1
Fifth stage
Surgery-Ortho
Lec-2
د. هشام القطان
8/3/2016
Hip pain
Irritable hip
:
Pain and limping
D.D :
Septic arthritis.
Perthes.
Irritable hip (transient synovitis).
Slipped capital femoral epiphysis.
Brucellosis.
Tuberculosis.
Rheumatoid arthritis (single joint in children).
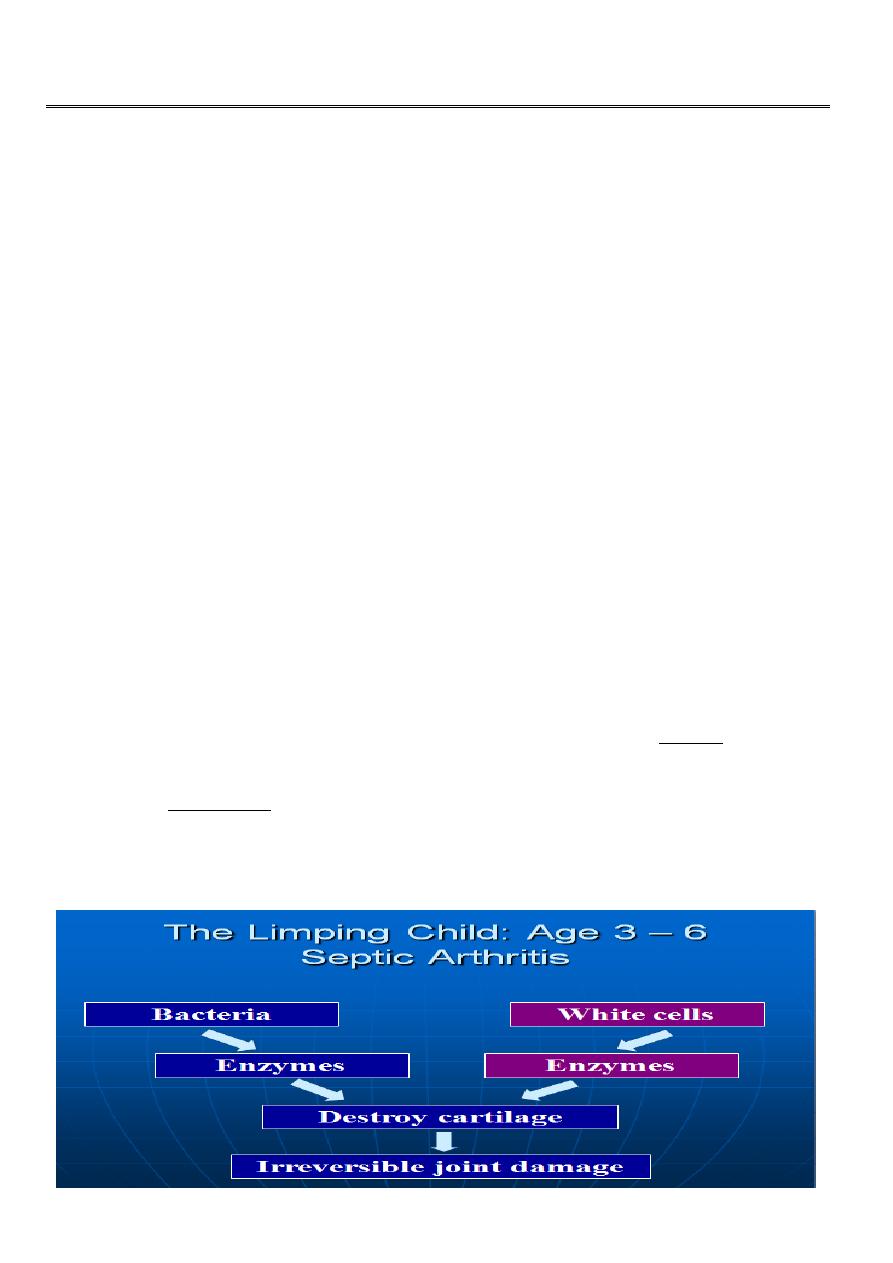
PYOGENIC ARTHRITIS :
seen in children under the age of 2 years.
