1
Ophthalmology
History taking:
Include:
Personal data.
Chief compliant.
History of present illness.
Previous ophthalmological history.
Previous medical and surgical history.
Drug history.
Loss of vision:
1- Gradual painless LOV:
Cataract.
Open angle glaucoma.
Diabetic retinopathy.
Tumor.
2- Sudden painless LOV:
Retinal detachment.
Optic neuritis.
Retinal venous occlusion.
Retinal arterial occlusion.
Vitrous hemorrhage.
Sudden discovery of preexisting unilat pinguecula.
3- Painful LOV:
Uveitis.
Iritis.
Close angle glaucoma.
Keratitis.
Trauma.
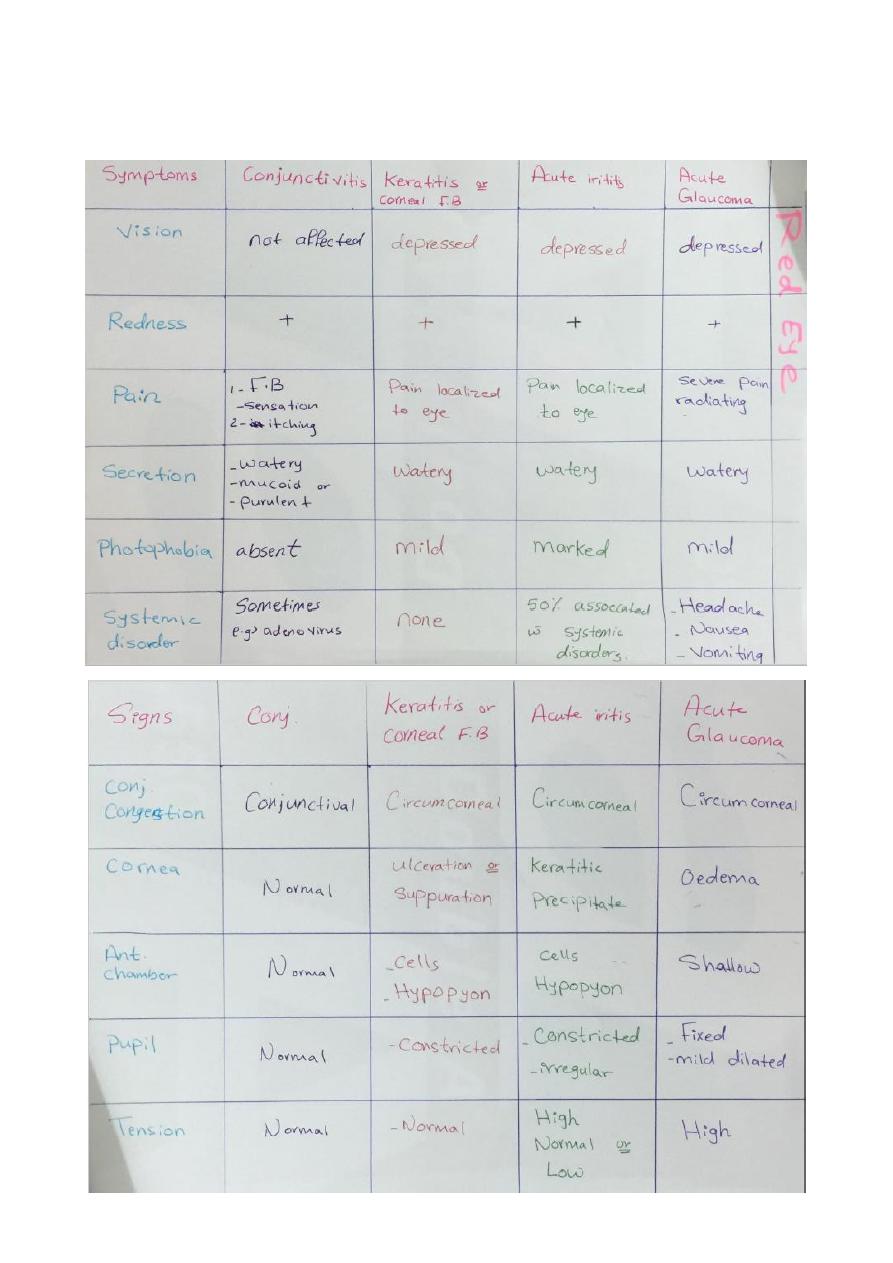
Red eye:
Conjunctivitis.

2
Keratitis.
Iritis.
Closed angle glaucoma.
Scleritis and epi-scleritis.
Blepharitis.
Allergy.
Trauma.
Side effects of corticosteroids eye drop:
Flare up of pre-existing eye infection.
Predispose for microbial keratitis (viral, bacterial, fungal).
Inhibit collagen synthesis of cornea and predispose to corneal thinning.
Cataract (chronic case).
Open angle glaucoma (chronic case).
Indications of topical steroid in eye disease:
Decrease inflammatory reaction in post ocular surgery (cataract operation).
Inflammatory noninfectious disorders (iritis).
Hypersensitivity to microbial antigens phlyctenular keratoconjunctivitis (under
cover of topical antibiotics) Disciform keratitis (under cover of antiviral).
Sometimes in non-severe microbial keratitis involving the axial part of the cornea to
decrease scaring under the follow precaution:
o Identify causative agent by lab investigations and giving appropriate antibiotic.
o There is clinical response or treatment.
o There is no thinning or impending perforation of cornea.
o Contraindicated in pseudomonas, fungal, epithelial viral keratitis.
o Patient must not immune compromised.
o Close follow up (in hospital).
Contraindications of steroids:
Active bacterial keratitis.
Pseudomonas, fungal, epithelial viral keratitis.
Immune compromised patient (D.M).
Thinning or impending perforation of cornea.
When we don’t know causative agent of disease.
3
Severely infected and complicated eye disease that need management with antibiotics
and follow up.
No clinical response on treatment.
4
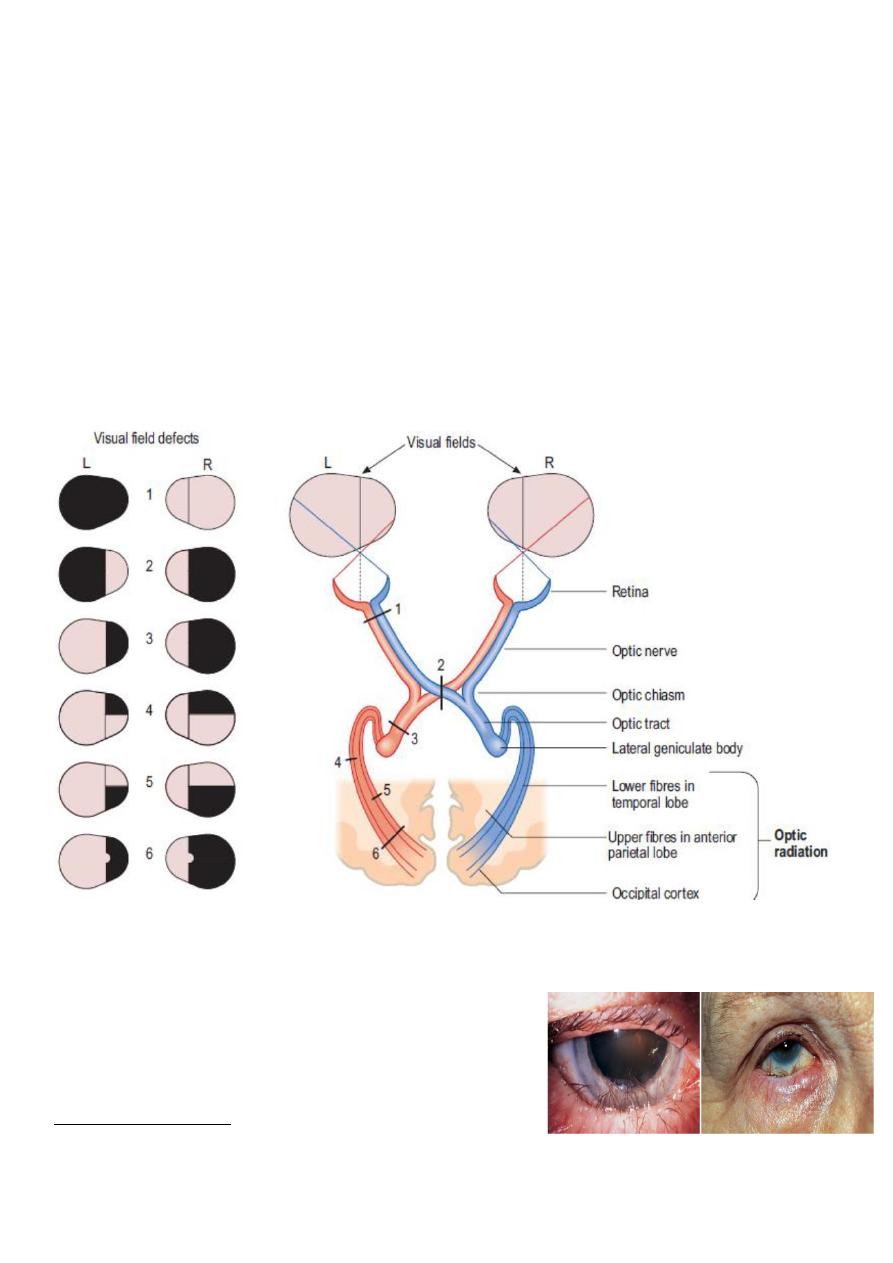
Effects of lesions in optic pathway on visual fields:
1- Blindness of the left eye.
2- Biltemporal hemianopia.
3- Right homonumus hemianopia.
4- Right upper quadrantic hemianopia due to lesion of lower fibers of optic radiation in the
temporal lobe.
5- Lower right quadrantic hemianopia due to lesion of the upper fibers of optic radiation in
the upper anterior parietal lobe.
6- Right homonymus hemianopia lesion in optic radiations in the posterior parietal lobe
here the light reflex is present.
Entropion:
Malposition (inward turning) of eyelid toward the
eyeball with trichiasis (misdirection of the eyelashes
toward the eyeball).
Causes of entropion:
1) Congenital (rare).
2) Acute spastic conditions such as infections, inflammatory & traumatic.
3) Cicatricial (scaring of the palpebral conjunctiva).
5
Causes of trichiasis:
1) Infections (trachoma, herpes).
2) Auto-immune (ocular cicatricial pemphigoid).
3) Inflammatory (Stevens-Johnson syndrome, vernal keratoconjunctivitis).
4) Trauma.
Complications (entropion & trichiasis):
1) Infections.
2) Corneal ulceration, corneal opacity.
3) Chronic conjunctivitis, conjunctival scar.
Treatment of entropion:
1) Eyelid hygiene.
2) Antibiotics to treat the causative microorganism.
3) Steroids.
4) Lubrication.
5) Small amount of botulinum toxin (BOTOX).
6) Surgical repair (Lateral canthotomy, lateral canthoplasty).
Treatment of trichiasis:
1) Treatment of the underlying disease (Stevens-Johnson syndrome & ocular cicatritial
pemphigoid).
2) Lubrication.
3) Treatment of infection.
4) Surgery (follicle destroying or lash/follicle repositioning).
Ectropion:
Abnormal eversion (outward turning) of the lower
eyelid margin away from the globe.
Patient complaint: Lacrimation.
Causes:
1) Congenital.
2) Acquired:
a) Senile.
b) Paralytic (facial nerve palsy).
c) Cicatricial (due to scar) such as burns, glaucoma drops and chronic dermatitis ….etc.
d) Mechanical (tumor) such as neurofibromas.
Complications:
1) Conjunctival keratinization.
2) Corneal breakdown (ulceration)
3) Epiphoria (watery eye: tears flow onto the cheek).
4) Pain.
Treatment:
1) Treatment of infection (Chlamydia, herpes).
2) Lubrication.
3) Steroid.
4) Surgical repair (V to Y plasty or Z plasty).
6
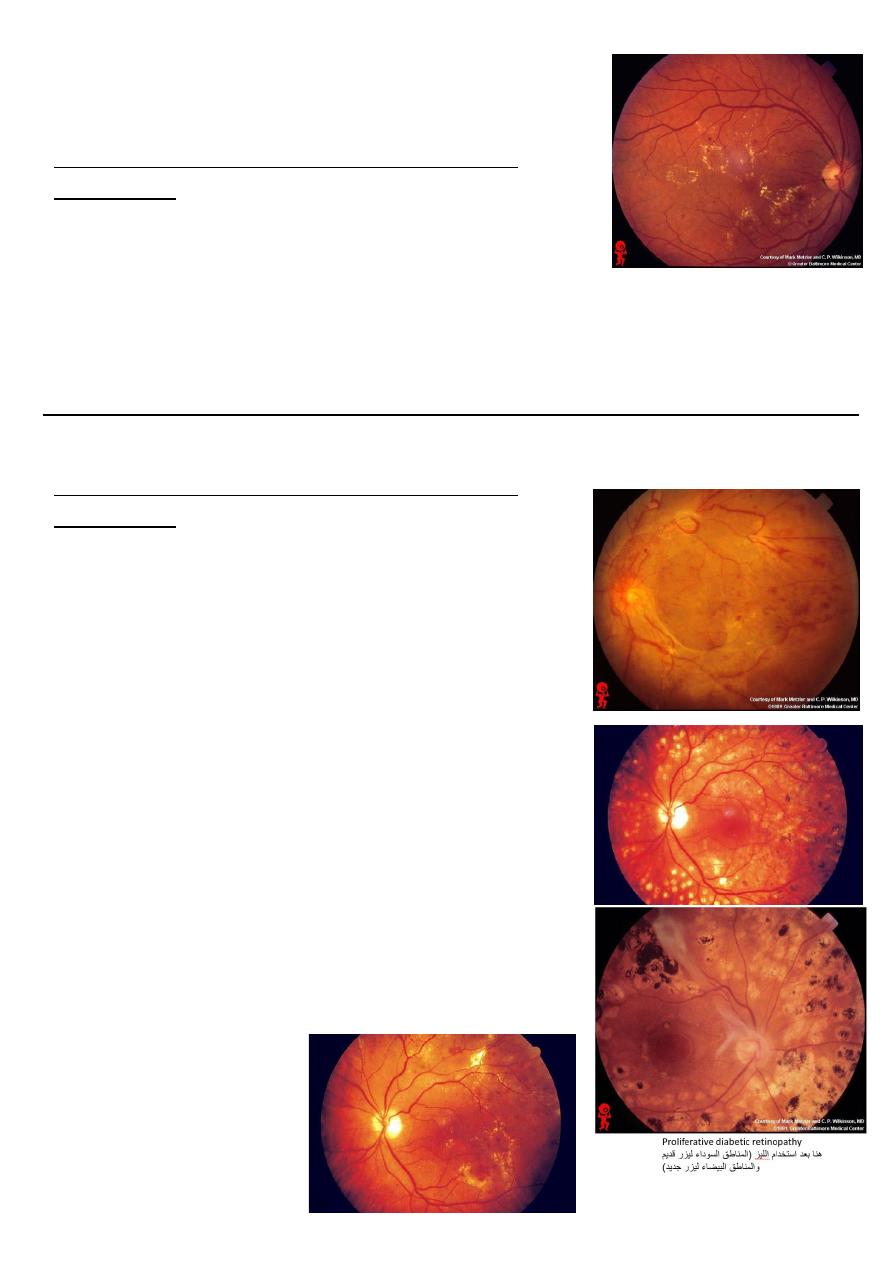
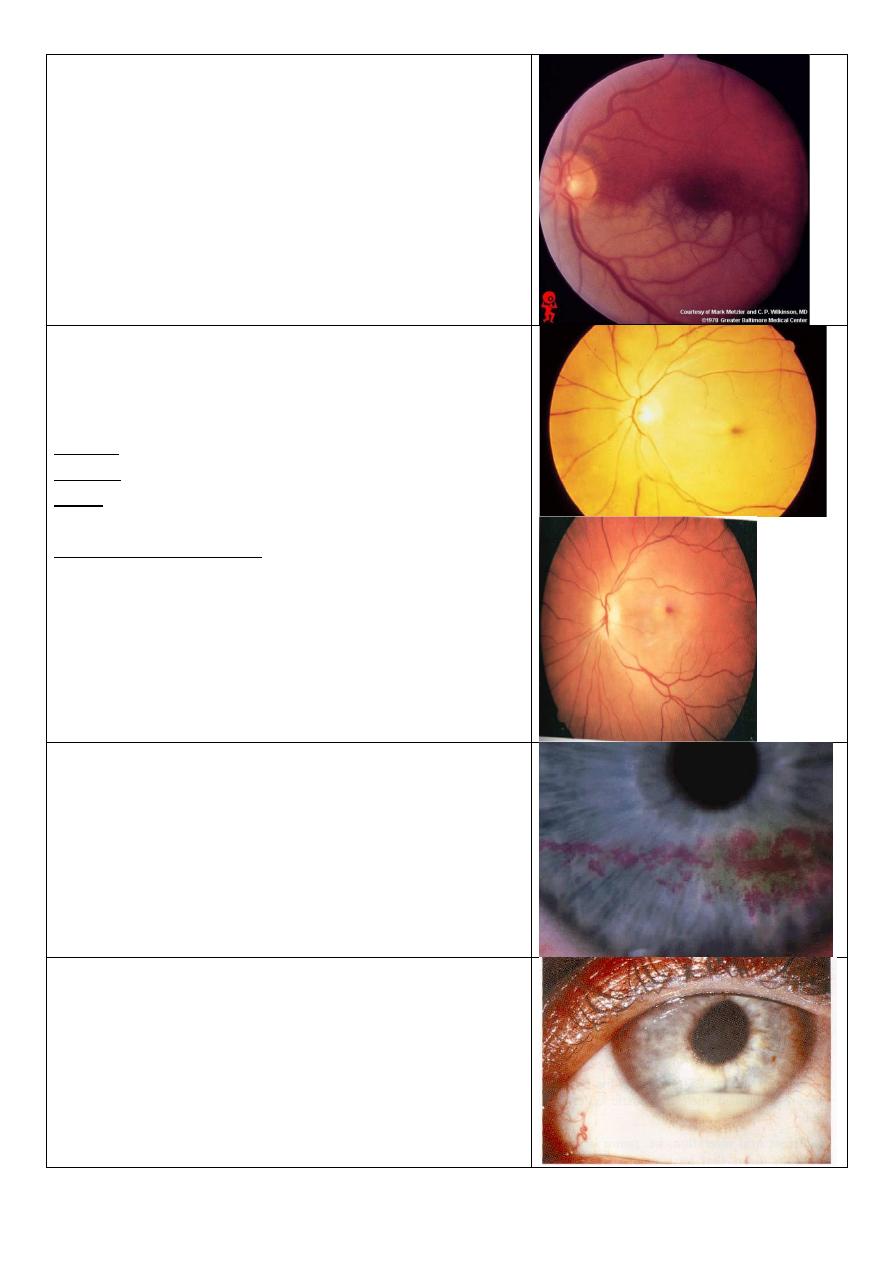
Diabetic retinopathy:
The problem is in the vessels.
