
1
Fifth stage
Gynecology
Lec-4
.د
ولدان
16/3/2016
Infections in gynecology
Objectives:
• Know the causes of genital tract infections.
• Know the mangement of genital tract infections.
• Know which infections are sexually transmitted.
• Know the sequale of sexaully trasmitted disease(STD).
Physiological discharge:
• Normal vaginal discharge is white, becoming yellowish on contact with air.
• It consists of desquamated epithelial cells from the vagina and cervix, mucus
originating mainly from the cervical glands. bacteria and fluid, which is formed as a
transuedate from the vaginal wall. More than 95 per cent of the bacteria present are
lactobacilli.
• The acidic pH is maintained by the lactobacilli and through the production of lactic acid.
• It increases due to increased mucus production from the cervix in mid-cycle,
pregnancy and sometimes when women begin using a combined oral contraceptive
pill.
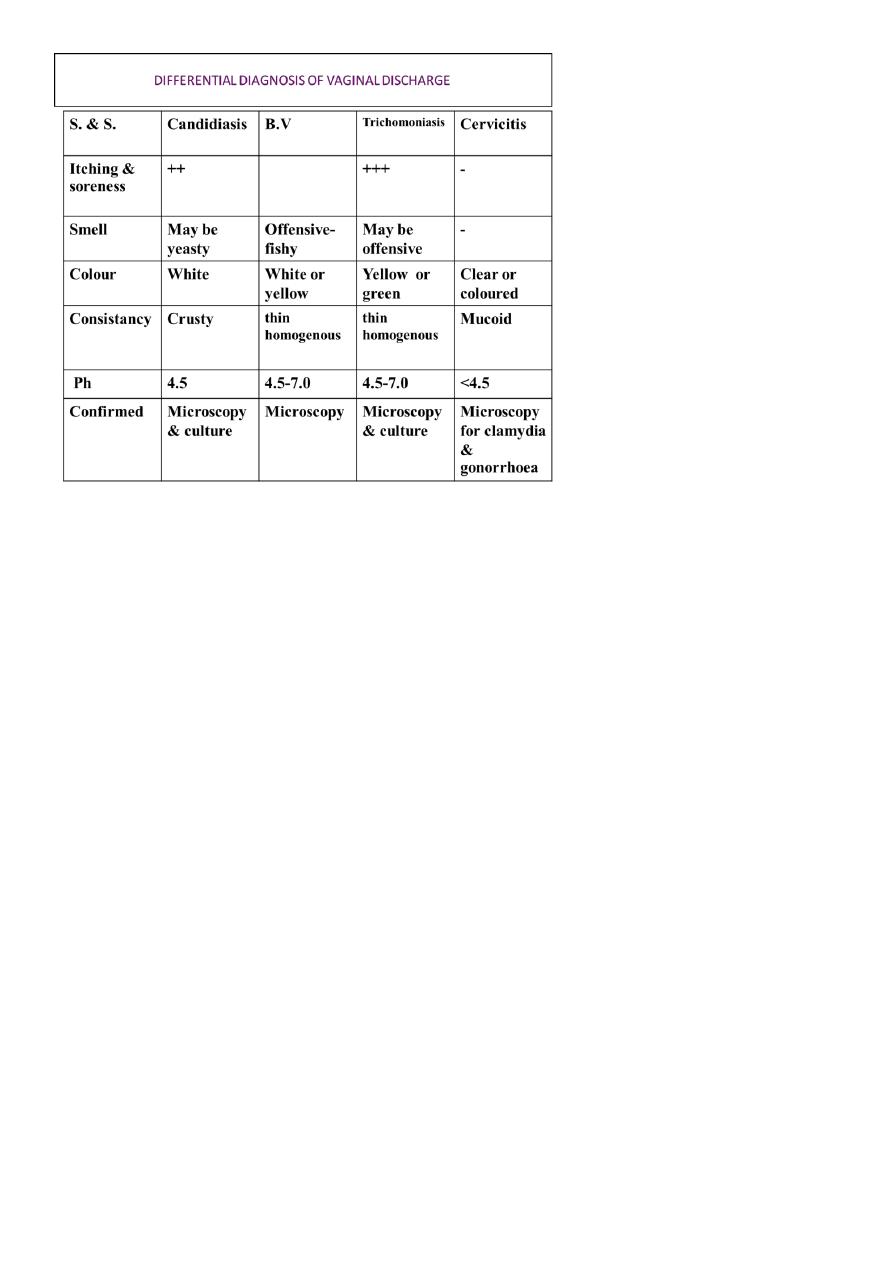
Lower genital tract infections:
• Vaginal discharge can originate from anywhere in the upper or lower genital tract.
• Discharge arising from the vagina itself can be physiological or due to bacterial
vaginosis (BV), candidiasis or Trichomonas infection.
Vulvovaginal Candidiasis: (vvc)
• An estimated 75% of women experience at least one episode of this infection.
• It is a common condition.
• It is a mycotic disease, caused by the dimorphic yeast candida albicans, a commensally
of the genital & digestive system.
• It is not a STD.
2
Predisposing facters:
• Broad-spectrum antibiotic therapy.
• Pregnancy.
• Diabetes mellitus.
• Immunosuppression.
• HIV.
• Steroids.
• Vaginal douching, tight clothing.
• Combined oral contraceptive pill.
Diagnosis:
• The symptoms of VVC consist of vulvar pruritis associated with a vaginal discharge that
typically resembles cottage cheese.
• The discharge can vary from watery to homogeneously thick.
• Examination reveals erythema and edema of the labia and vulvar skin.
• Discrete pustulopapular peripheral lesions may be present.
• The vagina may be erythematous with an adherent, whitish discharge.
• The cervix appears normal.
• The pH of the vagina in patients with VVC is usually normal (<4.5).
• The classical presentation is with itching and soreness of the vagina and vulva, with a
curdy, white discharge, which may smell yeasty, but in some cases there may be itching
and redness with a thin, watery discharge.
• Microscopy and culture of the vaginal fluid can confirm a diagnosis.
• Asymptomatic women from whom Candida is grown on culture do not require
treatment.
Treatment:
• Topically applied azole drugs are the most commonly available treatment for VVC and
are more effective than nystatin.
• Symptoms usually resolve in 2 to 3 days. An oral antifungal agent, fluconazole, used in
a single 150-mg dose.