The organism (usually a staphylococcus) reaches the joint either directly from a
distant focus
OR by local spread from osteomyelitis of the femur.
PATHOPHYSIOLOGY
2
Clinical features :
child is ill and in pain.
The affected limb may be held absolutely still and all attempts at moving the hip are
resisted. With care and patience.
it may be possible to localize a point of maximum tenderness over the hip;
Diagnosis
Confirmed by aspirating pus from the joint.
In neonates the most common presenting feature is a total lack of movement in the
affected limb (pseudo paralysis).
Local signs of inflammation are usually absent .
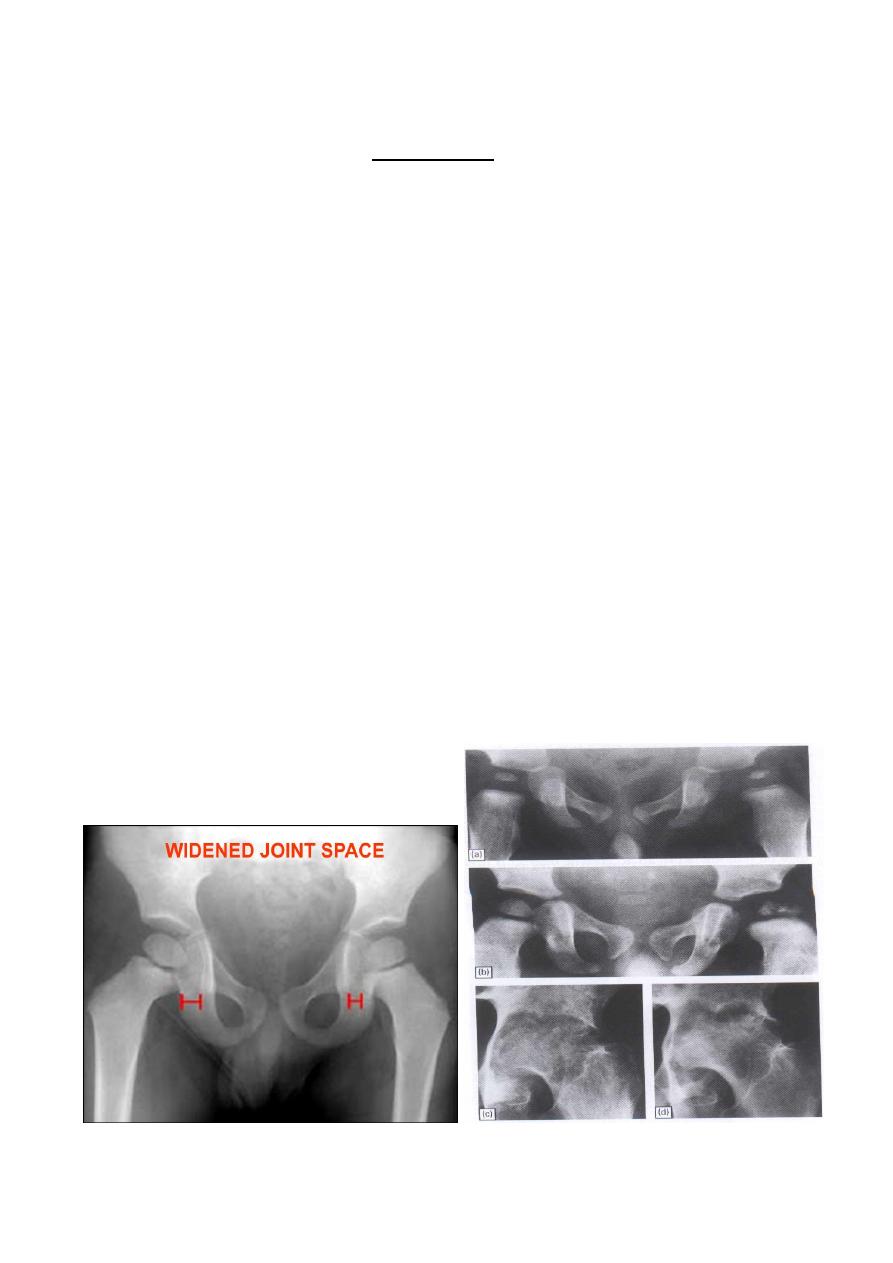
X-rays
During the acute stage of bone infection, x-rays may show
slight lateral displacement of the femoral head, suggesting the presence of a joint
effusion.