First type leakage (non-proliferative diabetic
retinopathy)
Loose pericyte of vessels wall.
Features:
o Hemorrhage red dots.
o Transudate (edema) change in color.
o Exudate (lipoprotein) golden yellow lesion.
o Aneurysm red dots near blood vessels.
Site of leakage: close it by laser.
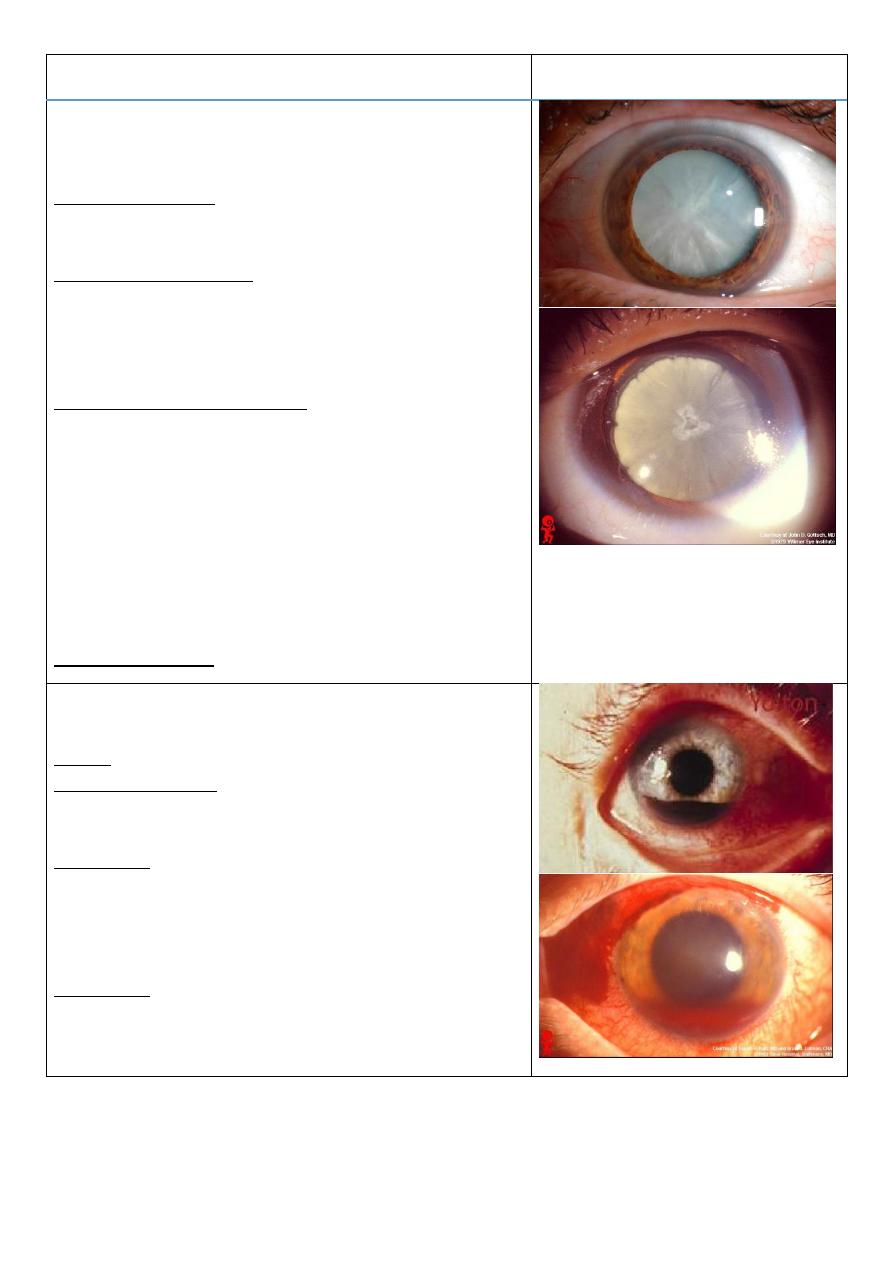
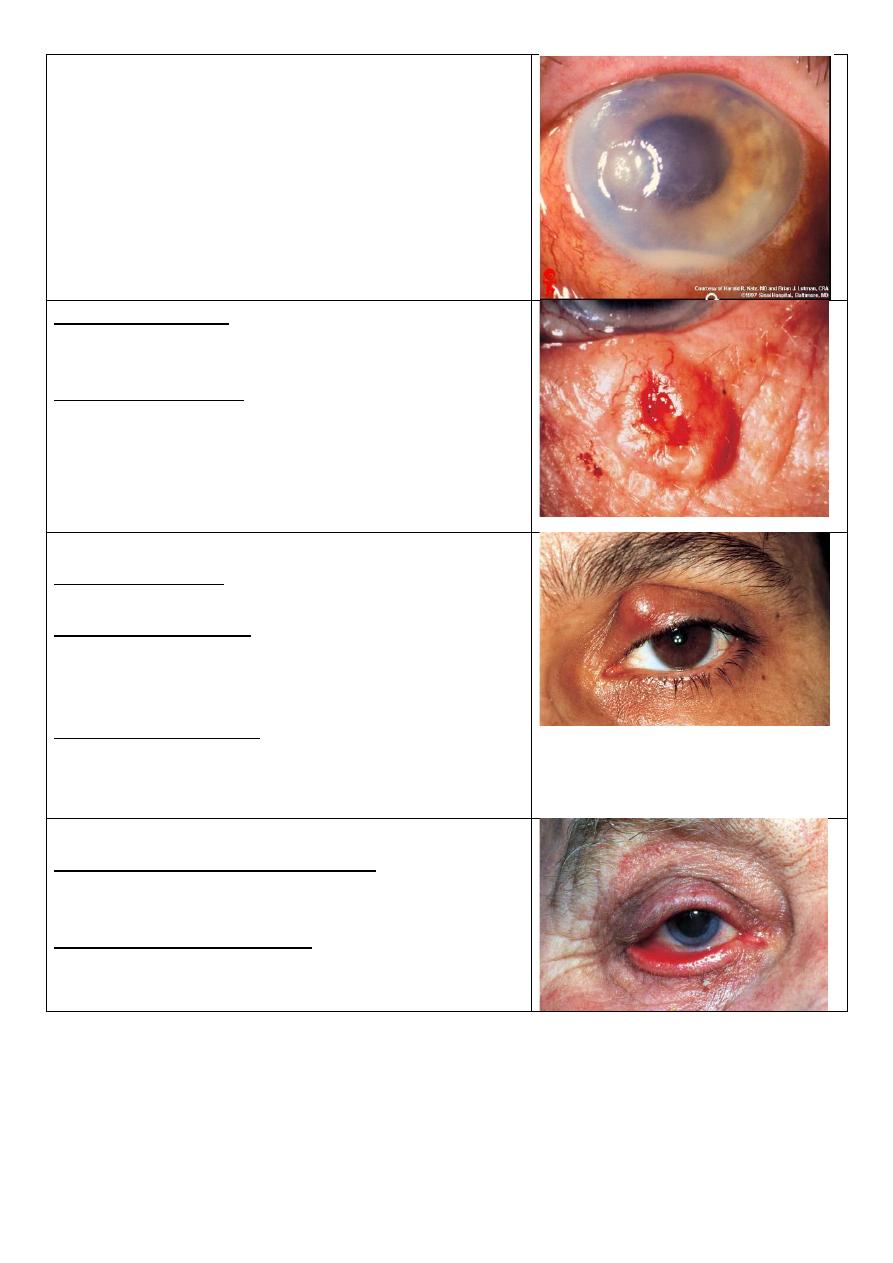
Second type occlusion (proliferative diabetic
retinopathy)
Because viscosity of blood increase and platelets
aggregation increase and vessels wall thick due to
hyperplasia of tunica media and RBC stick with each
other called roloux formation lead to ischemia in the
periphery.
Vascular endothelial growth factor:
o Produce new blood vessels that is fragile and lead to
hemorrhage.
o Produce fibrosis could lead to retinal detachment.
Features:
o Ischemia.
o Fibrosis.
o New vessels.
o Localized area of ischemia called cotton wall spots.
Site of ischemia: photocoagulation, this destroy new
vessels but the fibrosis not destroyed, and this
procedure not lead to any problem to the patient.
7
Description
Photo
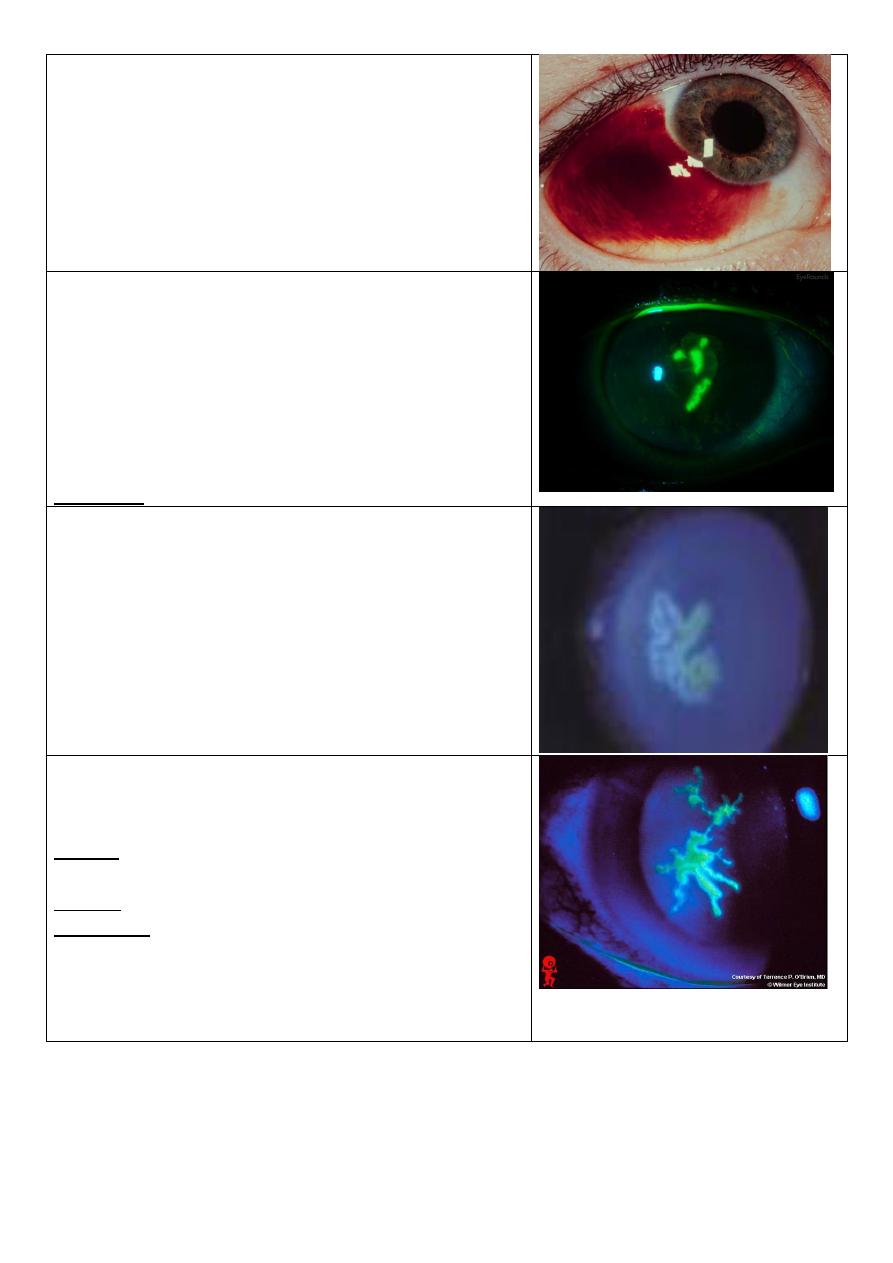
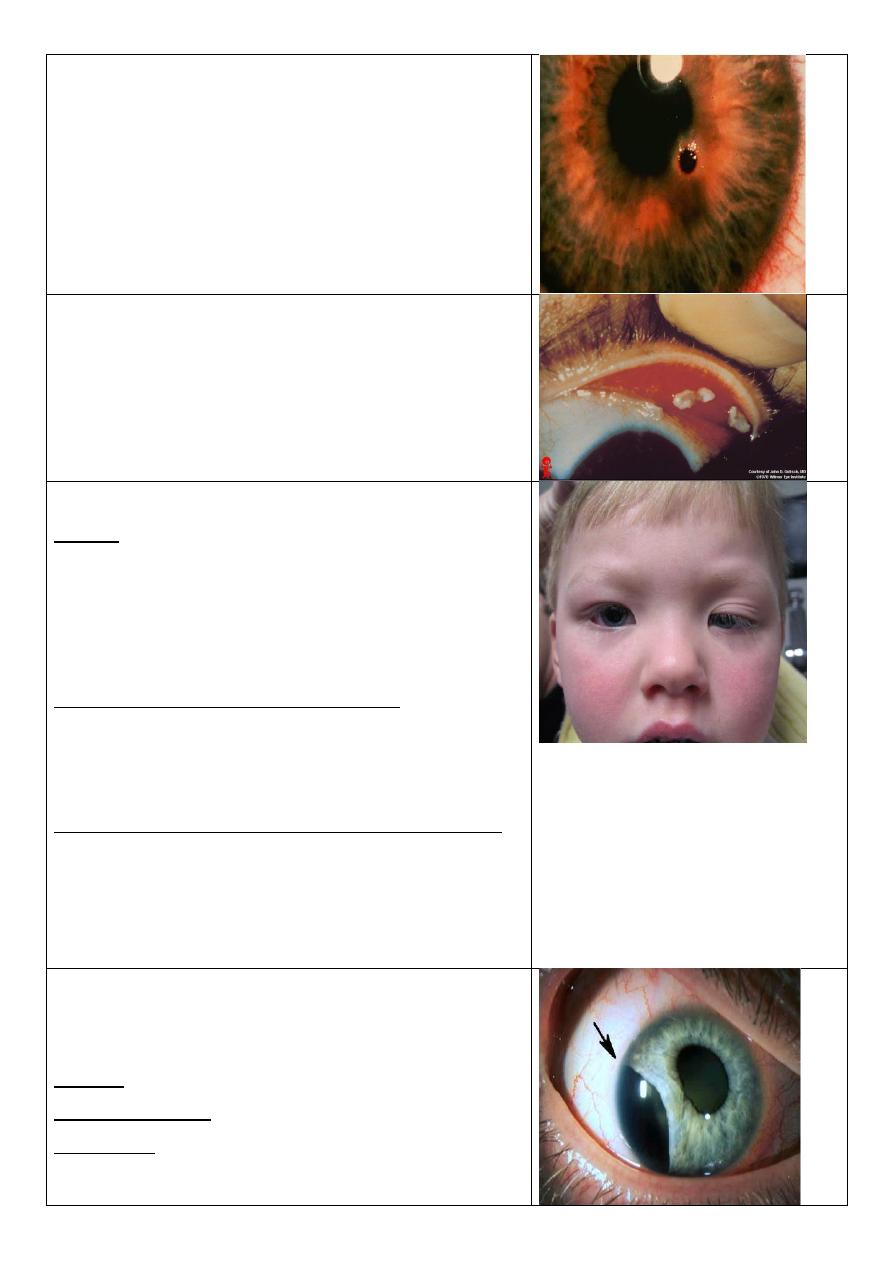
Cataract and dilated pupil
Any opacity in the lens is cataract (affect the vision or
not).
Causes of cataract:
1-age (commonest) 2-congenital
3-drugs like steroid 4-radiation 5-trauma
Causes of dilated pupil:
1- Drugs (sympathomimetic, anticholinergic)
2- Third CN palsy (parasympathetic damage)
3- Optic nerve damage
4- Traumatic mydriasis (damage of sphincter muscle)
Assess the state of fundus by:
1- Visual acuity.
