1
Fifth stage
ENT
Lec-15
د.سعد
24/3/2016
Physiology of Hearing
Sound travels in air at 340 m/sec at 20C° and atmospheric pressure. Sound has two subjective
physical properties; frequency (pitch) and intensity (loudness). The frequency is measured by
hertz (Hz) [Hz = Cycle/sec], whereas the decibel (dB) is the unit of intensity.
The purpose of the auditory apparatus is to convert vibrations in air to vibrations in the inner-ear
fluids, and then to nerve impulses to be transmitted along the auditory nerve to the higher centers
of hearing.
The ratio of the functioning area of the tympanic membrane to the foot plate is 14:1. This is
combined with an ossicular lever ratio of 1.3:1. The product of these (14X1.3= 18:1) which
represent the transformer mechanism.
Physiology of the Vestibular Apparatus
The balance of the body is maintained by coordination of information from three systems:
1. Proprioception, i.e. sensation from muscles, joints, tendons and ligaments.
2. The eyes.
3. The vestibular system.
The vestibular system consists of the semicircular canals, the utricle and the saccule. The utricle
and the saccule respond to linear acceleration. Impulses from the utricle and saccule give
information about the position of the head in space and initiate reflexes which tend to keep the
head in upright position and are contributory to maintenance of muscle tonus.
The semicircular canals respond to angular (rotatory) acceleration, and stimulation of the
semicircular canals gives rise to the sensation of rotation and to reflex movement of the eyes
and body to counter the movement.
2
Symptoms of ear disease
1.
Hearing loss;
Is defined as subjective impairment of hearing. It is either conductive, sensorineural or mixed.
Conductive hearing loss (CHL) results from failure of conductive mechanism to transmit the sound
impulse from the external ear to the inner ear fluid, and it may be due to diseases of the external
auditory meatus, tympanic membrane, the middle ear cavity or ossicles. Sensorineural hearing loss
(SNHL) can be a result of diseases of the cochlea or its neural connection.
In CHL the sound appears quieter but it is not distorted. Sound and speech are well heard when
amplified. In some cases the patient may hear better in the presence of background noise e.g. railway
carriage or motor car. This is called paracusis Willisii and it is found most typically in otosclerosis.
Paracusis probably results from the simple fact that in these places people with normal hearing
automatically raise their voice to overcome the background noise. The otosclerotics are unable to
hear the lower tones that present in the back ground noise. The quality of speech is well maintained
because the patient hears his own voice clearly.
In SNHL the sound not only seems quieter but it is distorted as in majority of cases the higher
frequencies are more affected than the lower, leading to difficulty in hearing the consonant sounds
which are so important for speech discrimination. In severe SNHL the patient does not hear his own
voice and leads to speech which is indistinct or expressionless.
2. Discharge;
Serous or purulent discharge; Otitis externa.
Mucopurulent discharge; Otitis media.
Sensorineural Hearing Loss
Conductive Hearing Loss
Sound appears quieter and distorted.
Sound appears quieter but it
is not distorted.
1.
Sounds` distortion limits the benefit
of amplification.
Sounds are well heard when
amplified.
2.
Paracusis Willisii negative.
Paracusis Willisii positive
3.
In severe cases the speech becomes
indistinct and expressionless because
the patient does not hear his own
voice.
The quality of speech is well
maintained.
4.

3
Watery discharge; CSF otorrhea following head injury or aural surgery. It occurs as a result
of damage to tegmen tympani.
Bloody discharge; due to granulation tissue in chronic suppurative otitis media or due to
malignant disease.
3. Pain (Otalgia);
It arises within the ear (otogenic or primary) or out side the ear (non- otogenic or referred
otalgia).Referred otalgia, commonly referred to the ear from lesions of related structures whose
nerve supply also send branches to the ear. The ear receives sensory nerve supply from the
trigeminal (V), glossopharyngeal (IX) and vagus(X) nerves as well as from branches of the upper
cervical roots especially C2 and C3. Ear pain can be referred pain to the ears in the following
ways:
1.
V
cranial nerve; diseases of the lower molars, e.g. pulp space infections and impacted
unerupted teeth, especially wisdom teeth. Otalgia may also follow dental extraction. The
temporomandibular joint (TMJ) is a common source of otalgia.
2.