The Limping Child: Age 3 – 6
In children the epiphysis may become necrotic and later appear unusually dense or
'fragmented' on x-ray.

3
Ultrasound scans also will help to reveal a joint effusion.
Treatment
:
Antibiotics should be given as soon as the diagnosis is reasonably certain,
but not before obtaining a sample of joint fluid (or pus) for microbiological
investigation and testing for antibiotic sensitivity.
The joint is aspirated under general an aesthesia and.
if pus is withdrawn, arthrotomy is advisable.
antibiotics are instilled locally and the wound is closed without drainage.
The hip is kept on traction or splinted in abduction until all evidence of disease
activity has disappeared.
Legg Calve’ Perthes' disease (COXA PLANA )
Disorder of childhood characterized by necrosis of the femoral head.
Although the incidence is only 1 in 10 000.
Should always be considered in the differential Diagnosis of hip pain in young
children.
Patients are usually 4-8 years old and show delayed skeletal maturity.
Boys are affected four times as often as girls.

4
Pathogenesis :
femoral head may depend for its blood supply almost entirely on the lateral epiphyseal
vessels.
whose situation in the retinacula makes them susceptible to stretching and pressure from
an effusion.
Causes of avascular necrosis
of the femoral head :
1. Steroids
2. Infection
3. Perthes’ disease
4. Sickle cell disease
5. Hypothyroidism
6. Skeletal dysplasia – classically multiple epiphyseal dysplasia
Pathology
The pathological process takes 2-4 years to complete, passing through three stages.
Bone death.
revascularization and repair.
Distortion and remodelling.
Clinical feature :
The patient - usually a boy
of 4-8 years .
Complains of pain and
Starts to limp
.
The hip looks normal.
Although there may be a little wasting of the thigh.
Movements are diminished and their extremes painful.
later, abduction is nearly always limited and usually internal rotation.
5
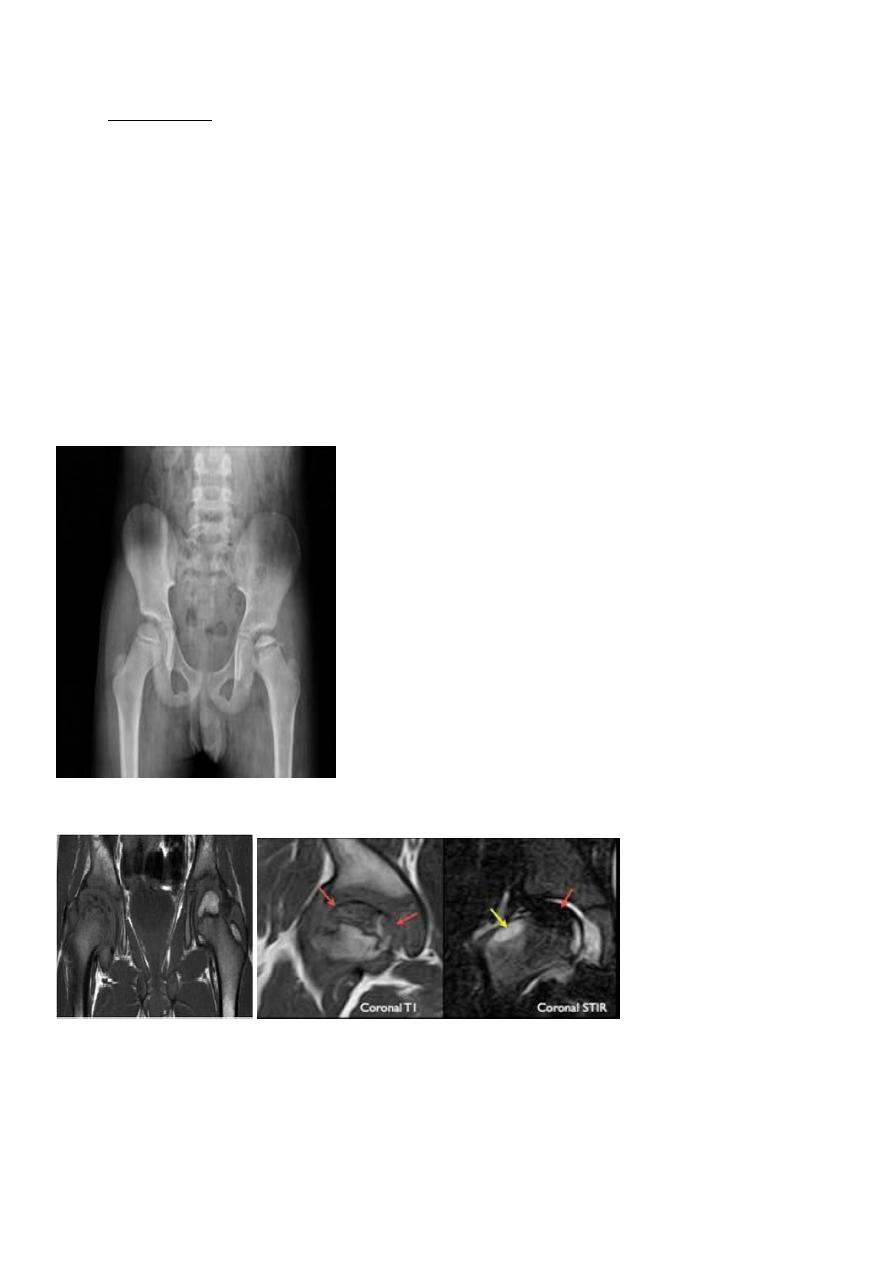
X-rays :
Before x-ray changes appear, the ischaemic area with decrease uptake ,can
sometimes be demonstrated as a 'void' on
radioisotope
scanning.
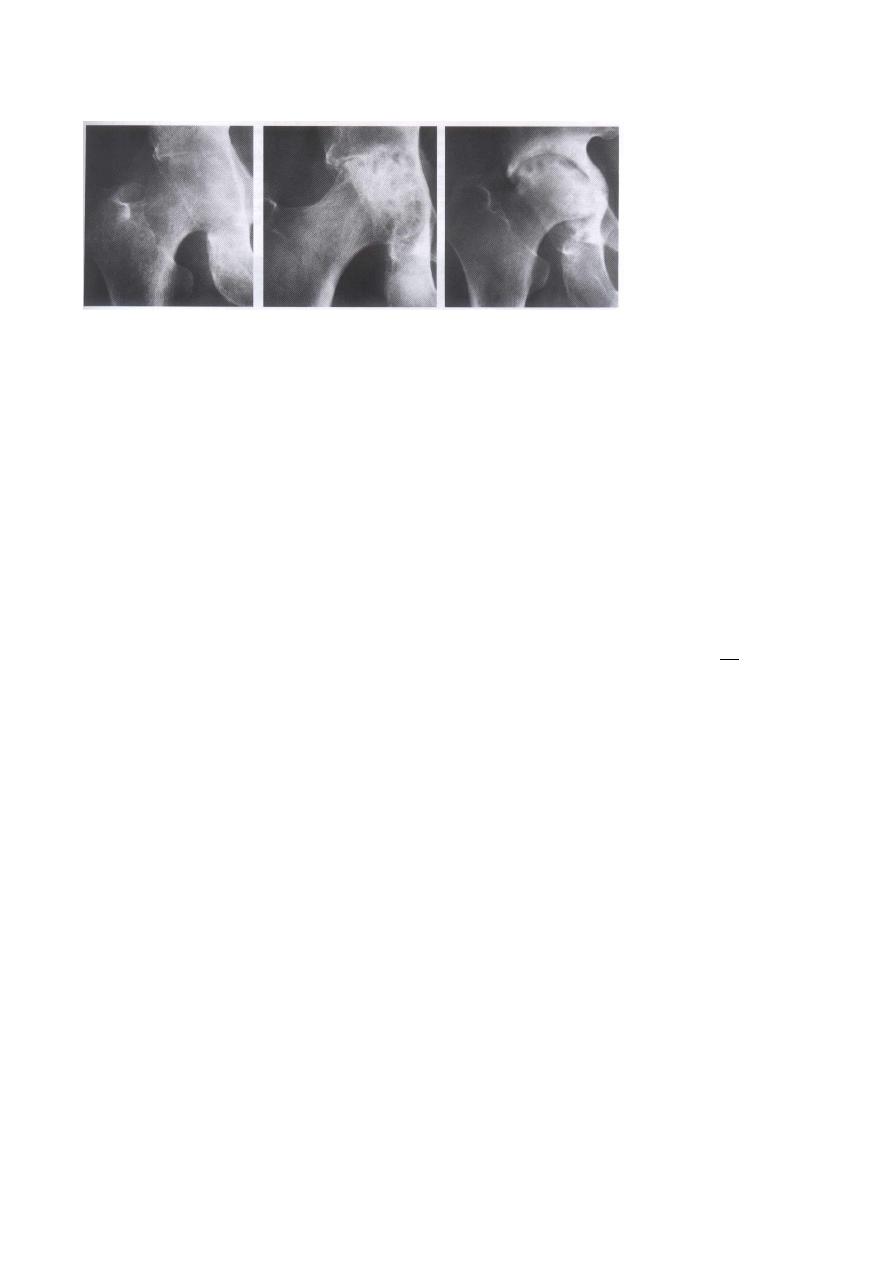
The earliest changes on X RAY:
are increased density of the bony epiphysis .
apparent widening of the joint space.
Flattening.
fragmentation .
lateral displacement of the epiphysis follow,