3
• It appears to have equal efficacy when compared with topical azoles in the treatment
of mild to moderate VVC.
• Women with complicated VVC benefit from an additional 150-mg dose of fluconazole
given 72 hours after the first dose.
• Patients with complications also can be treated with a more prolonged topical regimen
lasting 10 to 14 days.
• Adjunctive treatment with a weak topical steroid, such as 1% hydrocortisone cream,
may be helpful in relieving some of the external irritative symptoms.
Recurrent Vulvovaginal Candidiasis:
• A small number of women develop recurrent VVC (RVVC), defined as four or more
episodes in a year.
• These women experience persistent irritative symptoms of the vestibule and vulva.
Burning replaces itching as the prominent symptom in patients with RVVC.
• The diagnosis should be confirmed by direct microscopy of the vaginal secretions and
by culture. Many of these patients have chronic atopic dermatitis or atrophic
vulvovaginitis
• The treatment of patients with RVVC consists of inducing a remission of chronic
symptoms with fluconazole (150 mg every 3 days for 3 doses).
• Patients should then be maintained on a suppressive dose of this agent (fluconazole,
150 mg weekly) for 6 months. On this regimen, 90% of women with RVVC will remain
in remission.
• After suppressive therapy, approximately one half will remain asymptomatic.
• Recurrence will occur in the other half and should prompt reinstitution of suppressive
therapy.

4
Bacterial vaginosis:
• Its the commonest cause of abnormal vaginal discharge in women of child bearing age.
• It is not a STD.
• Its aetiology is unknown.
• It is characterized by an overgrowth of an anaerobic organism like (Gardnerella vaginalis
and Mycoplasma hominis) in the vagina, this leads to replacement of lactobacilli (usually
absent) and an increase in PH from a normal 4.5 to 7.
• 50% are a symptomatic .
• Symptomatic patient has offensive, fishy-smelling
vaginal discharge particularly noticeable around the time of menstruation or following
intercourse.
• Vaginal secretions are gray and thinly coat the vaginal walls.
• The vagina is usually not erythematous, and cervical examination reveals no
abnormalities.
Risk Factors:
• Douching.
• Black race.
• Cigarette smoking.
• Intrauterine device.
• Early age of sexual intercourse.
Diagnosis:
Amsel's criteria for diagnosis of bacterial vaginosis in which at least three out of four should
be present and these are:
• thin, gray, homogenous discharge.
• Clue cell on microscope ( vaginal epithelial cells so heavily coated with bacteria that
the border is obscured).
• PH of vagina> 4.5(usually between 4.7-5.7).
• The addition of KOH to the vaginal secretions (the “whiff” test) releases a fishy, amine
like odor.