2- Light perception (+ve other disease, -ve optic
damage).
3- Light perception (from which side the light come?).
4-pupillary reflex
5- Color discrimination (done by put color filter in the
slit lamp, it is used to check the function of optic
nerve).
6- B scan US.
Treated by surgery (extraction of lens).
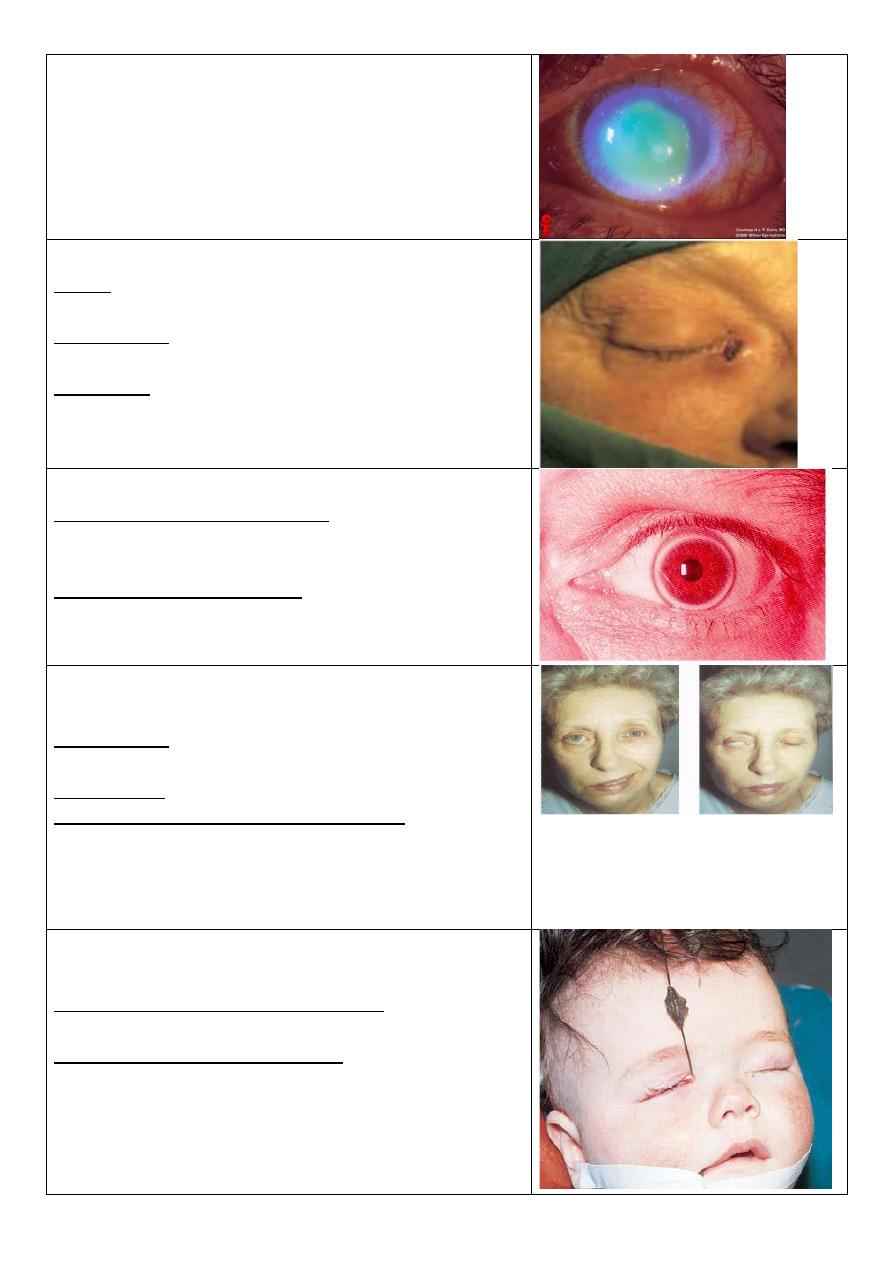
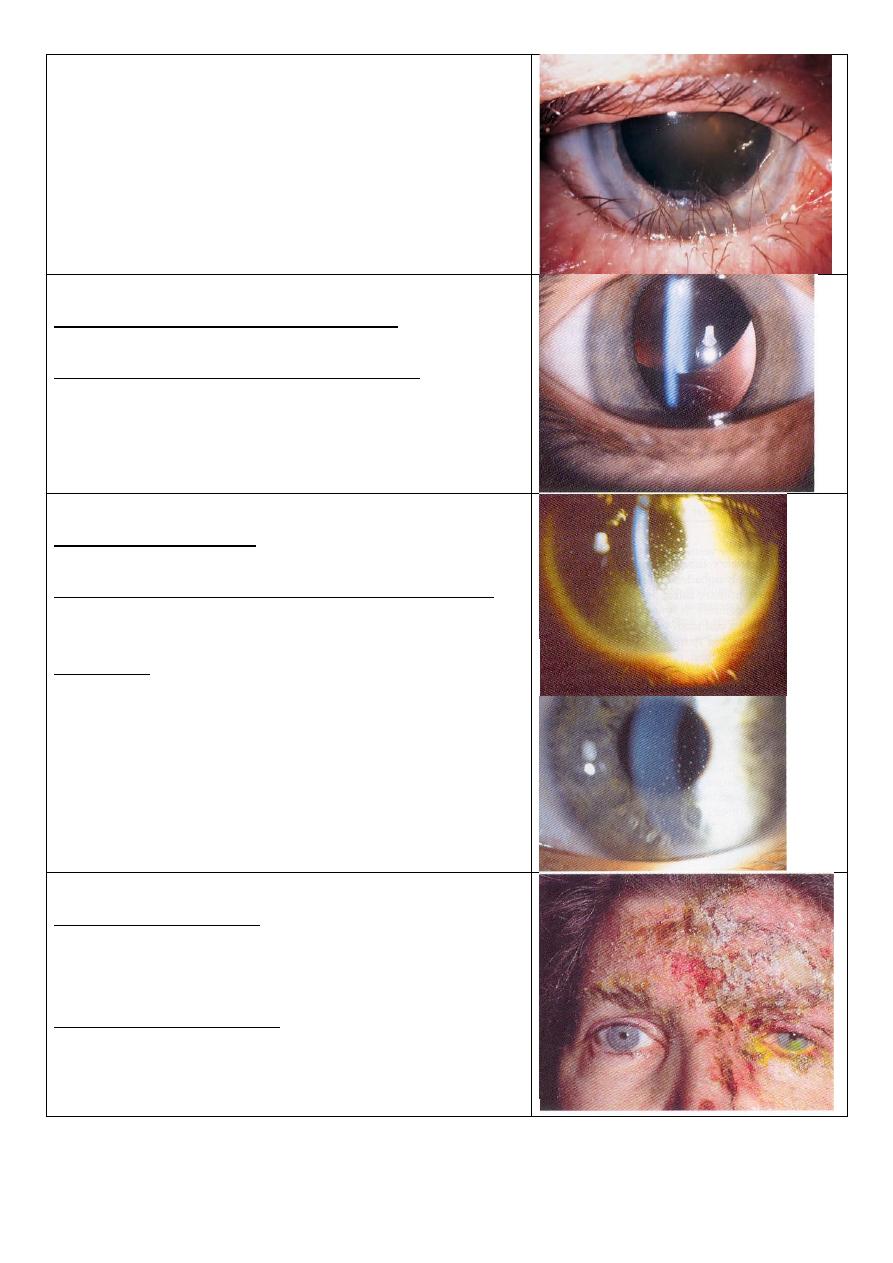
Hyphema
(blood in the anterior chamber)
+
subconjunctival hemorrhage + dilated pupil
Cause: trauma.
Cause of hyphema: Trauma is the major cause, surgery
(during & after), intraocular tumors, anticoagulant
treatment.
Assess IOP:
1- The blood will block the trabecular meshwork
space
no drainage
high IOP.
2- Wound on sclera or other parts
leak of eye fluid
low IOP.
Treatment:
1-bed rest with head elevated
2-anti-glucoma drugs if increased IOP
3-drainage of blood if high amount
8
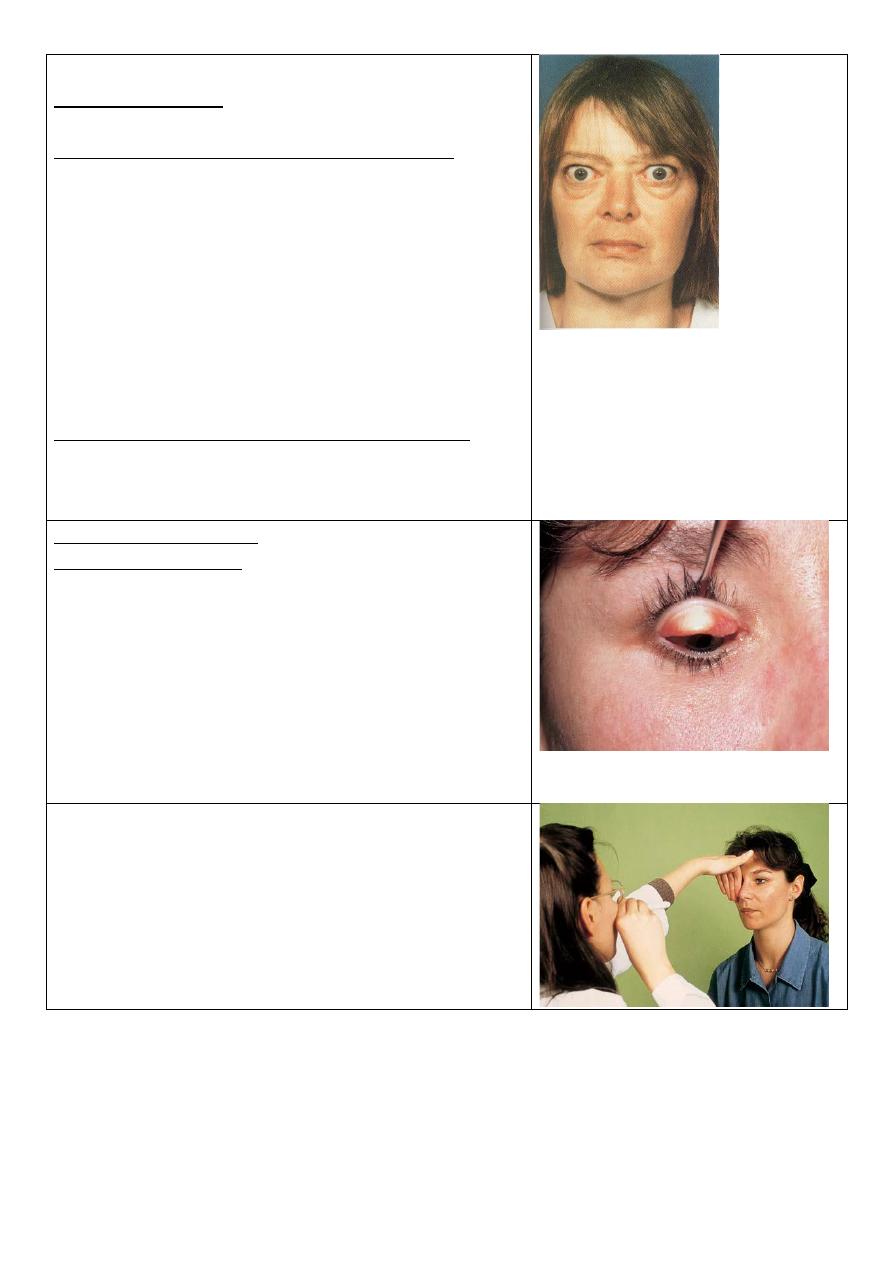
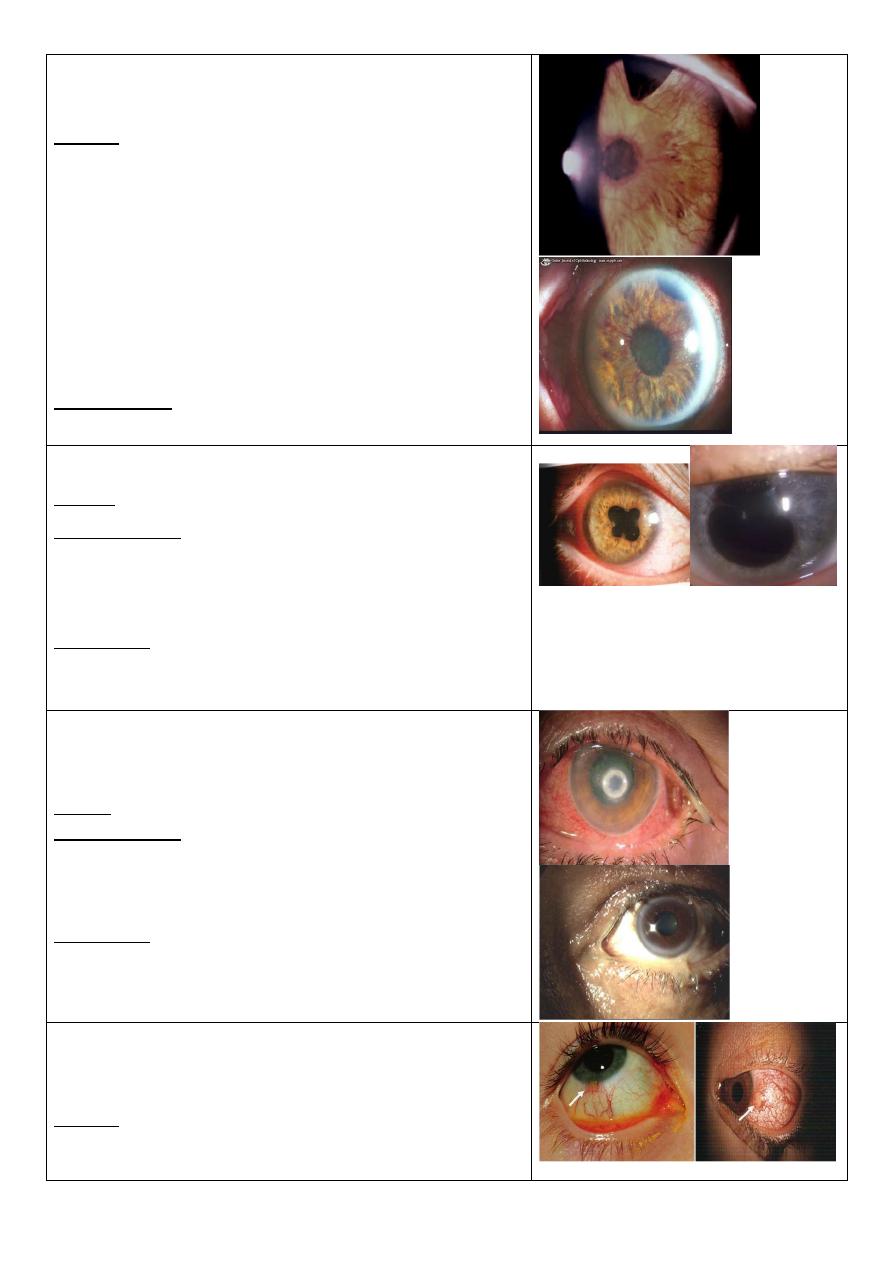
Subconjunctival hemorrhage
Ask the patient about trauma, straining (cough,
vomiting), bleeding tendency, drug.
HSV-1 eye lesion
Branching greenish discoloration of the cornea =
dendritic ulceration due to HSV-1 infection.
The color of fluorescence is orange but here we see it
greenish because we use the slit lamp filter.
Fluorescence stain has affinity to collage fibers, so
areas of no epithelium or removed epithelium will be
stained by the florescence stain.
Treatment: Acyclovir, trifluridine, idoxuridine.
Ameboid ulcer
Cause:
Mistreatment of dendritic ulcer by steroid.
Geographical ulcer
Fluorescein stain showing ulcer in the cornea.
Cobalt blue filter in slit lamp.
Causes: 1-steroids 2-chemical substances 3-bacterial
infections 4-F.B. 5-trauma 6-contact lens users
History: patient with HSV-1 wrongly treated by steroid
Treatment:
1- according to the cause
2- gradual decrease in steroids
3- antiviral (if dendritic)
4- patching and soft bandage (if traumatic)
9
Corneal ulceration
-Fluorescein stain showing corneal ulceration
-Same causes of any ulcers
-If we see pus in the anterior chamber (Hypopium) the
cause is bacterial.
Dacryocystitis
Cause: obstruction of the nasolacrimal system.
Most common organism is staphylococcus.
Presentation: painful swelling on the medial side of
the orbit, which is the enlarged, infected lacrimal sac.
Treatment:
1- Systemic antibiotics 2- Dacryocystorrhinostomy
(DCR) to prevent recurrence.