with rarefaction and broadening of the metaphysis.
MRI :
Differential diagnosis :
non-specific transient synovitis the so-called irritable hip.
Symptoms last for a week or two and clear up completely.
Ultrasound may show a joint effusion,

6
but the x-rays are always normal.
The child should be kept in bed until pain disappears and the effusion resolves.
Treatment :
As long as the hip is painful, the child should be in bed with skin traction applied to
the affected leg.
For about 3 weeks.
Then to follow up
it is essential that they attend periodically for radiological review .
Containment
This means keeping the femoral head well seated within the acetabulum. Surrounded
by its socket.
can be achieved by holding the hips widely abducted in plaster.
A removable splint until the bone changes have run their course (at least a year).
OR by performing a varus osteotomy of the femur.
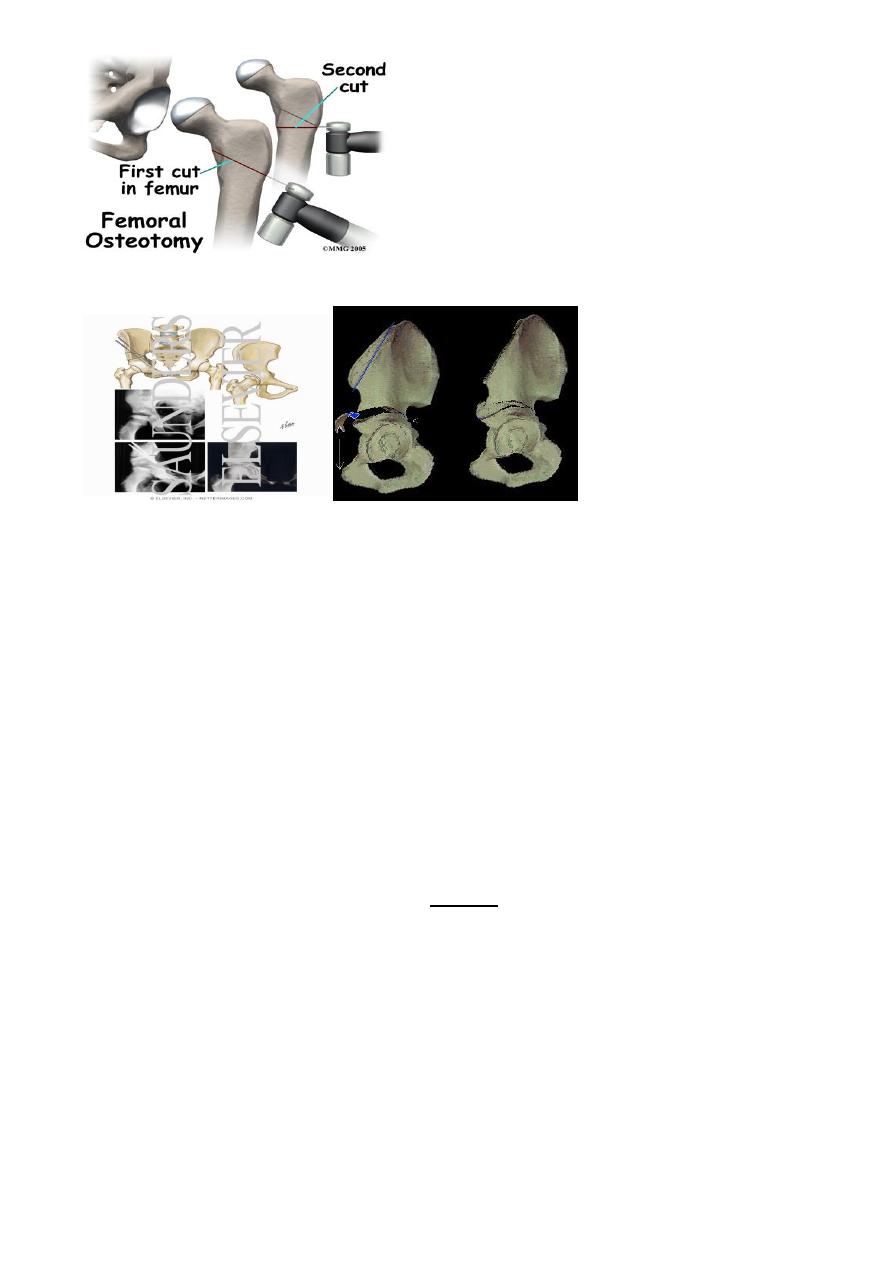
7
An innominate osteotomy of the pelvis.
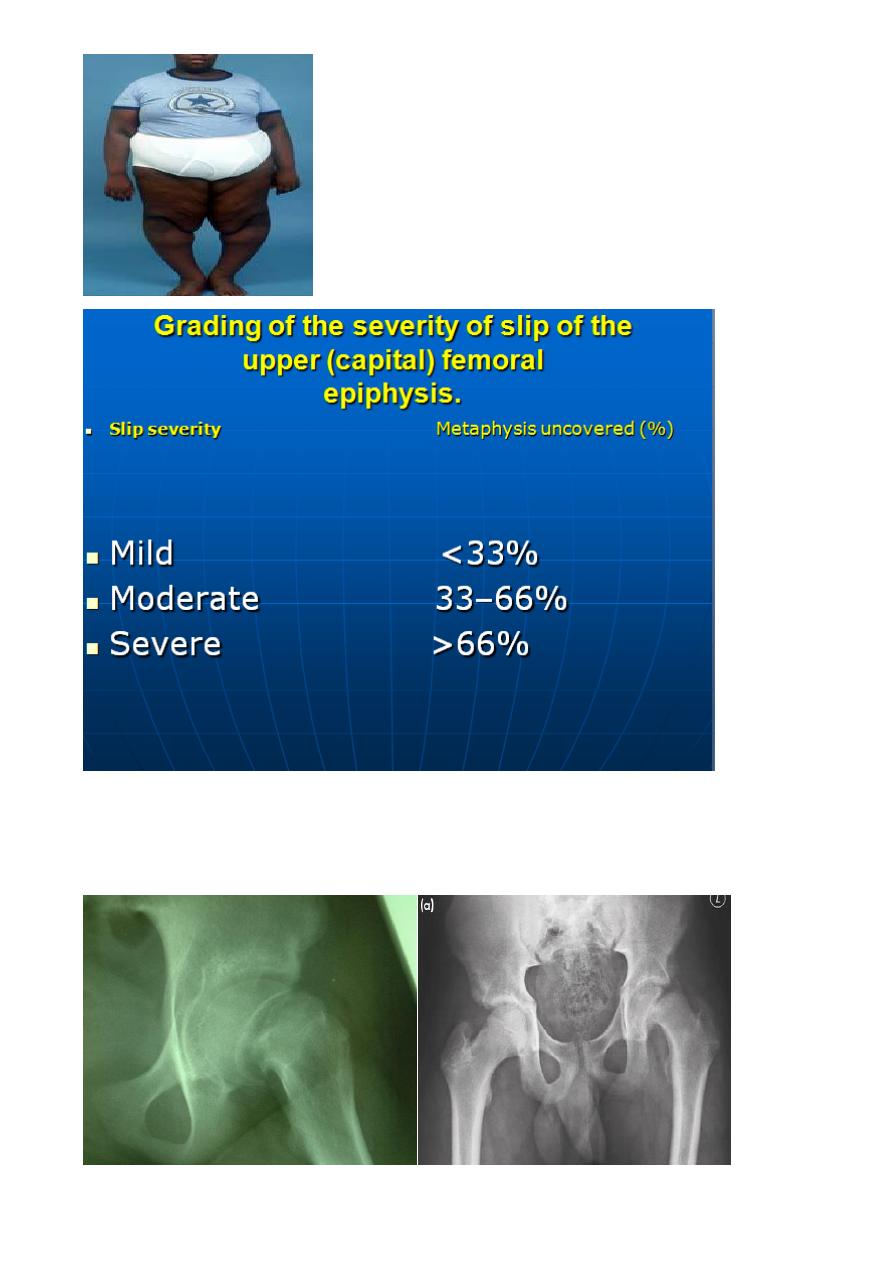
SLIPPED UPPER FEMORAL EPIPHYSIS
Incidence and aetiology :
Boys ate affected more often than girls.
Slip of the upper (capital) femoral epiphysis (SUFE or SCFE)