5
BV can also be diagnosed from Gram-stained vaginal smear, large number of Gram-positive
& gram-negative cocci are seen with reduced or absent large Gram-positive bacilli (
Lactobacilli).
BV associated with significant adverse sequelae:
• increased risk for pelvic inflammatory disease (PID).
• postoperative cuff infections after hysterectomy.
• abnormal cervical cytology .
Pregnant women with BV are at risk for:
• late miscariage.
• Postabortal PID.
• premature rupture of the membranes.
• preterm labor and delivery.
• chorioamnionitis.
• Postpartum-endometritis.
In women with BV who are undergoing surgical abortion or hysterectomy,
perioperative treatment with metronidazole eliminates this increased risk .
Treatment:
• avoid vaginal douching and use of antiseptic bath agents.
• recommended regimen is:
• Metronidazole 500 mg orally twice daily for 7 days or single dose 2g.
• Metronidazole gel 0.75% 5 g intravaginally once daily for 5 days.
• Clindamycin cream 2% 5 g intravaginally at bedtime for 5 days.
Pregnancy and bacterial vaginosis:
All symptomatic pregnant women with bacterial vaginosis should be treated, also
asymptomatic pregnant women with previous history of preterm birth or second trimester
loss may be screened and treated.

6
Trichomoniasis:
• STD.
• Trichomonas vaginalis found in the vagina, urethra, and paraurethral gland.
• It can be acquired perinatally in 5% of babies to infected mother.
This sexually transmissible infection can be carried asymptomatically, it can be carried in
toilet articles from women to another, cross-infection in antenatal & gynecological clinics
may occur. In men is carried asymptomatically but may present as non- gonococcal urethritis.
In women it causes vulvo vaginitis with purulent offensive yellow frothy discharge with
irritation & soreness but in few cases the discharge is less. The onset is sudden & there
may be history of previous attacks, this infection usually seen during pregnancy.
Examination show yellow or green vaginal discharge which has an un pleasant odors with
inflammation of vulva, urethra & adjacent skin .
The vaginal wall is intensively red & inflamed & numerous minute punctate hemorrhages
can occur on the vagina & cervix as strawberry spots.
It is confirmed by culture in specific media. Microscopy of vaginal discharge mixed with
saline has 60% sensitivity to detect the pear-shaped protozoon that can be recognized by
its high motility with numerous leucocytes.
• 10% - 50% asymptomatic
• Vaginal discharge, vulval itching, dysuria, and offensive odor
• 70% have vaginal discharge, vary from thin and scanty to profuse and thick
• 10 - 30% has classical frothy yellow vaginal secretion
• Vulvitis, vaginitis; and cervicitis
• 2% has visible strawberry cervix
• 10-15% no abnormalities
• In pregnancy increase incidence of preterm labour and IUGR
Treatment:
• Systemic treatment is recommended and the regimen used is metronidazole 2 g in a
single dose or 400 mg twice daily for 5-7 days.
• The partner should be screened and treated.
• In pregnancy, metronidazole is contraindicated in the first trimester, so local
treatment can be used like clotrimazole 100 mg daily for 7 days.
7
Vaginal discharge in children:
• Common condition.
• Streptococcal infection is the commonest cause.
• Recurrent infection may be due to foreign body.
• Entrobius vermicularis migrate from anus at night and cause itching and irritation.
• Sexual abuse.
Other conditions affecting the vagina:
Atrophic vaginitis:
• is common in post menopausal women in whom vaginal epithelium atrophies &
lactobacilli replaced by skin commensal organisms lead to superficial dyspareunia and
vaginal soreness.
• treatment is with estrogen replacement.
• Occasionally a true bacterial vaginitis is encountered due to streptococci or other
organism.
Bartholine abcess:
• Bartholin's gland situated on either side of the vagina, opening in the vestibule.
• Bartholin's cyst can present as painless swelling if gland duct opening become blocked.