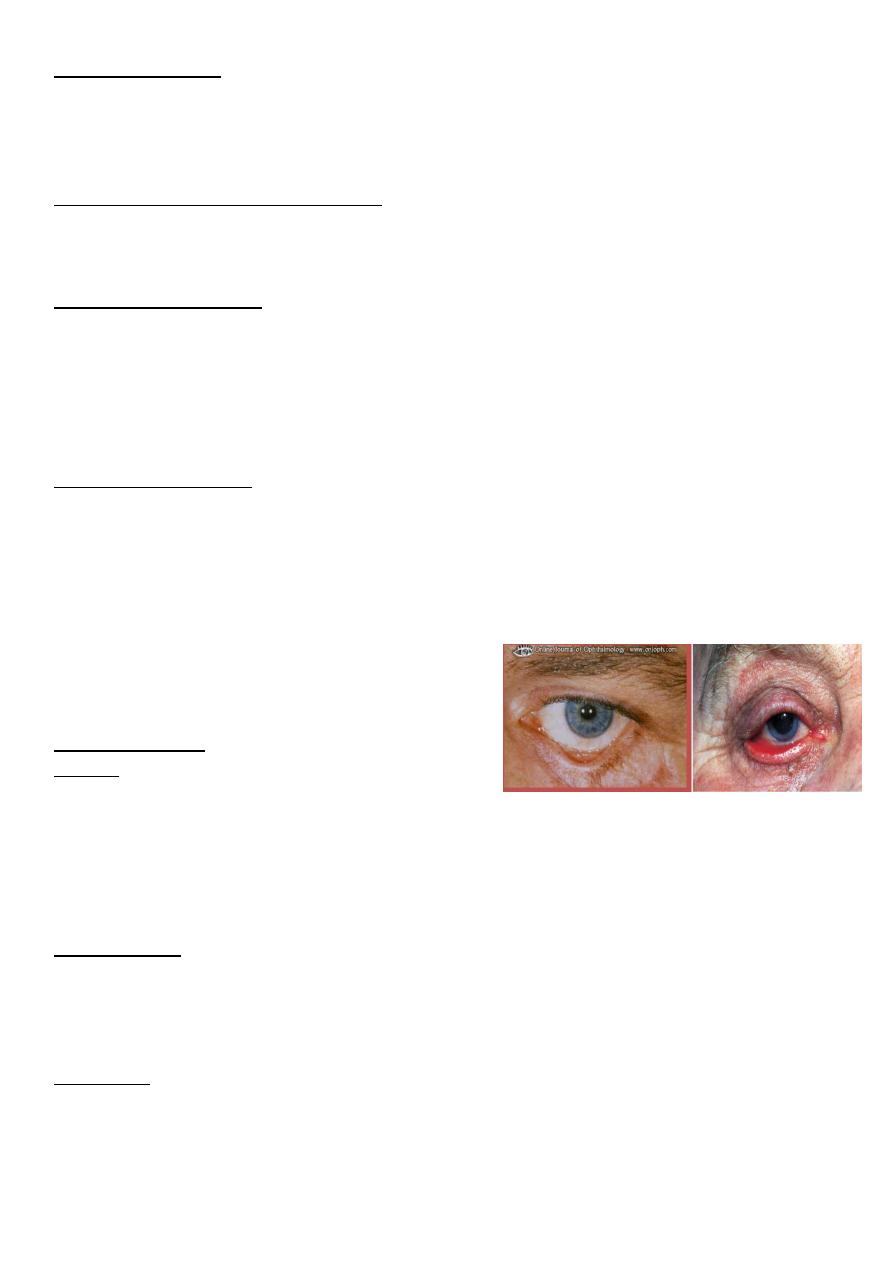
Corneal arcus (lipidis) or arcus senilis
What is the clinical significance? It indicate
hyperlipidemia in young people which may causes
systemic diseases.
What is the visual prognosis? It never affect
vision(never reach cornea)
Facial palsy on R. side with lagophthalmos &
Bell's phenomenon
Presentation: Mouth deviated to the left side, cannot
close right eye, eye pulled upward (bell's phenomina).
Significance? Exposure keratopathy
How do you treat the eye of this patient?
1-artificial tears in days
2-closure of eye at sleep (taping)
3-If chronic do surgery (lateral tarsorraphy)
4-shield glasses
Congenital failure of canalization of right
nasolacrimal duct
What is the presentation of this child? Lacrimation on
right side(epiphora) or conjunctivitis
What is the proper management?
1-reassurance of parents
2-topical AB with massage till the end of the first year
3-if not opend (after the first year, most open
spontaneously during the first year) probing and
irrigation with antiseptic solution
11
Ptergyium
Describe this lesion: Localized redness located at nasal
corner of the eye, triangular in shape with the apex
extend to involve cornea due to fibrovascular
ingrowths
Causes?
1- reflected or direct UV light exposure 2- irritation
3- Exposure to irritant materials (dust, smoke…)
4- SCC (mass) 5- fibrosis due to injury
Treatment? Surgical removal with conjunctival graft
What are the indications of surgery in this patient?
1-affect visual axis. 2-severe discomfort. 3- cosmetic.
4- poor vision. 5- dryness of cornea. 6-astigmatism.
Subconjuctival hemorrhage
What will you ask in the Hx? 1-history of trauma,
straining conditions (vomiting, constipation, cough)
2-history of hypertension. 3-bleeding tendency.
4-history of drugs: anticoagulants and NSAIDs.
Management: assurance of patient, resolved after 10-
14 days, it is simple condition put if the patient want
treatment you can give artificial tear or lubricants.
Membranous conjunctivitis
What are the possible causes?
1-true membrane: diphtheria.
2-pseudomembrane: most bacteria like staph +
adenoviral infection.
What is this sign? Papillae on the inner surface of
upper lid (giant cobblestones papillae)
What are its causes? vernal keratoconjunctivitis,
allergic conjunctivitis: atopic, seasonal, giant papillary
conjunctivitis.
Treatment:
Avoiding exposure to the causative allergen, topical
steroids, mast cell stabilizers, antihistamine, dark
glasses & cold compresses.
11
Corneal topography
Color coded map used for studying the shape,
curvature, refractive power of cornea in every point
with details.
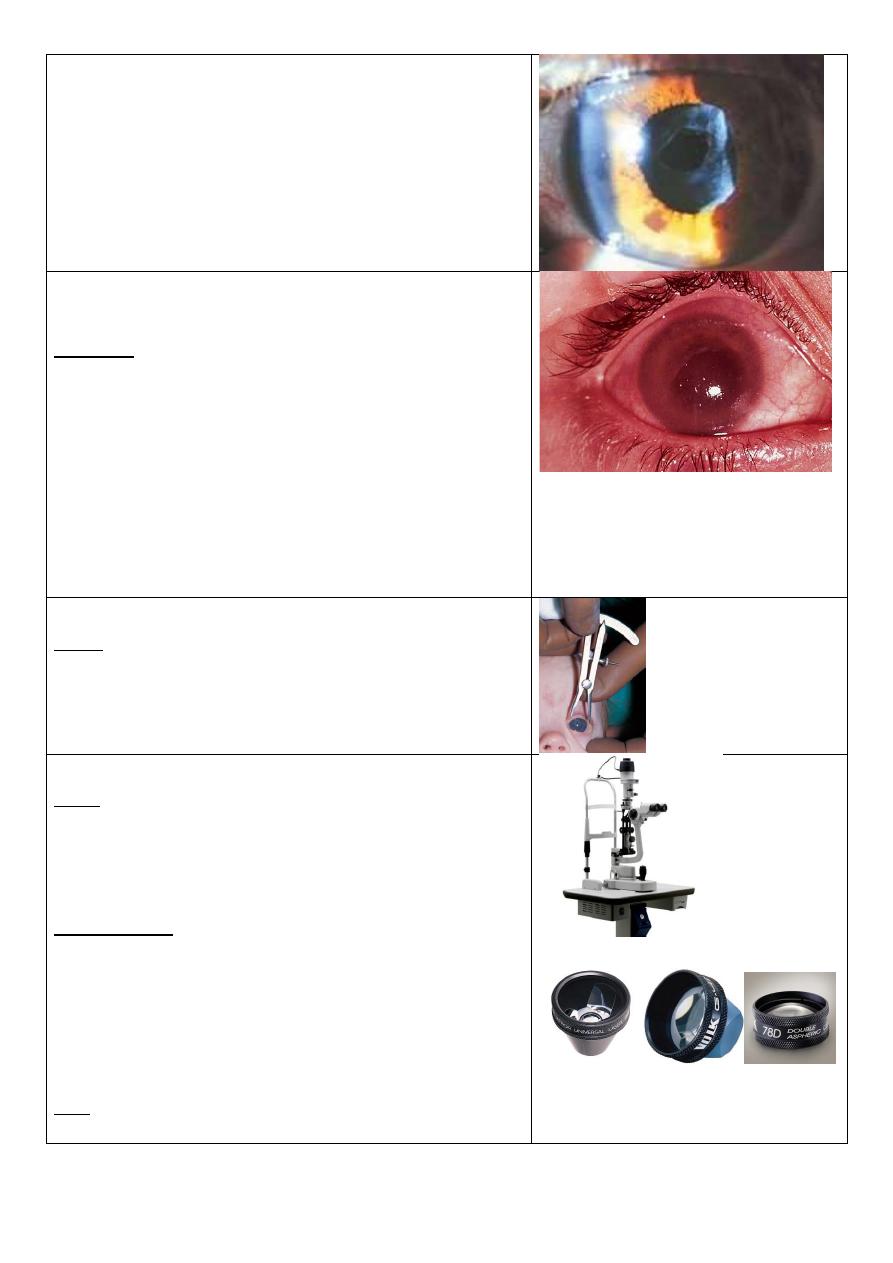
Staphyloma
-Occur in high myopia as the globe is large.
-Thinning of retina, bulging, exposed sclera.
US in high myopia
US showing large melanoma
B scan sonography showing the vitreous cavity
12
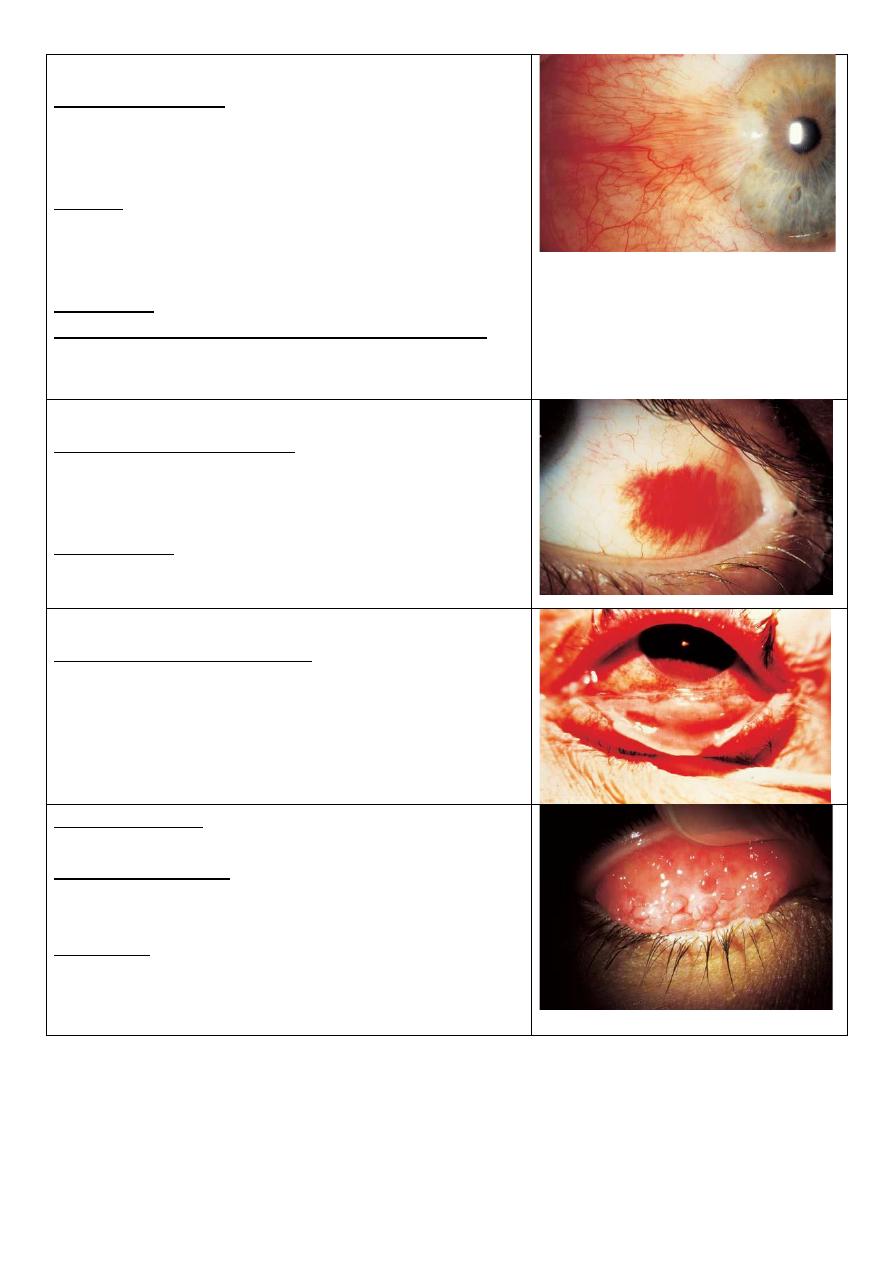
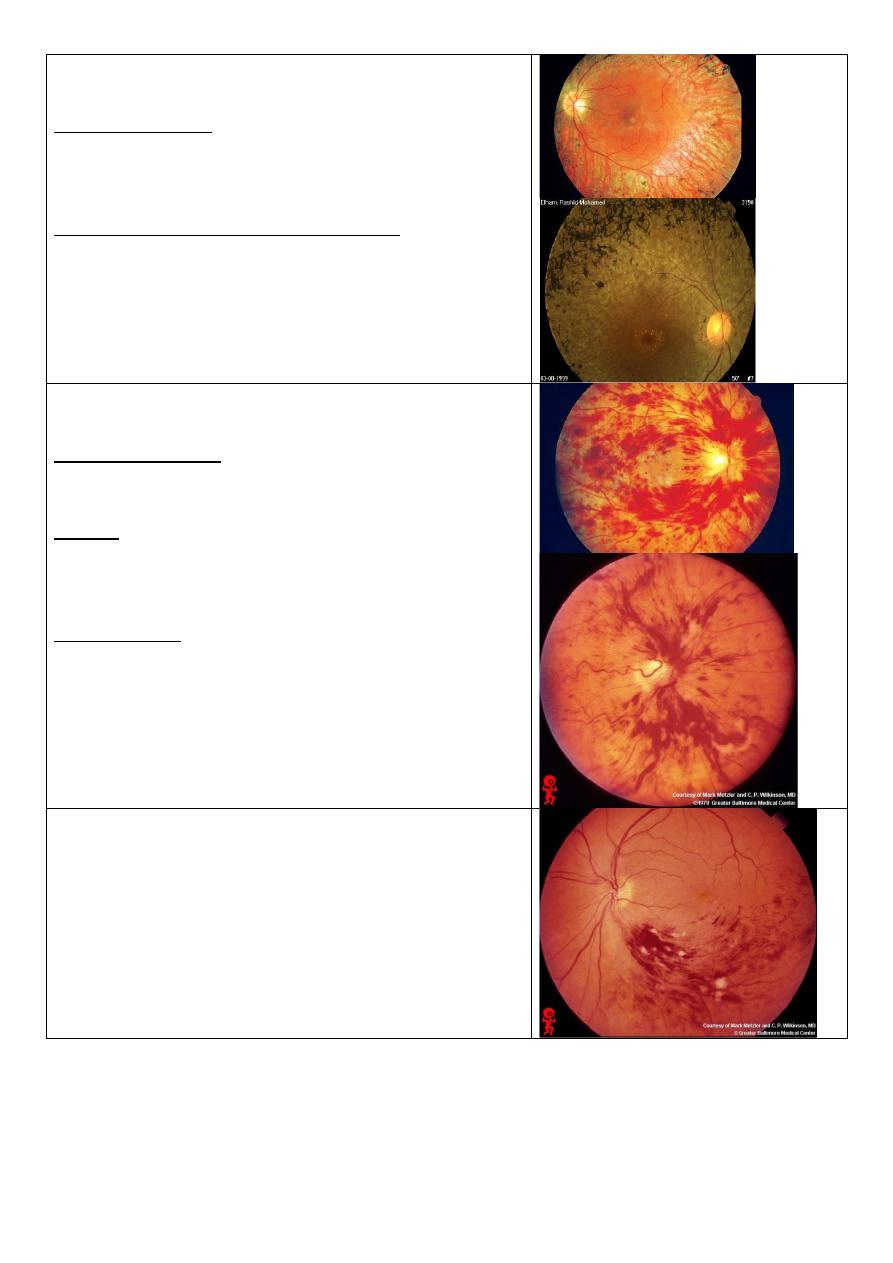
Leukocoria & pseudosquint
Describe the lesion? Right white pupil.
Enumerate the most common causes according to
their frequency?
1-congenital cataract.
2-retinoplastoma.
3-retinal fibrosis.
4-persistent hyperplastic primary vitreous.
5-retinopathy of prematurity.
Cause of pseudosquint: Epicanthal fold.