IX
(Jacobson) and
X
(Arnold) nerves; pharyngeal cause of otalgia include acute tonsillitis,
tonsillectomy, ulcers in the mouth, tongue and pharynx, malignant disease of the
nasopharynx, pharynx, and hypopharynx. Glossopharyngeal neuralgia is a primary
neuralgia causing intermittent agonizing paroxysms of pain affecting the base of the
tongue, the fauces and the ear.
3. 2nd and 3rd cervical spine nerves (lesser occipital and greater auricular): intervertebral
disc disease and cervical spondylosis
4. Itching:
Is generally associated with otitis externa. Also it may arise from discomfort of wax.
5. Tinnitus:
Is a subjective sensation of sound in the ear or head in the absence of any relevant external
signals. (Occasionally it is objective e.g. in palatal myoclonus and glomus tumors). It is regarded
as a sign of irritation of the cochlea or upper auditory pathways. Tinnitus may be met with any
form of ear disease, and is also a symptom of some general diseases which indirectly affect the
ear through the circulation. It is a common symptom of renal disease, cardiac disease,
intracranial tumors and anaemia, and it may be caused by certain drugs, such as quinine, the
salicylates and ototoxic antibiotics.
4
6. Vertigo:
Is defined as hallucination of movement or subjective sense of imbalance. It can be due to CVS
disease, CNS disease or ear disease. Vertigo is considered as a symptom of irritation of the
vestibular apparatus.
Assessment of Hearing
While assessing the auditory function it is important to find out:
1. Type of hearing loss ( CHL, SNHL or mixed )
2. Degree of hearing loss.
3. Site of lesion.
4. Cause of hearing loss.
A. Clinical tests of hearing:
1. Finger friction test; rubbing the thumb and finger close to the ear.
2. Watch test; A clicking watch is brought close to the ear and the distance at which it
is heard is measured.
3. Speech ( voice ) test; A person with normal hearing can hear conversation voice
with the opposite ear occluded in a quite room from a distance of 6 meters.
4. Tuning fork tests:
The tuning fork (TF) used should have a frequency of 512 Hz. The note of the
higher frequency forks tends to decay quickly where as the lower frequency forks induce
perception by vibration sensation.
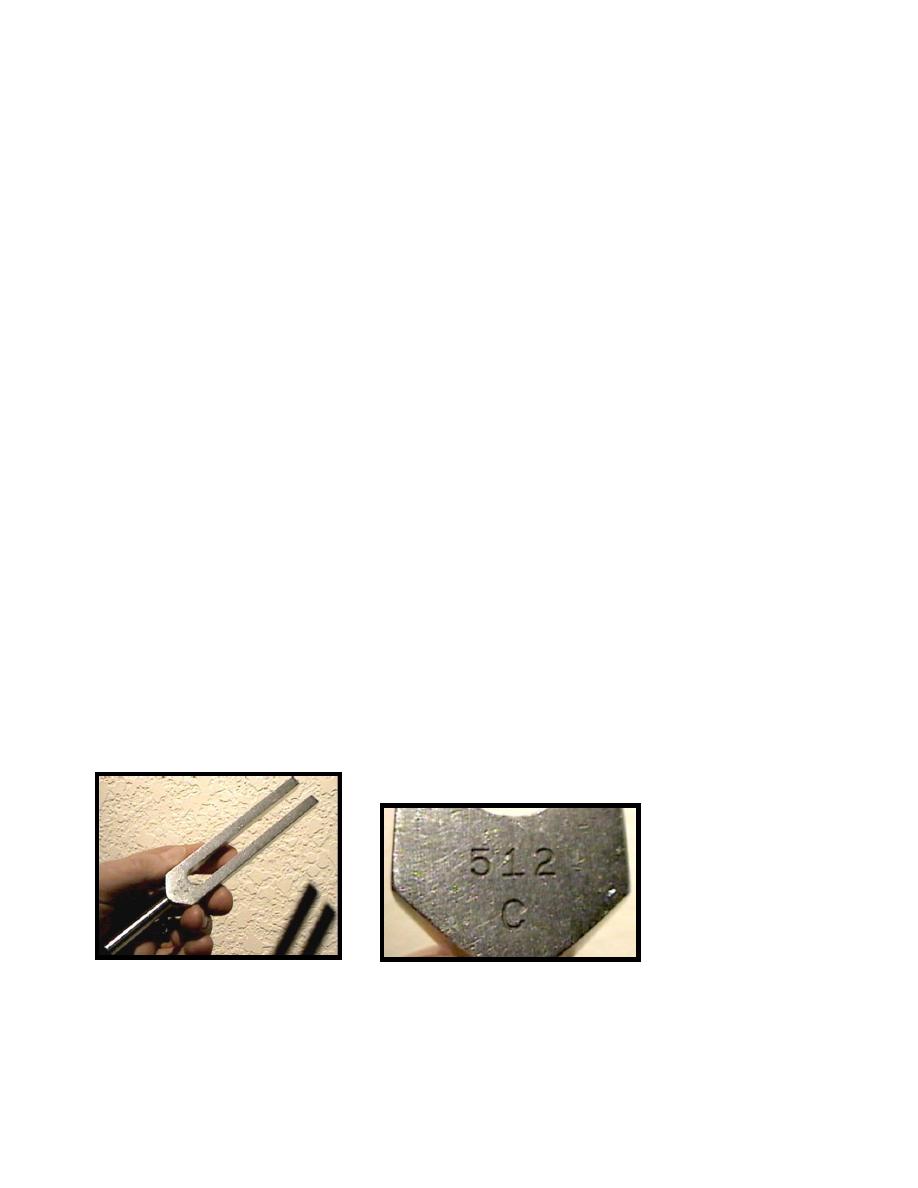
Rinne`s test; The TF is struck against resilient surface and then held so that the acoustic axis
is in line with the EAM. In this way the sound of the TF is heard by air conduction (AC). Bone
5
conduction (BC) is heard by holding the TF with its base placed firmly against the mastoid
bone. Here the sound is transmitted through the bones of the skull to the cochlea.
Therefore, this test compare air and bone conductions in the same ear. More correctly,
the test is done by requiring the subject to indicate as soon as the fork becomes inaudible
by bone conduction then quickly transferring it close to the EAM. If it is then audible, the
AC is said to be better than BC. If not then the BC is better than AC.
Normal subject = AC > BC (
Rinne
+ve)
CHL = BC > AC (
Rinne
-ve)
SNHL = AC > BC(
Rinne
+ve) and often the BC is not heard.
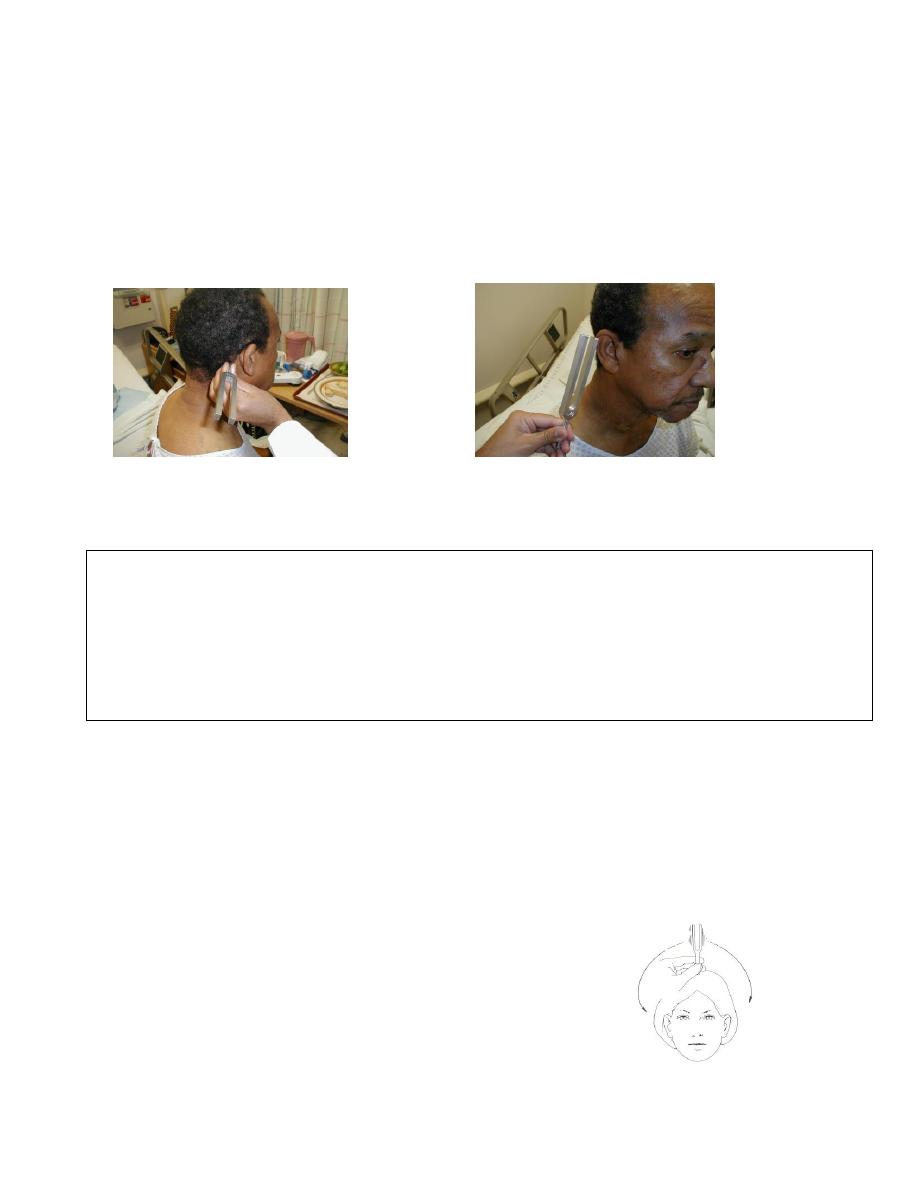
Weber test; This test compares the BC
of the two ears. The TF is set in vibration
and applied to the vertex of the skull in
the midline and the patient is asked in
which ear he hears the sound.