an incidence of 5:100 000 population.
the peak incidence is related to the start of puberty, hence it is earlier in girls.
Cause and pathology
A slipped epiphysis is an insufficiency fracture through the hypertrophic zone of
the cartilaginous growth plate.
Normal forces, exacerbated by
obesity with delayed gonadal development.
and repetitive minor trauma, precipitate a slip.
Puberty.
Tall children .

8
Clinical features :
The patient - usually a boy of 14 or 15 years .
presents with pain in the groin, the anterior part of the thigh or the knee (referred
pain).
he may also limp.
The onset may be sudden and in 30 per cent there is a history of trauma (acute slip').
However, in the majority ..
symptoms are chronic I.e.
chronic slip,
or else a long period of pain may culminate in a sudden climax following minor
trauma .
acute-on chronic slip.
On examination :
the leg is externally rotated and is 1 or 2 cm short.
Characteristically there is limitation of abduction and medial (internal) rotation.
Following an acute slip, the hip is irritable and all movements are accompanied by
pain.
Hip Flexion Causes Abduction & External Rotation
OR SCFE :
Associations with , Obesity
Endocrine issues
Hypothyroidism
9
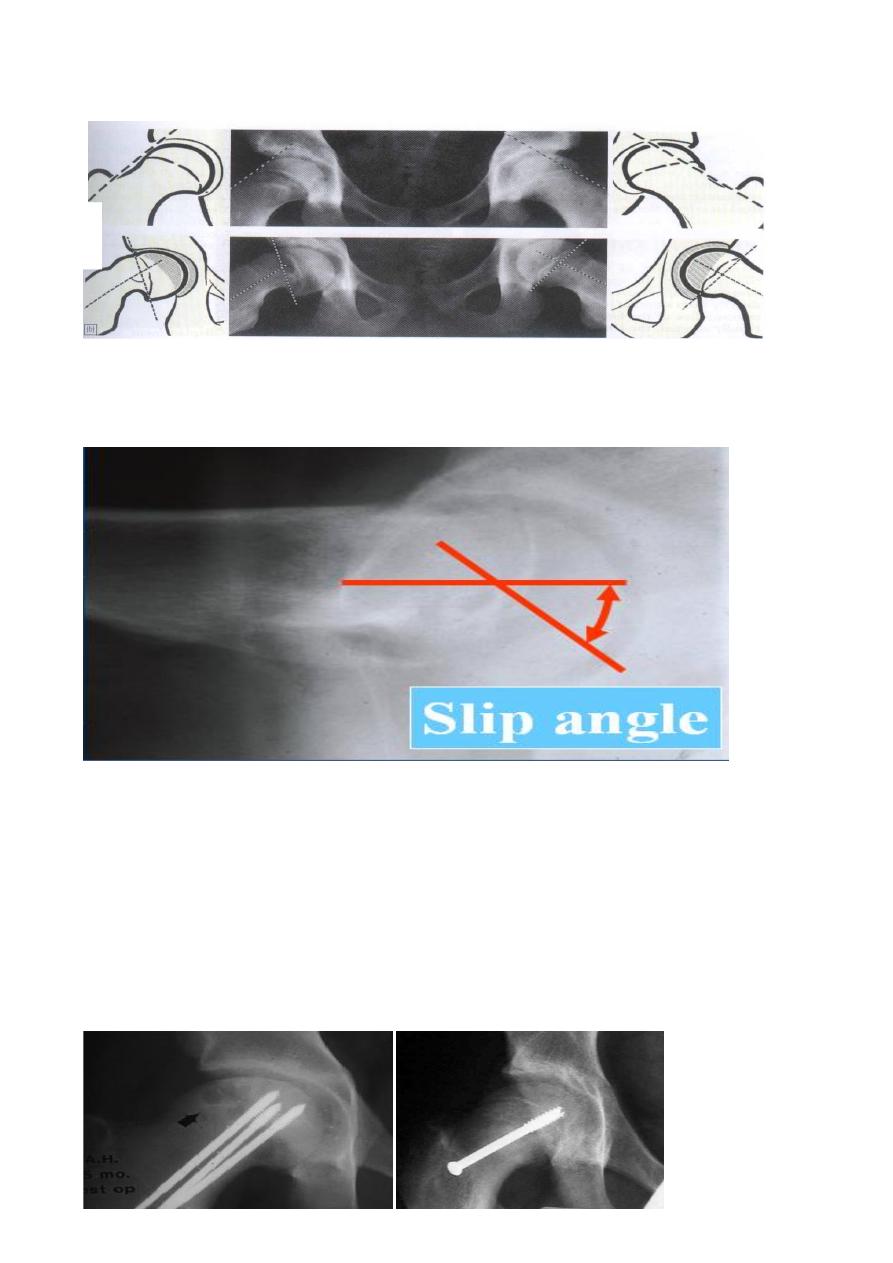
X-rays :
In the anteroposterior view the epiphyseal plate seems to be too wide and too
'woolly'.
10
Trethowan's sign A line drawn along the superior surface of the neck remains
superior to the head instead of passing through it .
In the lateral view the femoral epiphysis is tilted backwards; small degrees of tilt
can be detected by measuring the angle between the epiphyseal base and the
femoral neck .
Treatment :
Manipulation is dangerous and should be avoided.
Minor displacement
Displacement of less than one-third the width of the epiphysis is treated by accepting
the position and fixing the epiphysis with two thin threaded pins or screws. This is
always done under x-ray control.
fixation in position

11
Severe displacement
If the displacement is more than half the epiphyseal width, corrective surgery will be
needed.
TUBERCULOSIS :
The disease may start as a synovitis, or as an osteomyelitis in one of the adjacent
bones.
Once arthritis develops, destruction is rapid and may result in pathological
dislocation.
Healing usually leaves a fibrous ankylosis with considerable limb shortening and
deformity.
Clinical features
Pain in the hip is the usual presenting symptom,
The patient walks with a limp;
though in late, neglected cases a cold abscess may point in the thigh or buttock.
muscle wasting may be obvious and
joint movements are limited and painful.
Investigations :
1.
Blood examination … E S R.
2.
Mantoux test
3. ELAIZA TEST .
X-rays :
The first x-ray change is general rarefaction of bone around the hip,
In a child, the femoral epiphysis may be enlarged, again suggestive of chronic
synovitis.
12
Later changes are erosion and eventually destruction of the articular surfaces on
both sides of the joint.
Complications :
However, if the joint is destroyed, the usual result is an unsound fibrous ankylosis.
The leg is scarred and thin.
and shortening is likely to be severe.
Treatment
If the disease is caught early, anti-tuberculosis chemotherapy should result in
healing.
During the acute phase, the joint may need to be splinted in abduction or held in
traction until the symptoms subside.
An abscess in the femoral neck is best evacuated.
If the joint has been destroyed, arthrodesis may become necessary, but usually nor
before the age of 14.
In adults joint replacement is feasible