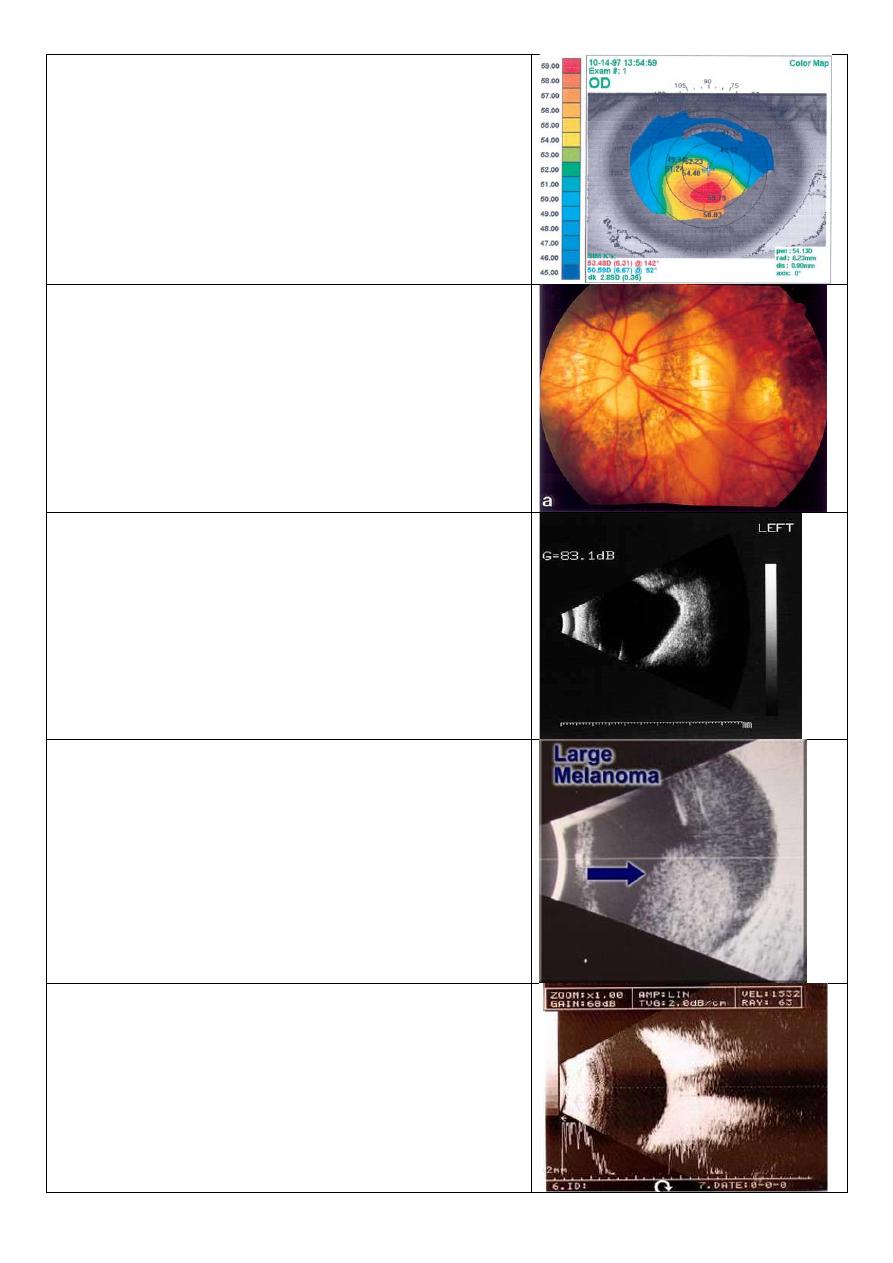
Scleritis
Symptoms/Signs: Pain, Significant ocular tenderness to
movement and palpation, Watering, photophobia.
Etiology: immune, associated systemic disease,
connective tissue disease, rheumatoid arthritis.
Treatment: underlying condition, NSAIDs,
corticosteroids, immunosuppression.
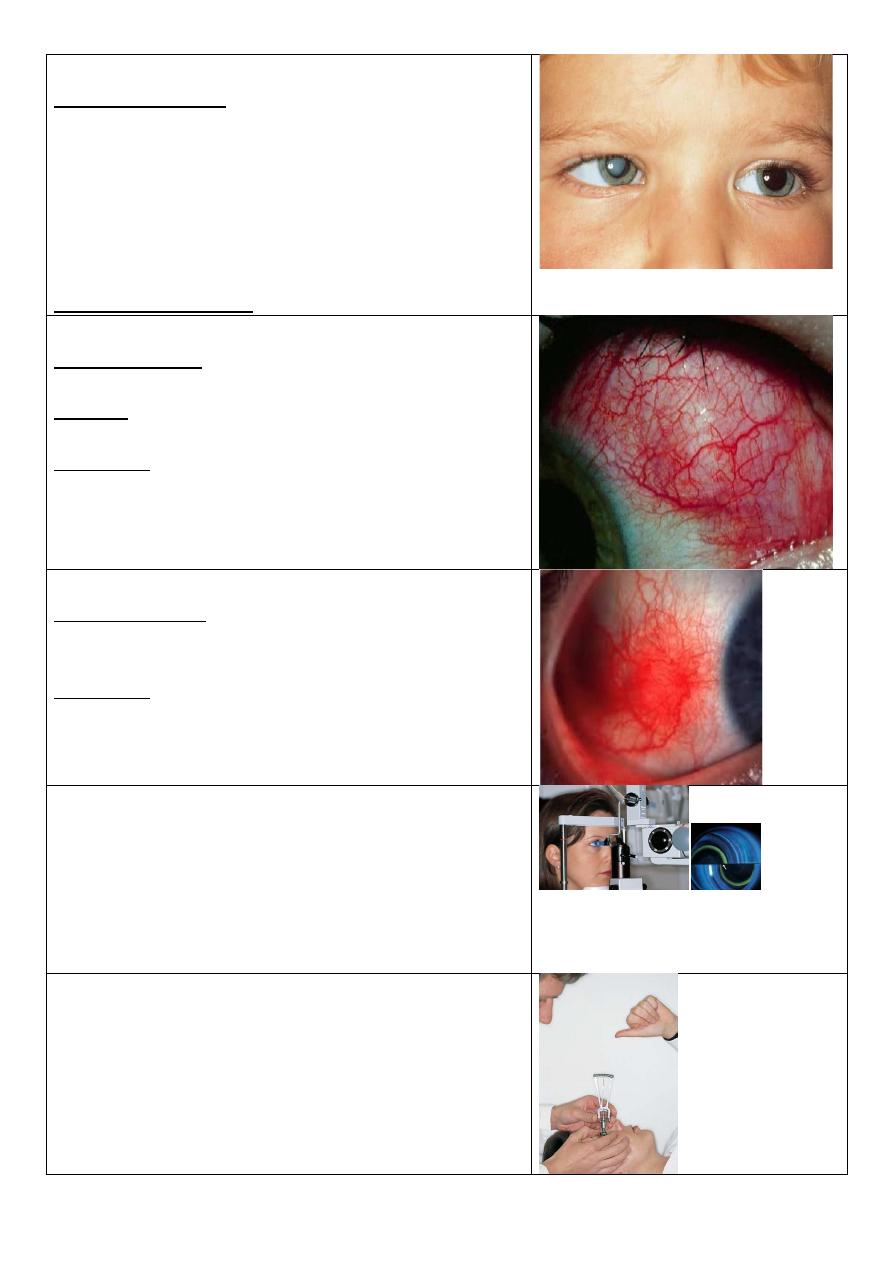
Episcleritis
Symptoms/Signs: Often asymptomatic, Mild tearing/
irritation, Tender to touch, Self-limiting (may last for
months).
Treatment: Lubricants, NSAIDS, Rarely low dose
steroids.
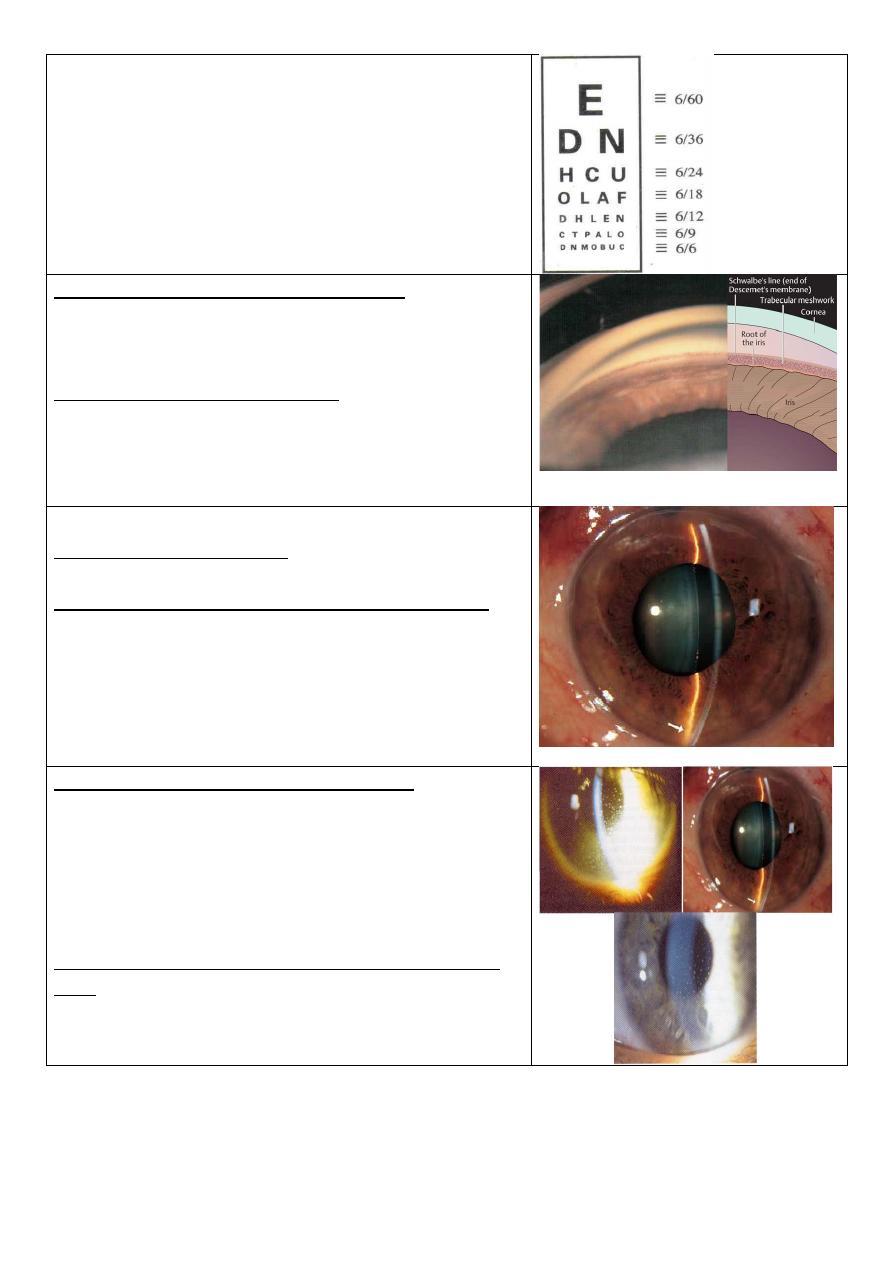
Goldmans applanation tonometry
Put florescence stain to the tear film then press the
external surface of eye by the tonometer and when it
become flat it means equalization of the pressure
inside and outside the eye, and the semi-circles will
meet each other, so take this point as IOP.
Schiotz tonometry
There are 3 things here:
1- Weight (g).
2- Degree of corneal indentation (mm).
3- Table of pressure measurement.
Pressure reversely related with the indentation.
13
Snellen's test
For assessment of visual acuity
By using which test we can get this view?
1- Gonioscopy (visualization of the angle of the
anterior chamber = irido-corneal angle)
2- With goniolens (for detecting glaucoma).
Describe the aqueous circulation:
It is produced by the ciliary process of ciliary body
>posterior chamber >pupil> anterior chamber
>trabecular meshwork> Canal of Schlemm>extraocular
veins.
Measurement of AC depth
Comment on the AC depth: Shallow anterior chamber
depth.
If this patient is asymptomatic, how you treat him?
1-Medical Tx: mitotic agents ,alpha agonist, b-blocker,
carbone anhydrase inhibitor, prostaglandin analogs
2-peripheral laser iridotomy (YAG laser)
*it consider pre-glaucoma so it is urgent.
3- hypermetropia: convex lenses.
4- Treatment of glaucoma: pylocarpin, iridotomy
Comment on the anterior chamber depth:
1) Eclipse sign: we shine a light on the temporal aspect
of the patient anterior chamber & watching the iris, if
the AC is deep the whole iris is illuminated, if the AC is
shallow, only the temporal part is illuminated.
2) Important in angle closure glaucoma.
If this patient is asymptomatic, how would you treat
him?
Miotic agents, alpha agonist, carbonic anhydrase
inhibitors and prostaglandin analogs.
14
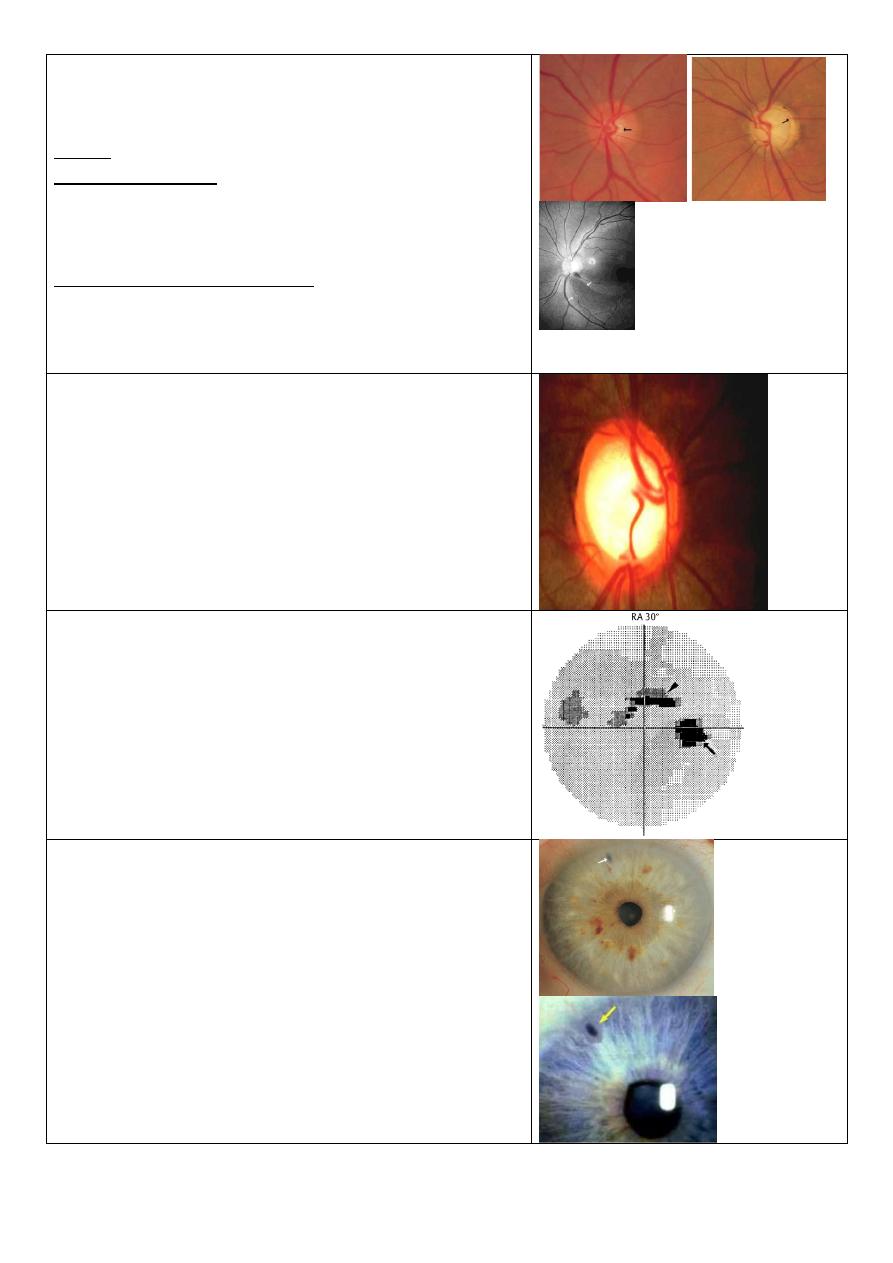
Abnormal cupping of the optic disk
(CD ratio > 0.3)
Normal cup:disk ratio 0.3 – 0.4
If CD ratio increase it means there is large cup.
Cause: primary open angle glaucoma
Criteria of cupping:
1-cup:disk ratio > 0.3.
2-progressive enlargement
3- asymmetrical between the two eyes.
Criteria to diagnose glaucoma:
1) Increased IOP. Normally 15±6 mmHg.
2) Abnormal cupping.
3) Changes in visual field.
Glaucomatous cupping of optic nerve
-Expected field of vision: Tubular field.