6
In normal subjects the sound is heard in the midline or in both ears equally.
In CHL the sound is heard in the affected ear due to the absence of environmental noise.
In SNHL the sound is heard in the non-affected ears.
False negative Rinne; In unilateral severe SNHL, Rinne`s test will appear to give a
negative result. AC is absent but BC may be good because the sound is transmitted to
the opposite cochlea through the skull. This result may confuse the examiner in making
a wrong diagnosis of CHL. In this situation Weber test is important (if it is CHL, the TF
should be heard in the deaf ear). This condition can be overcome by applying a Barany`s
noise box to the non-test ear. It is a clock work device which emits white noise (wide
frequency) and raises the threshold of hearing in the non –test ear to such a level that
the TF can not be heard in that ear by cross hearing. It will then be found that the patient
is unable to hear the TF by either AC or BC.
B. Audiometric tests:
1. Pure Tone Audiometry
An audiometer is a device which produces pure tone, the
intensity of which can be increased or decreased in 5 dB
steps. The frequencies usually tested are octave steps i.e.
125, 250, 500, 1000, 2000, 4000 and 8000 Hz. AC is done
by delivering pure tones to the ear under test through a
suitable earphone whereas a vibrator is applied to the
mastoid in assessing BC.
7
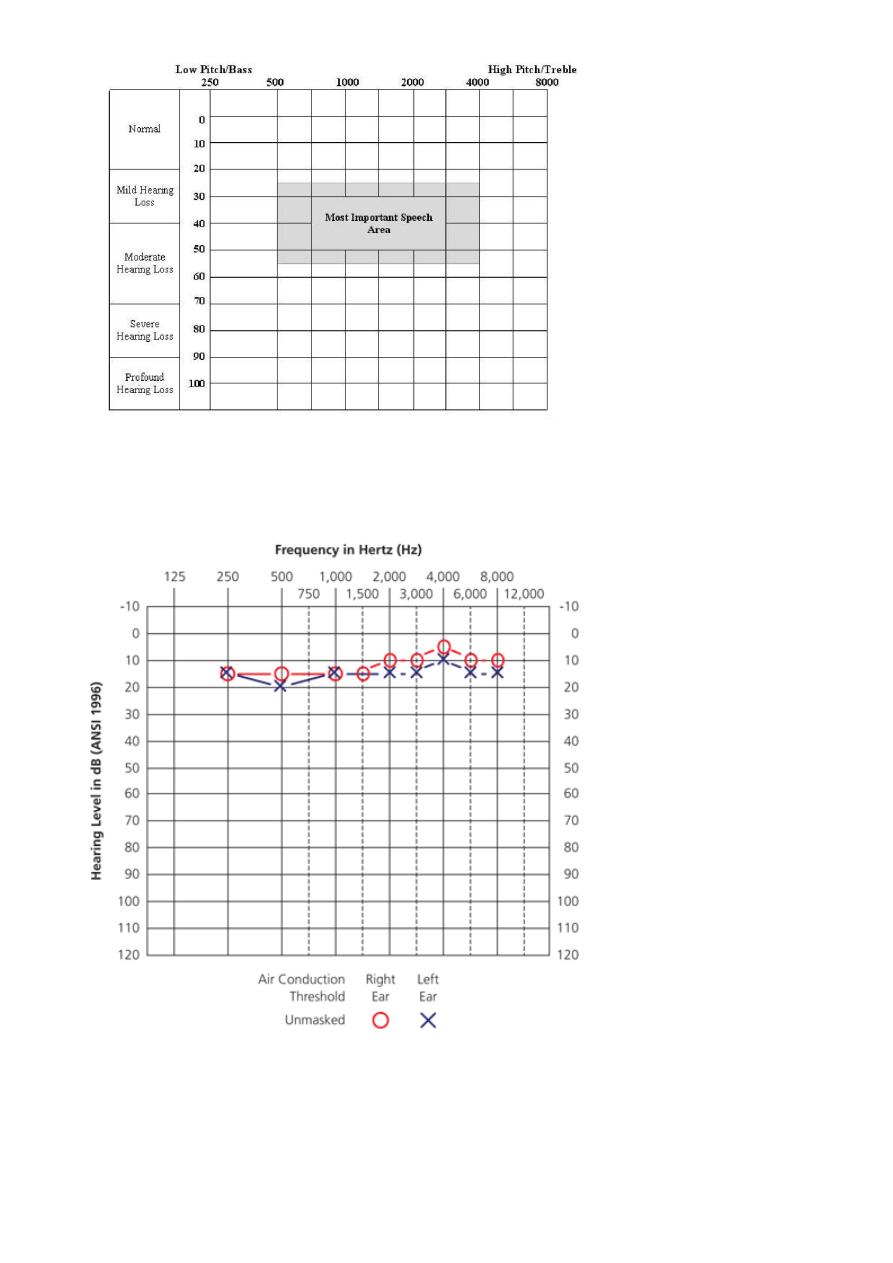
Blank audiogram paper
The fig. shows normal audiogram
2. Speech audiometry; the patient ability to hear and understand speech is measured. Two
parameters are studied: (1) speech reception threshold. (2) discrimination score.

8
3. Impedance audiometry; particularly useful in children and consists of;
(a) Tympanometry; is based on a simple principle, i.e. when a sound strikes tympanic
membrane, some of the sound energy is absorbed while the rest is reflected. A stiff
tympanic membrane would reflect more of sound energy than a compliant one.
(b) Acoustic reflex measurement: is based on the fact that a loud sound, 70-100db
above the threshold of hearing of a particular ear, causes bilateral contraction of
the stapdial muscles which can be detected by tympanometry.
Assessment of vestibular function
A. Clinical tests:
1. Spontaneous Nystagmus
2. Fistula Test; pressure change in EAM Nystagmus
( if +ve suggest erosion of horizontal semicircular canal)
3. Romberg Test; The patient is asked to stand with feet together, and arms by the side
with the eye first open and then closed. In peripheral vestibular lesions, the patient
sways to the side of the lesion when the eyes are closed while in central disorder,
patients shows instability.
4. Gait; the patient is asked to walk along a straight line to a fixed point, first with eyes
open then closed. In case of lesion of vestibular system, with eyes closed, the patient
deviate to the affected side.
5. Hallpike Maneuver; This test is particularly useful when patient complains of vertigo
in certain head positions. It also helps to differentiate a peripheral from a central
lesions. Patient sits on a couch. Examiner holds the patient's head, turns it 45˚ to
the right and then places the patient in a supine position so that his head hangs 30˚

9
below the horizontal. Patient's eyes are observed for nystagmus. The test is repeated
with the head turned to the left.
In benign paroxismal positional vertigo, nystagmus appears after a latent period
while in cetral lesions it appear immediately.
(B) Laboratory test of vestibular function
1. Rotation test
2. Electronystagmography
3. Caloric test: in this test each labyrinth can be tested separately. Syringing the ear
with hot or cold water induces convection currents within the lateral SCC and
therefore stimulates them with resulting vertigo and nystagmus. The patient lies with
the head at an angle of 30 degree above the horizontal, which brings the lateral SCC
into a vertical plane. The ears are irrigated in turn with water at 30 C then at 44 C (7 C
above and below body temperature). This situation causes nystagmus with its quick
component away from the ear on the cold testing and towards the ear on hot caloric
testing (COWS). This nystagmus commonly lasted for about 2 minutes from the
beginning of stimulation.
Canal paresis is present if the duration of nystagmus is reduced equally for both
hot and cold tests. Canal paresis is suggestive of a lesion in the peripheral
vestibular apparatus e.g. vestibule or vestibular nerve.
COWS= Cold Same Warm Opposite