8
• If infected a bartholin abcess develops and present as hot, tender mass near lower
part of vagina.
• Need surgical treatment by marsupialization.
• Culture should be sent.
Toxic shock syndrome:
is a rare condition associated with retention of tampons or foreign bodies in the vagina lead
to over growth of staphylococci producing a toxin causing systemic shock , fever, diarrhea,
vomiting & rash.
Infestations:
Pubic lice and scabies are transmitted by close bodily contact.
Pelvic inflamatory disease: (PID)
• is broad term used to cover upper genital tract infection i.e. endometritis, parametitis,
salpinigitis & oophoritis. These infections usually spread from-vagina or cervix through
uterine cavity, lymphatic spread may occur parametrically or along the surface of the
uterus. It may be spread from the bowel or blood born.
Infection may be from the bowel or can be blood borne 80% of cases is triggered by
transmissible infection either chalmydia or gonohoea.
Endogenous anaerobes as bacteriodes spp., or mycoplasma hominis usually came in as
secondary invaders & cause tubal abscess. PID is important condition because it result in
tubal damage leading to ectopic pregnancy & tubal factor infertility, 20% of women left with
chronic pelvic pain.
Etiology:
• Neisseria gonorrhoeae and Chlamydia trachomatis are the most important m.o.,
although gardnerella vaginalis, anaerobes and others like mycoplasma may be
implicated and responsible for subsequent abscess formation.

9
Pathology:
• First stage of salpingitis is mucosal Inflammation with swelling, redness and deciliation.
• Submucosal invasion with polymorph nuclear cell, mononuclear and plasma cell.
• Inflammatory exudates fills the lumen.
• Inflammation extends to the serosal surface, and pus exudes from the fimbriae to the
ovaries and adnexia.
• Omentum usually confines the infection to the pelvis, however, infection may cause
tissue damage end with tubo-ovarian abscess .
• Subsequent scarring made the fimbrial end adherent to the tube and sealing the end of
the tubes .
• The-uterus fixed by adhesion and becomes retroverted.
• Hydrosalpinx, and if infected pyosalpinx results .
Factor associated with PID
• Young age < 25 years.
• Multiple sexual partners.
• Past history of STD.
• Termination of pregnancy.
• Insertion of IUCD in the past 6 months.
• Hysterosalpingography (HSG).
• In vitrofertilization.
• Postpartum endometritis.
• Bacterial vaginosis.
• Smoking.
Symptoms suggestive of PID
• Lower abdominal pain.
• Deep dyspareunia.
• Irregular vaginal bleeding.
• abnormal vaginal discharge.

10
• Pyrexia may be present.
• Dysmenorrhea.
• Dysuria. In acute sever infection fever, nausea, and vomiting.
Bimanual examination
• Lower abdominal and adnexal tenderness.
• Cervical excitation.
• Adnexal mass in 20%.
Diffrential diagnosis:
• Ectopic pregnancy.
• Acute appendicitis.
• Endometriosis.
• Complicated ovarian cyst.
• Constipation.
Infestigations:
• High vaginal swab for tricomonas and vaginosis and endocervical swab for gonorrhea
and Chlamydia.
• ESR and c-reactive protein is elevated.
• Laparoscopy: done if clinical diagnosis is uncertain. in mild cases the tubes are swollen
and red. In sever cases the tubes adherent to the adjacent structures. In pelvic
peritonitis, all the organs are congested and adhesion cause inflammatory abscess.
• Ultrasound.
Management:
• Rest.
• Pregnancy test.
• Appropriate analgesia.
• Avoid sexual intercourse until both of them treated.
11
• Inpatient management in those with:
Sever condition
Failure of oral treatment
Suspicions of tubo-ovarian abscess
Those with immunodeficiency problem
Pregnant women (PID can occur up to 12 weeks
Outpatient:
• Oral ofloxacine 400mg bd + oral metronidazole 400 mg bd daily for 14 days or
• IM ceftriaxone 500 mg + oral doxycycline 100 mg bd 14 days + oral metronidazole 400
mg bd 14 days.
Inpatient:
• I.V. ceftriaxone 2g od + I.V. doxycycline 100mg bd followed by oral doxycycline 100mg
bd 14 days + oral metronidazole 400mg bd for 14 days.
• Drainage of abscess is indicated if i.v. treatment failed after 24-48 hours.
• Intra-abdominal spread of infection of Chlamydia and gonorrhoeae can cause
perihepatitis, which is called Fitz-Hugh Curtis syndrome (adhesion between liver and
peritoneal surface appear at laproscopy as typical violin string appearance).
Consequences of pelvic infection:-
• Recurrence:- 25% of patient of patient will have recurrence , the damaged tubal
epithelium will have subsequent invasion by organisms.
• Pain: long term pain occurs in 15-20% of patients with dysmenorrhea & dyspareunia.
• Infertility PID is the most common & preventable cause of infertility pelvic damage is
usually irreversible .
• Ectopic pregnancy : the ratio of ectopic pregnancy & PID is high due to tubal damage
.