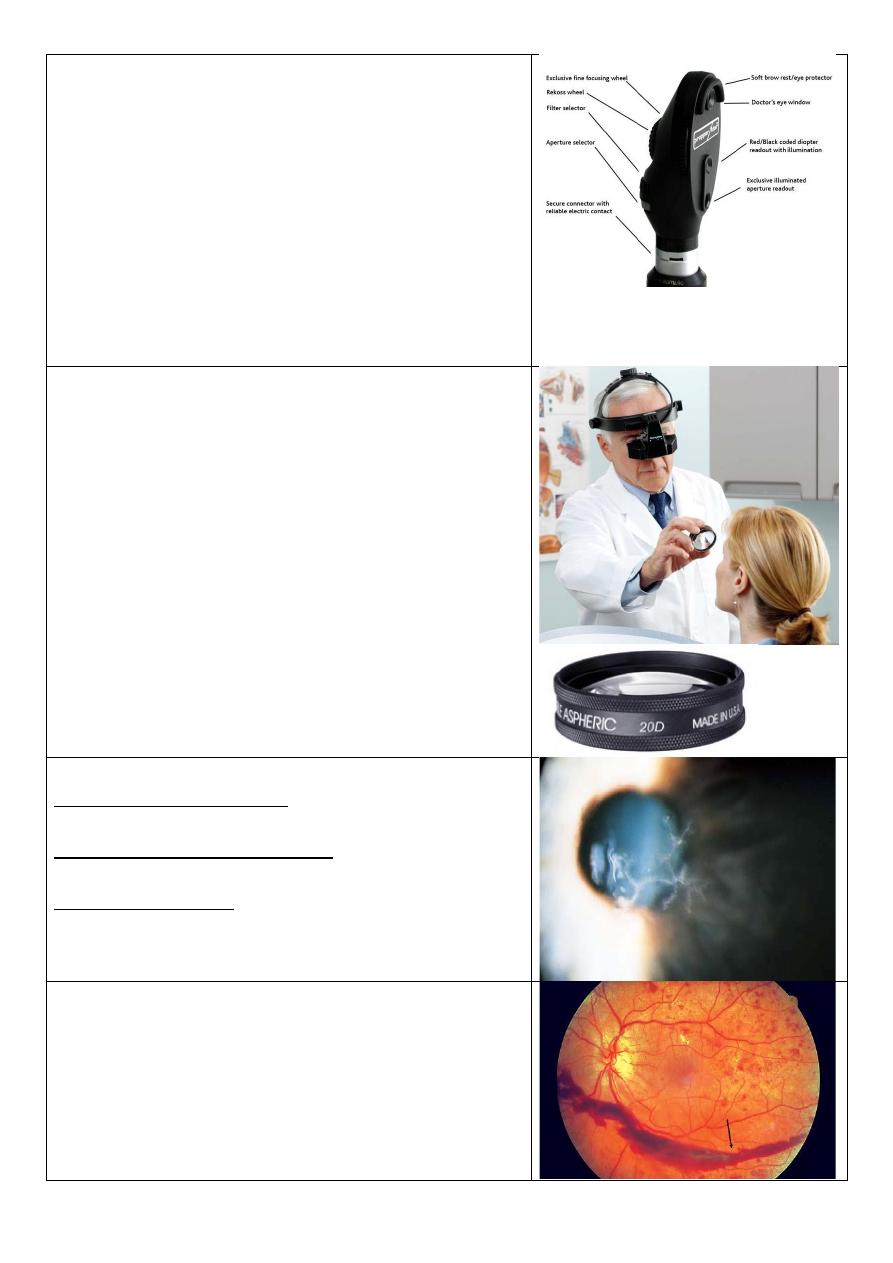
Automated static perimetry (visual filed)
perimetry graph showing paracentral scotoma in open
angle glaucoma
-No patient complain
-Diagnosed by chance
Peripheral laser iridotomy
Indication:
Shallow anterior chamber (angle closure glaucoma) so
we do it to make direct shunt between anterior and
posterior chambers.
15
Posterior capsule opacification
Treatment: YAG laser capsulotomy to open
thickened posterior capsule after cataract surgery.
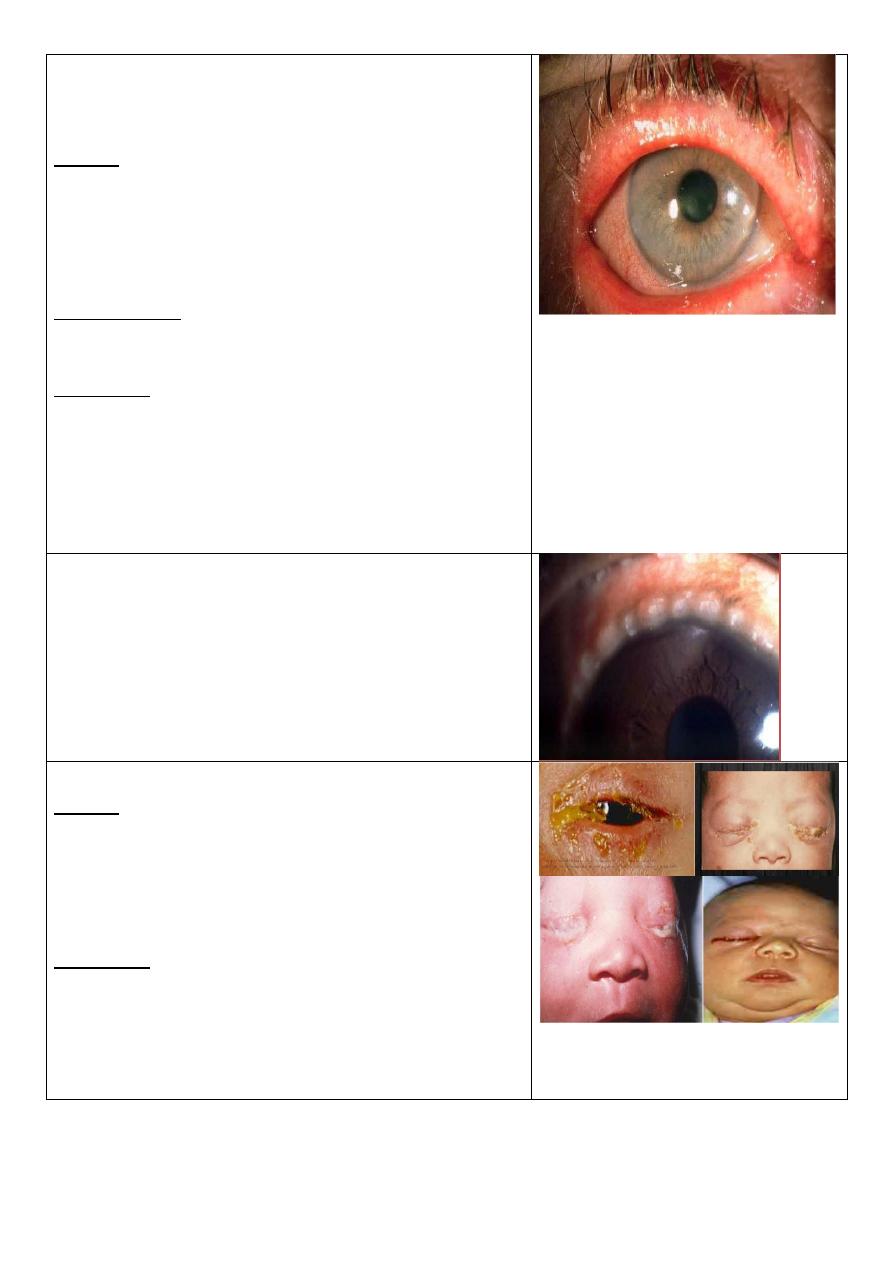
Dx: Red congested eye (acute angle closure glaucoma)
with corneal edema, ciliary flash and dilated pupil.
Features:
Painful red eye.
Achy, abdominal pain.
Misty vision.
Go from light into dark.
Small eye, shallow anterior chamber.
Pupil mild dilated.
Iris lens contact.
Push the iris forward.
Eye feels hard.
Measuring corneal diameter by caliber
Why?
To detect and follow up congenital glaucoma (
buphthalmos)
Slit lamp
Uses:
1- Examine the anterior segment of the eye.
2- Examine the posterior segment with special lenses.
3- Measure the IOP with Goldman aplination
tonometer.
Added lenses:
1-Goldman 3 mirrors contact lens (use topical
anesthesia, vescoelastic substance).
2-Central lens.
3-Dome shape lens (goniolens): used to see
iridocorneal angle (the test called gonioscopy).
4-Plus lens 78D (convex lens).
See: upside down and laterally reversed image (real
image) by using this instrument.
16
Direct ophthalmoscope
1-Portable, light instrument.
2-Examine the patient in any position (lying, setting,
standing).
3-Not specialized instrument (used by general
physician).
4-Cause magnification X15 times so see narrow field.
5-We can see the fundus without dilatation of it.
6-The image seen here is erect (virtual image).
7-This examination is affected by refractive error of
the patient so use the lenses inside this instrument.
8-Right eye-right hand-right eye.
Indirect ophthalmoscope
1-It is specialized instrument.
2-Need special training, difficult to use.
3-Magnification 3-5 times depend on the lens we use
so not see the fundus directly.
4-The field here is larger than in direct method.
5-Examine the patient with your both eyes.
6-Should dilate the eye of patient.
7-Not affected by refractive error of patient.
8-The 3D image (with depth) because we use both
eyes.
9-During retinal surgery the indirect ophthalmoscope
is instrument of choice.
10-Use +20 or +30 lens.
Describe this corneal lesion: Dendritic ulcer
What is the most likely diagnosis? HSV type 1
How would you treat? Antiviral drugs (acyclovir ,
trifluoridine and idoxuridine) // avoid steroids.
Subhaloid hemorrhage
Hemorrhage between retina & vitreous
17
Retinitis pigmentosa
Bone spicules, waxy disc & attenuated blood vessels.
Patient complains:
1-night blindness (nyctalopia).
2-visual loss
3-seeing flashes of light (photopsia).
Mention 2 syndromes associated with it.
1-bardet biedl syndrome
2-refsum syndrome
3- Autosomal dominant / recessive
Central retinal venous occlusion (CRVO)
Congested dilated blood vessels.
History (ask about):
Hypertension, hyperlipidemia, DM, smoking, obesity,
life style, psychological problems, stress.
Causes:
1) Extraluminal causes: hypertension & tumor.
2) In the wall: vasculitis.
3) Intraluminal: thrombus.
Complications:
1) Neovascular glaucoma.
2) Chronic macular edema.
Branch retinal vein occlusion
Occlusion of the lower temporal branch of retinal vein
marked by hemorrhage and multiple spots (cotton
wool spots) of ischemia in the lower temporal zone of
retina
18
Occlusion of Lower temporal and lower nasal branches
of retinal artery a marked by complete ischemia
Central retinal arterial occlusion (CRAO)
Attenuation & constriction of the arteries (cattle track
appearance), the whole retina is pale except the fovea
(cherry red spot) due to double blood supply.
Causes: Usually embolic.
History: ask same questions in venous occlusion.
Could lead to neovascular glaucoma (due to occlusion
of iris root by new vessels).
DDx For cherry red spot:
-Commotio retinae
-Quinine poisoning
-Macular hole surrounded by RD
-Amauratic family idiocy
Filamentray keratitis
Stain: rose bengal stain
Causes : 1-dry eye 2-sjogren syndrome
3- facial palsy 4-blepharoptosis
Presentation: patient with dry eye and the mucin
become thick and adhere to the cornea and give
sensation of F.B.
Hypopium
It is pus in the anterior chamber
Causes:
1- Infected: endophthalmitis (pneumococcus).
2- Sterile: severe iritis.
3- keratitis.
4-any inflammation or infection.
19
Hypopium with cloudy cornea and red eye
Describe this lesion?
Nodulo-ulcerative lesion Oval, elevated, ulcerated,
congested, dirty lesion on the lower lid
Differential diagnosis?
1-basal cell carcinoma
2-sequamous cell carcinoma
3-sebaeous cell carcinoma
4-keratoacanthoma
5-malignant melanoma
Chalazion
Describe this lesion Localized swelling in the upper lid
with normal skin over it
Enumerate four causes
1-chalazion 2-stye 3-sebaceous cell carcinoma
4-haemangioma 5-blockage of tarsal glands
6-Seborrhea 7-Chronic blepharitis 8-Acne rosacea.
How would you treat it?
1-conservative: massage, hot compress, AB ointment,
local steroid.
2-surgery: surgical incision and curettage of the gland.
Ectropion of the right lower lid
What is the complaint of this patient?
Lacrimation, congested red conjunctiva, repeated
infections.
What are the possible causes?
1-aging 2-congenital 3-lower lid scar
4-faiacl palsy 5-neurofibromas 6- mechanical cause
21
Entropion of the lower lid with trichiasis
What are the possible causes?
1-aging
2-congenital
3-palpebral conjunctival scaring
4- trachoma, trauma, infection, inflammation
Lens dislocation (ectopic lens)
What are the possible visual symptoms? Blurred vision
and diplopia and refractive errors.
Enumerate three possible systemic causes:
1-trauma
2-marfan syndrome
3-homocystinuria
4-high myopia (eye problem)
Keratic precipitate (white dots in cornea)
What is your diagnosis? It is a feature of iritis or
anterior uveitis
What do you think the presentation of this patient?
Blurred vision, photophobia, pain, redness, and
lacrimation.
Treatment:
1- topical: atropin sulphate and corticosteroid
2- systemic: steroids (severe cases) or AB (infected
cases)
Herpes zoster ophthalmicus
Describe the skin lesion:
Erythematous base lesion with crust, pastule and
some sloughing involving forehead and side of the
nose and upper + lower lid of lift eye.
Describe the ocular lesion:
FLOURESCEIN stain showing corneal ulcer of left eye+
skin lesion involve upper + lower lid.
21
Thyrotoxicosis
Describe this facies:
Staring facies with periorbital edema
Enumerate four ocular features of this disease:
1-lid lag
2-lid retraction
3-exophthalmos
4-excessive lacrimation
5-Chemosis.
6-Periorbital soft tissue changes as chemosis & lid
swelling.
7-Exposure keratopathy.
8-Ophthalmoplegia.
Enumerate four systemic features of this disease:
1-sweating 2-palpitation 3-tremor 4-tachycardia
5- Goitre 6- Increased appetite with loss of weight
What is this procedure? Eversion of upper lid
What are its benefits?
1-very simple
2-F.B. detection
3-papillae detection
4-follicular reaction detection
5- Arlet line of trachoma.
6- Giant papillary conjunctivitis.
7- Adrenochrome deposits.
8- Melanoma.
9- Conjunctival concretion.
What is this procedure?
• Cover/uncover test
In which disease you want to use it in your
examination?
• Used to detect inapparent squint (phoria)
22
Retinal detachment
Left complete ptosis
What are the possible causes?
1- 3
rd
palsy 2-congenital 3-birth injury 4-horner
syndrome
Would you go for surgery for this child? Yes, to avoid
amblyopia or reduction of visual acuity and here we do
sling procedure.
Munson sign
Describe what you see: This patient asked to look
down, lower lid is seen pushed by cornea due to
increased corneal curvature with opacity.
What is the disease? Keratoconus with acute hydrops
Significance: It is one of the common causes of
reduction in visual acuity (myopia & Astigmatism).
Diagnosis of keratoconus:
1-Ask the patient to look down.
2-Placido disc.
3-Corneal topography (green normal, blue depression,
red elevation).
4-Keratometry (give the reading in diopter).
What are the lines of treatment for this case?
1-contact lens or patching
2-hypertonic drops to cause withdrawal of hydrops
3-corneal graft
Lines of treatment of keratoconus in general:
1- Corneal Collagen Cross-linking, in early cases to
arrest the disease
2- Glasses
3- Contact lenses (Rigid)
4- Shaving the corneal surface
5- Intra-stromal corneal rings
6- Penetrating keratoplasty or Lamellar
keratoplasty..in advanced cases or corneal scarring
23
• Is it a concomitant or incomitant squint? incomitant
• Which muscle is affected? Right lateral rectus
• What is the nerve supply? Abducent nerve
• concomitant: angle of squint not changed in
different visual directions
• incomitant: angle changed
Marcus - Gunn phenomenon
Pathogenesis:
Faulty Innervation (motor fibers from 5th nerve reach
levator instead of the 3rd nerve).
Astigmatism
Treatment:
Cylindrical lenses & refractive eye surgery
.
