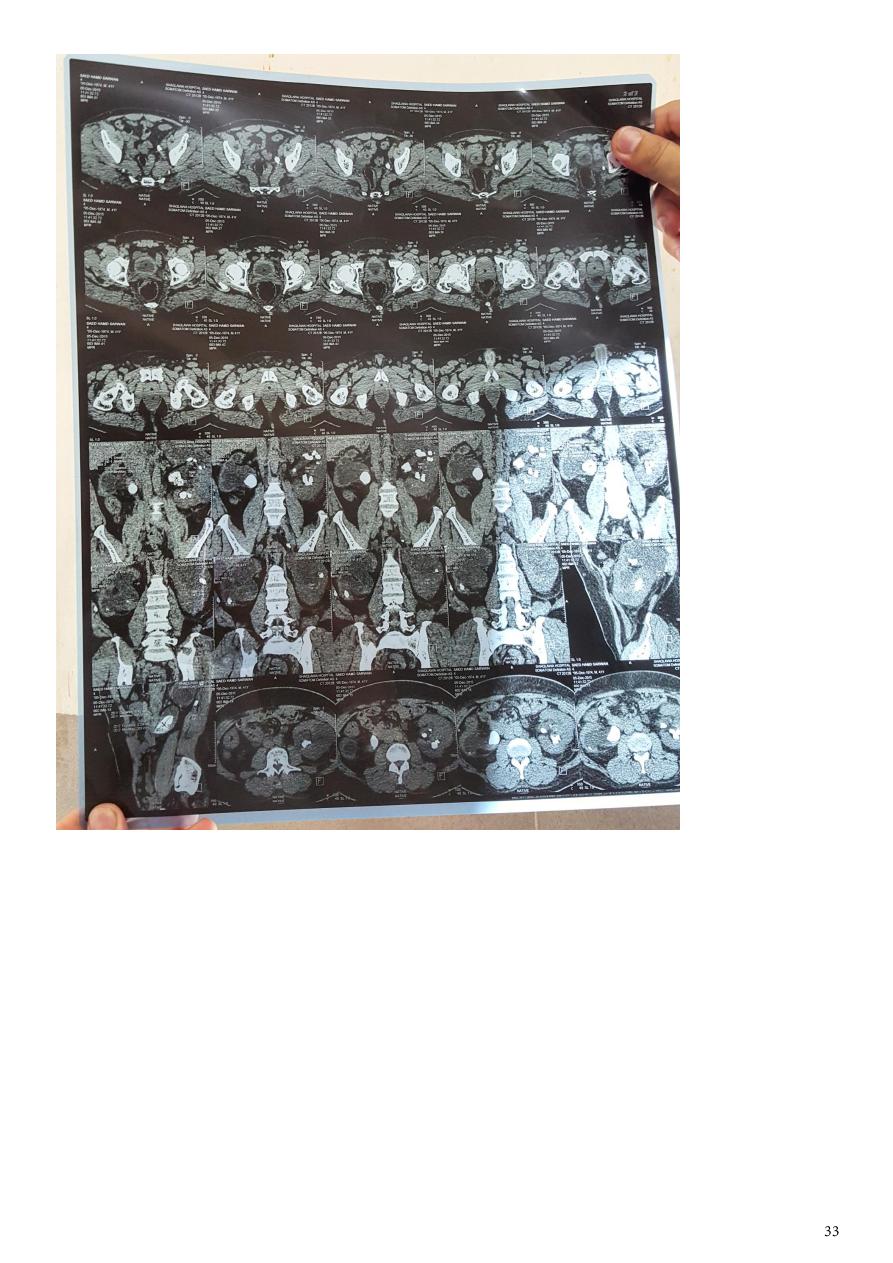
Axial plane CT of the lower abdomen :
Red arrow : Lower ureteric stone
Part11
: Extra
Causes:
Investigations:
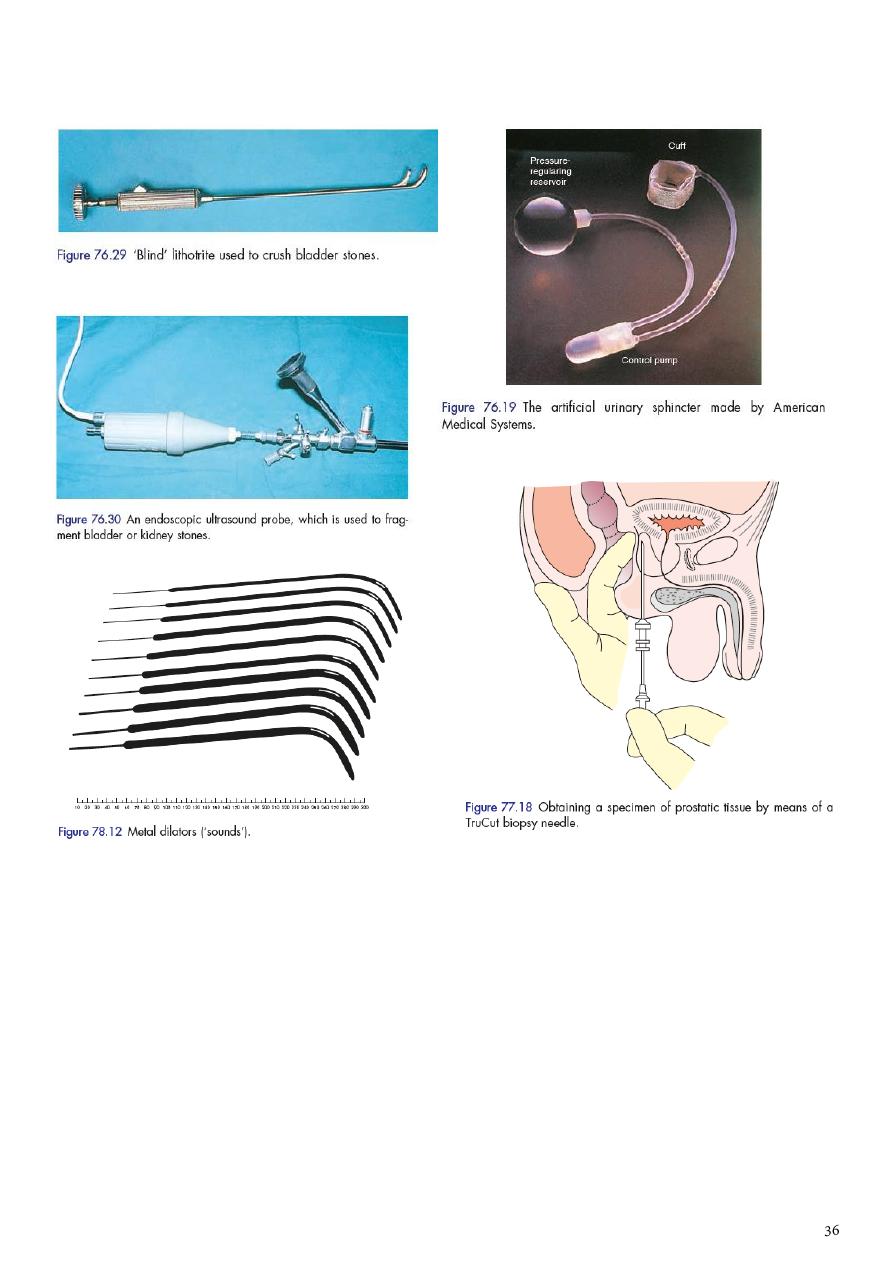
Instruments:
Notes:
Patients are at high risk for IVU contrast:
IDDM with renal insufficiency.
Renal insufficiency.
Dehydration.
Past medical history of contrast allergy.
Allergic diseases (hay fever, asthma, dermatitis, food allergy).
Congestive heart failure.
Multiple myeloma.
Failure of visualization of kidney on IVU could be:
Agenesis.
Dysplastic kidney.
Ectopic kidney.
Nephrectomy.
Grossly dilated kidney.
Obstructed kidney (congenital or acquired).
Renal pedicle injuries.
Indications of orchidectomy:
Tumor (radical).
Trauma (simple).
Torsion.
TB.
Severe epididymo-orchitis (pus collection).
Undescended testis in above 10 years aged patient.
Advanced CAP (bilateral sub capsular orchidectomy).
Indications of nephrectomy:
Tumor (radical).
Trauma (simple).
Large stone burden with destructive effect.
Severe infection as in pyonephrosis or perinephric abscess.
Chronic pyelonephritis kidney.
TB nephritis.
Advanced hydronephrotic kidney.
Congenitally abnormal kidney (hypoplastic or dysplastic kidney).
Indications of nephron-ureteroctomy:
Cancer (TCC).
TB nephron-uretritis.
Advanced case of reflux (grade5).
Indications of partial nephrectomy:
Duplex system with destructive changes in either moiety.
Tumor in single kidney.
Trauma.
Segmental hydronephrosis.
Multiple stones in lower pole.
Indications of cystostomy:
Retention of urine.
BOO.
Impossible stricture.
Post open prostatectomy.
Performing antegrade contrast study.
Infant with severe form of posterior urethral valve (temporarity vesicostomy).