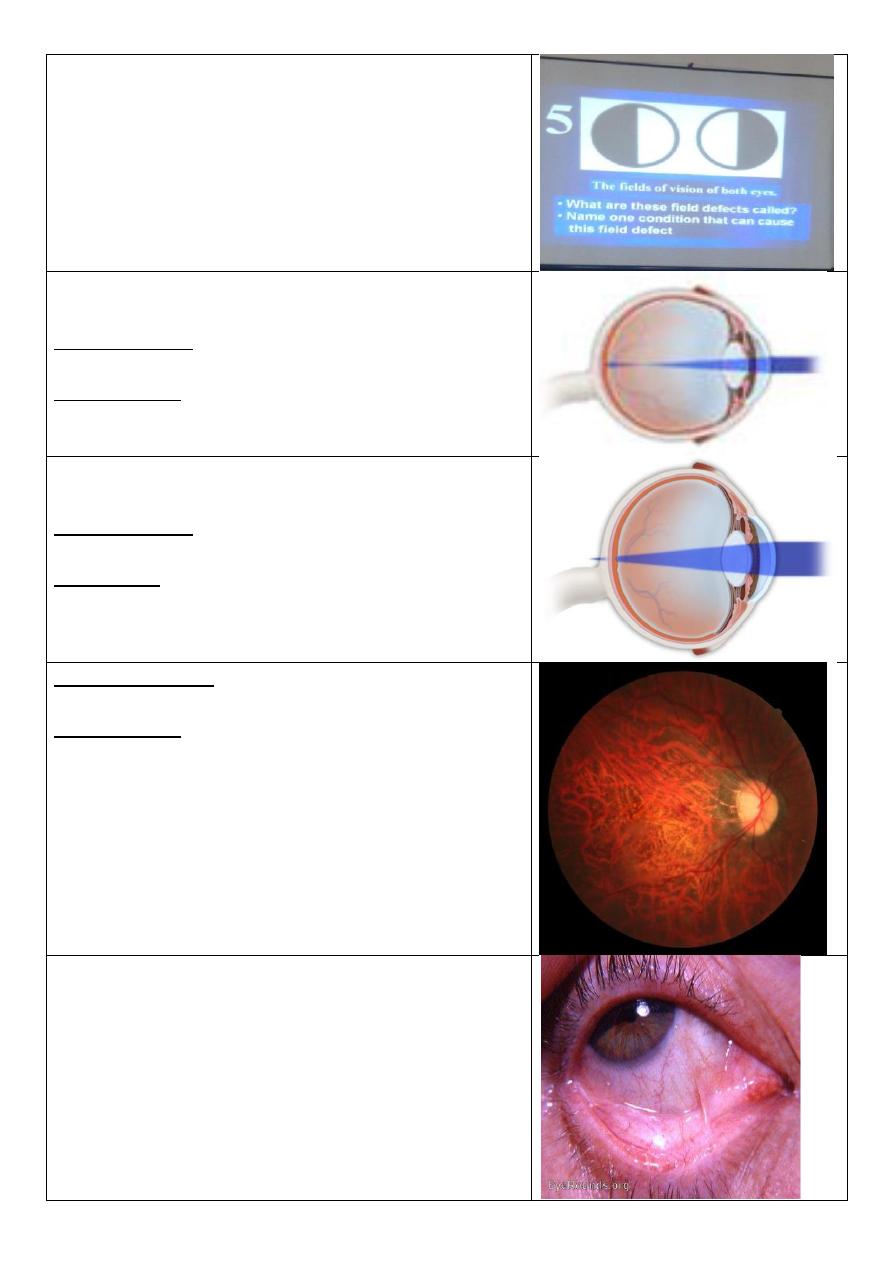
Papilleodema
Cause:
Elevated intracranial tension.
24
Chemosis
Edema of the conjunctiva.
Causes:
1) Conjunctivitis.
2) If drainage of blood & lymph from around the eye is
obstructed.
Describe:
Upper eyelid eversion, follicular formation.
Causes:
Trachoma & viral conjunctivitis.
Red congested eye
Common Causes:
1- Conjunctivitis.
2- Acute iritis (ant. Uveitis).
3- Keratitis (Corneal Ulcer).
4- Angle closure glaucoma.
5- Episcleritis (& scleritis).
6- Subconjunctival hemorrhage.
7- Dry eye.
Esotropia: convergent
Exotropia: divergent
Buphthalmos
Surgical procedures:
1) Goniotomy.
2) Trabeculotomy.
25
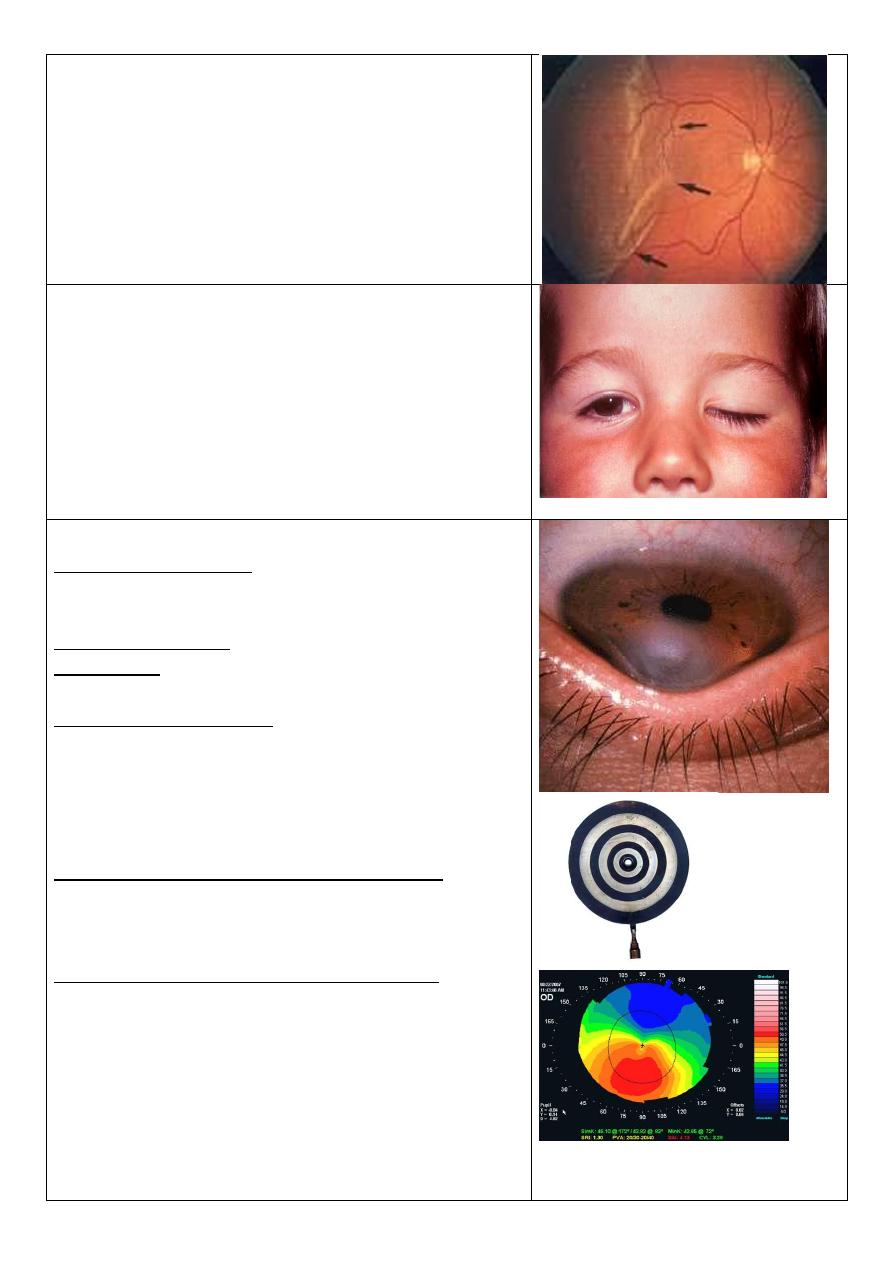
Bitemporal hemianopia
Caused by: Optic chiasma lesions (nasal fibers damage)
e.g. Pituitary gland tumor.
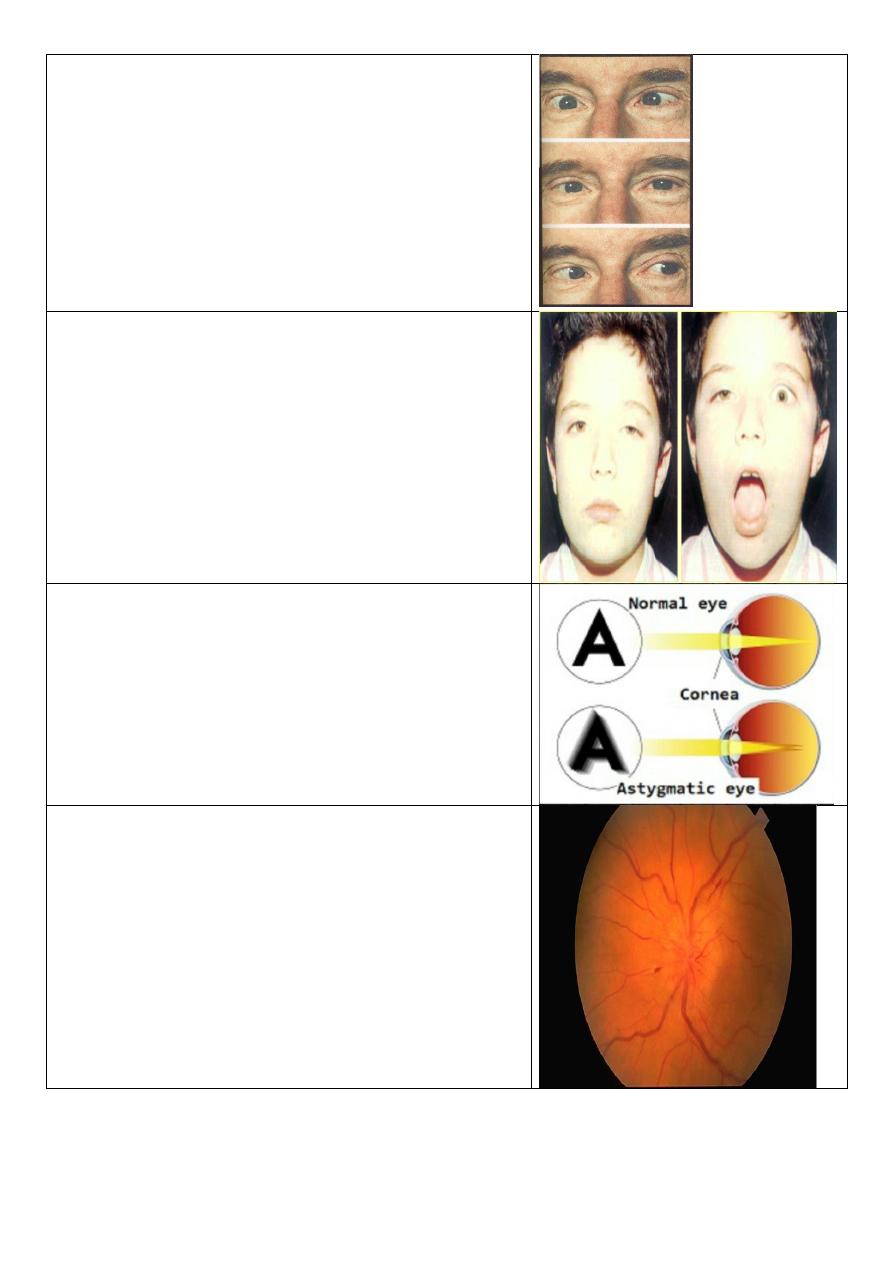
Myopia
Correction is by: Concave lenses (-) & refractive eye
surgery.
Complications: Retinal detachment, macular hole,
open angle glaucoma.
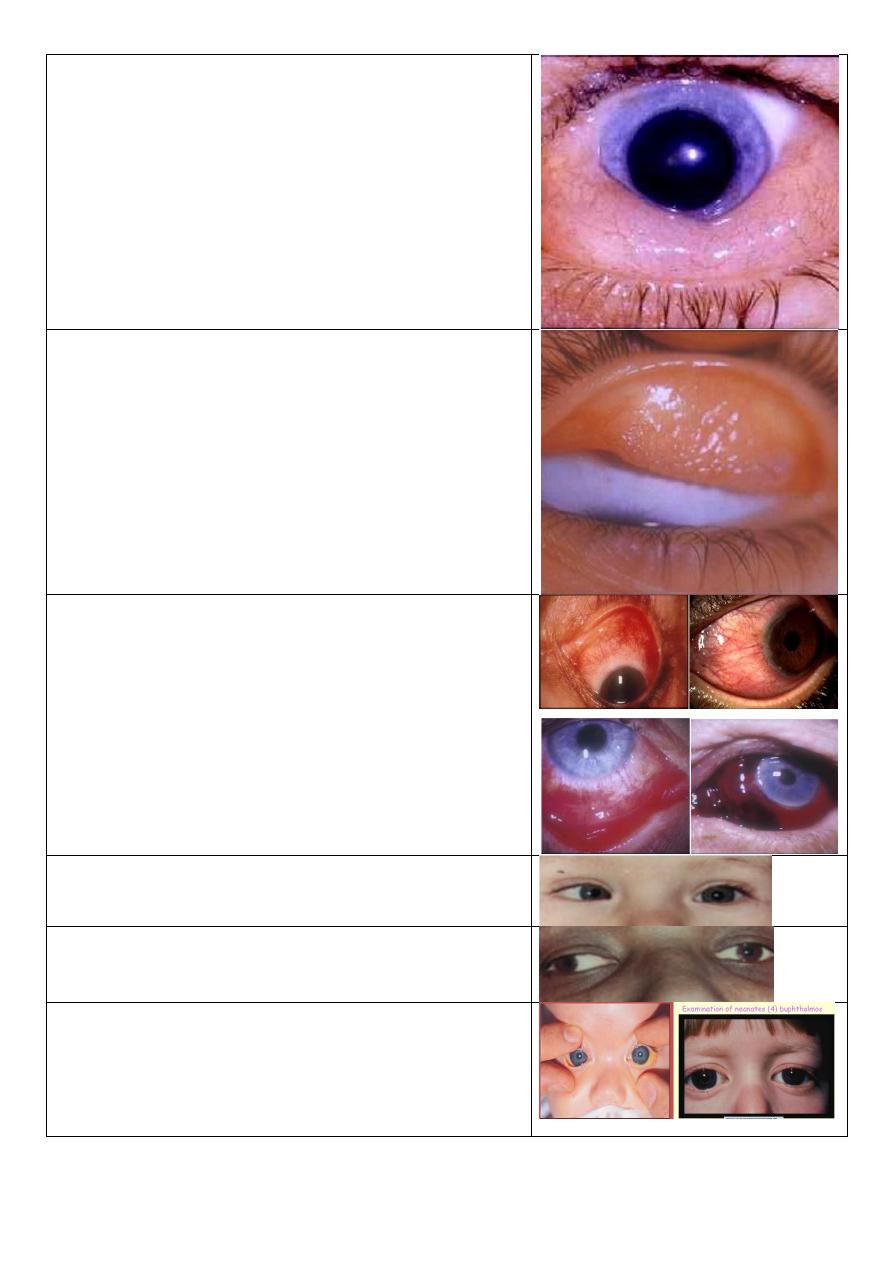
Hypermetropia
Correction is by: Convex lenses (+) & refractive eye
surgery.
Significance: Angle closure glaucoma as a
complication.
Error of refraction: High myopia.
Complications:
1) Chorio-retinal degenerations.
2) retinal tears.
3) retinal detachment.
Symblepharon
Causes:
1) Post-trachomatous.
2) Post-operative (Pterygium excision).
3) Ocular cicatricial pemphigoid.
26
Corneal foreign body.
Treatment: Surgical removal.
F.B. in the inner surface of upper lid
Left partial ptosis
Causes:
1) Oculomotor nerve palsy.
2) Horner syndrome.
3) Birth trauma.
4) Congenital.
Factors affecting prognosis & treatment:
1) Is the pupil covered by the ptotic lid or not?
2) Are there significant refractive errors between the
eyes?
The significance is developing of amblyopia (causes):
1) Strabismus amblyopia due to squint.
2) Anisometropic amblyopia due to deferent refractive
errors.
3) Deprivational amblyopia.
Iridodialysis
A dark crescentic gap at the edge of the iris where the
tear has occurred.
Causes: Trauma, Tumor excision.
Patient complaint: Uniocular diplopia.
Treatment: Surgical reduction and suturing of the iris.
27
Rubeosis iridis
(Growth of blood vessels onto the
iris)
& Peripheral iridectomy
Causes:
1) Diabetic retinopathy.
2) Central retinal vein occlusion (CRVO).
3) Long standing retinal detachment.
4) Ocular ischemic syndrome.
5) Hyoptonus eye.
6) Long standing uveitis.
7) Uveal melanoma, Retinoblastoma.
Complication: Rubeotic glaucoma & prognosis is very
bad.
Posterior Synechiae
Cause: Anterior uveitis (iritis).
Complications:
1) Band keratopathy.
2) Bulus keratopathy.
3) Cataract, Glaucoma.
Treatment:
1) Atropine & corticosteroid drops.
2) Surgical separation (synechialysis).
Mucopurulent conjunctivitis
Diffuse redness of the sclera with yellowish
mucopurulent discharge & eyelid edema.
Cause: Trachoma.
Complications:
1) Membrane formation.
2) Subsequent scarring of the punctum.
3) Corneal ulcer.
Treatment:
1) Eye lotions, Hot foments.
2) Antibiotics ointments e.g. tobramycin at night.
3) Antibiotic eye drops (tetracycline).
Phlyctenular conjunctivitis
Small pinkish-yellow nodule surrounded by a zone of
dilated blood vessels at corneoscleral junction.
Causes:
Hypersensitivity reaction (type 4) to endogenous
antigens e.g. bacterial antigens as T.B & Chlamydia.
28
Ulcerative blepharitis
Erythema & crusting of the lashes and lid margins &
adherence of the lashes with each other by oily debris.
Causes:
1) Herpes simplex & Varicella zoster dermatitis.
2) Allergic or contact dermatitis.
3) Bacterial infection (Staph.) is the usual pathogen.
4) Exposure to smoke, fumes & other irritants.
5) Sjogren syndrome may be present as blepharitis.
Complications:
Chronic conjunctivitis, Madarosis, trichiasis, Poliosis,
epiphora, Ectropion, corneal ulcer.
Treatment:
1) Eyelid margin hygiene (warming, washing &
application of antibiotic ointment to the lid margins).
2) Antibiotic – corticosteroid solutions to reduce
inflammation if the cause is bacterial.
3) Antivirals.
4) Avoiding exposure to irritant materials.
Bulbar spring catarrhal
Treatment:
Avoiding exposure to the causative allergen, topical
steroids, mast cell stabilizers, anti-histaminic dark
glasses, cold compresses.
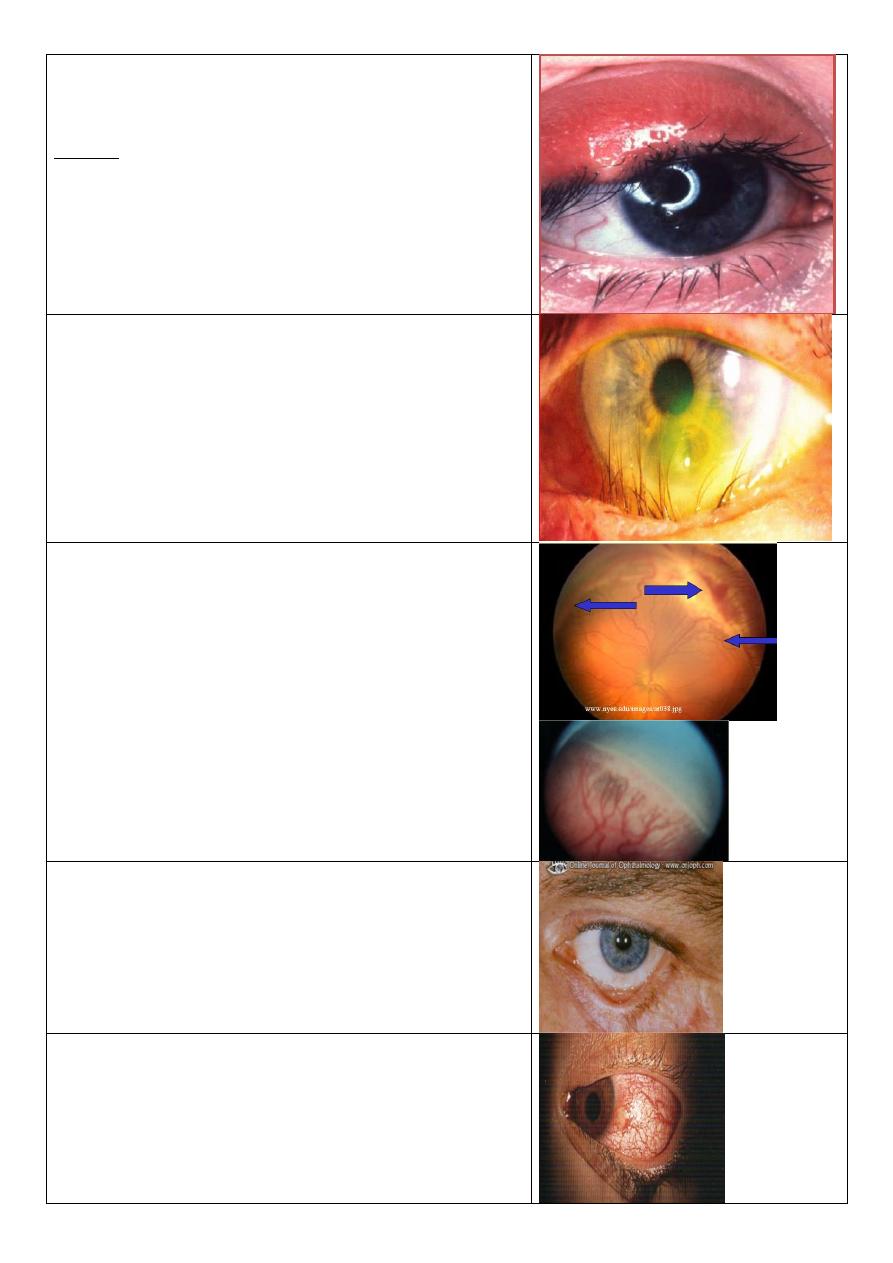
Ophthalmia neonatorum
(neonatal conjunctivitis)
Causes:
1) Chemical (silver nitrate).
2) Bacterial (1st 3 days=Staph.aureus , after the 3rd
day= Strept.peumonia , after the 1st week=Neisseria
gonorrhea , after 12 days=Chlamydia).
3) after 15 days= H. influenza & herpes simplex virus).
Treatment:
1) Gonococcal infection treated by cefotaxime for 7
days.
2) Chlamydial infection by systemic erythromycin.
3) Herpes by I.V acyclovir.
4) Topical antibiotic for staph.
29
Stye
Red swelling of the upper eyelid due to inflammation
of eyelash follicles.
Causes:
Bacterial infection staph. Aureus infection.
Treatment:
1) Local antibiotics & eye drops.
2) Bathing in warm water.
3) Removal of the eyelash involved.
Entropion with trichiasis & corneal ulceration
Retinopathy of prematurity
• in premature babies peripheral retina is not
vascularised at birth
• Under certain conditions instead of the
vascularisation proceeding normally, there is a
growth of new vessels and scarring
• 100% oxygen, crucial period 28-36weeks, especially
low birth weight
• vascularisation
• Laser peripheral retina
• Without laser,retinal detachment/blindness; have
to check (screen) all appropriate neonates
Cicatricial ectropion
Treatment: V to Y plasty or Z plasty
Phlycten
Causes:
Hyper sensitivity to an endogenous antigen e.g.
tuberculo-protein, Intestinal parasites, staphylococcal
blepharoconjunctivitis.
31
Acute congestive glaucoma
2 Medications for emergency: hyper-osmotic agent,
topical miotics, topical steroids
Treatment: essentially surgical recent….surgical
iridectomy late….their is PAS, an external fistulizing
operation.
Nerve& muscle affected: Right Abducent nerve - right
lateral rectus
Direction of gaze: To the right
Main complaint: Binocular Diplopia
Type of squint: exotropia
angle: 30
Confirmatory test: Cover test
After cataract
Treatment:
- No interference if vision is not affected
- If thick : surgical intervention
Senile ectropion
Possible complications:
1- xerosis
2- corneal ulcer
31
Ecchymosis & subconjunctival haemorrhage
Possible findings:
Concussion cataract " Rosette-shaped"
Lens subluxation or dislocation
Lens subluxation
Causes:
1- Marfan's syndrome
2- Homocystenuria
3- Trauma
4- High myopia
Symptoms:
Blurred vision, diplopia, increase IOP, pupillary block
(glaucoma), affected visual fields.
S
ublaxated & cataractous lens
Complications:
lens dislocation
2ry Glaucoma
Iridocyclitis
Blood staining of the cornea
“total hyphema or 8-
ball hyphema”
Complications:
Elevation of IOP
Corneal staining
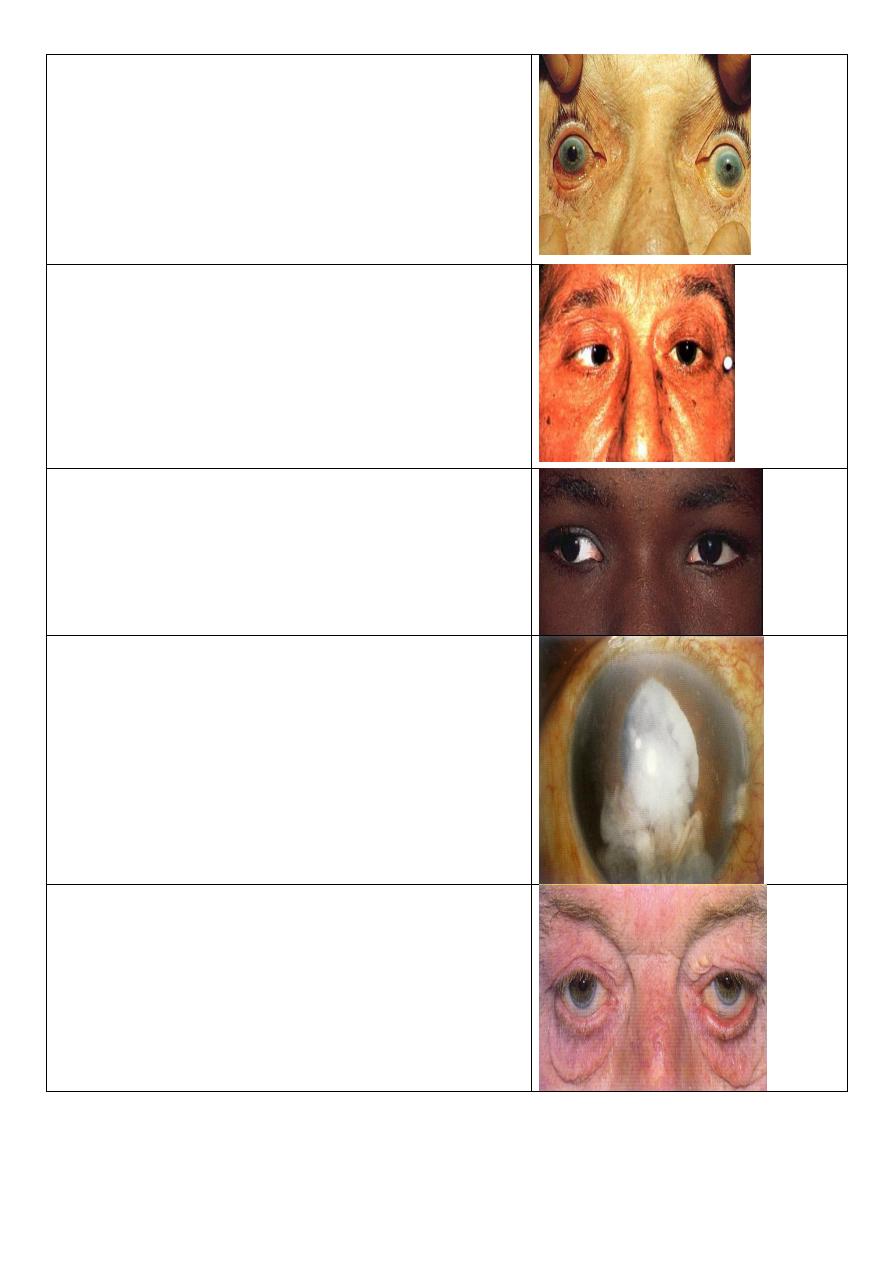
Sederosis bulbi
Patient with foreign body in his eye from one year
In picture you will see one eye normal &other
eye(black iris)
32
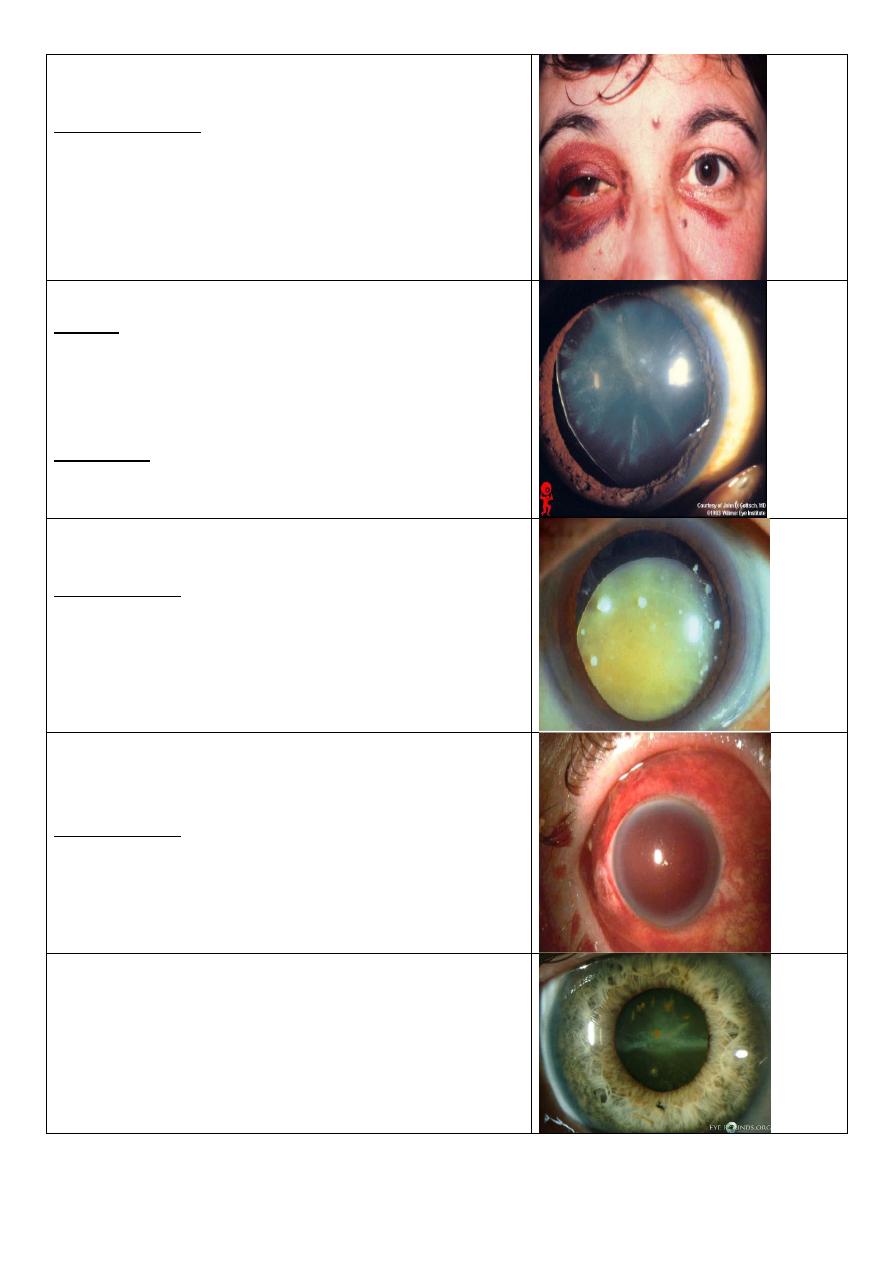
Scotoma
Area of blindness surrounded by area of vision due to
lesions in specific regions of retina.
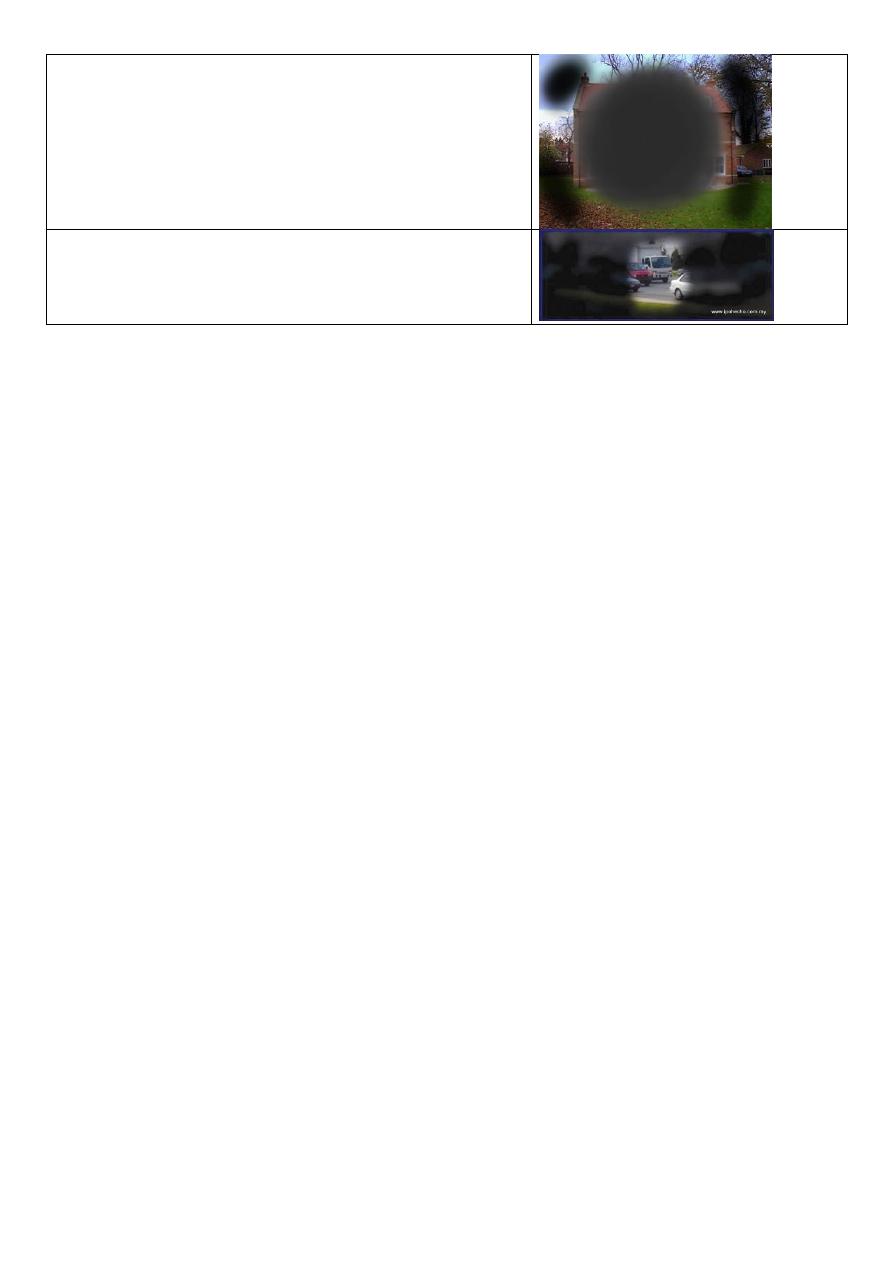
Tunnel vision
Only see the central part.