1
Fifth stage
Medicine
Lec-10-11-12
د.خالد نافع
27/3/2016
Lymphoma
Most present as tumor Involving lymph nodes or other lymphoid organs such as the spleen.
But extra nodal presentation may seen.
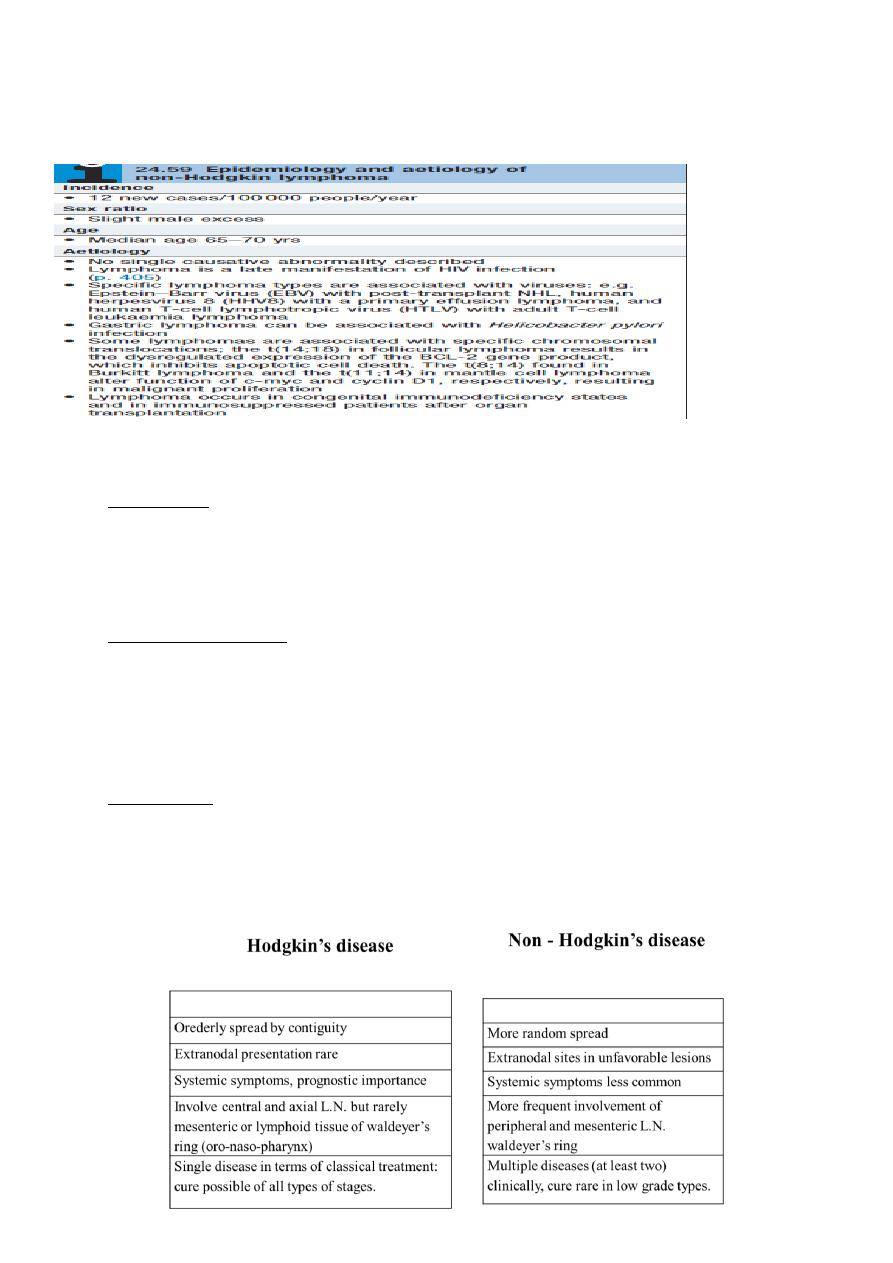
1. Hodgkin’s Lymphoma.
2.Non - Hodkin’s Lymphoma; Non-Hodgkin lymphomas are classified as low- or high-grade
tumours on the basis of their proliferation rate.
High-grade tumours divide rapidly, are typically present for a matter of weeks before
diagnosis, and may be life-threatening.
• Low-grade tumours divide slowly, may be present for many months before diagnosis, and
typically behave in an indolent fashion.
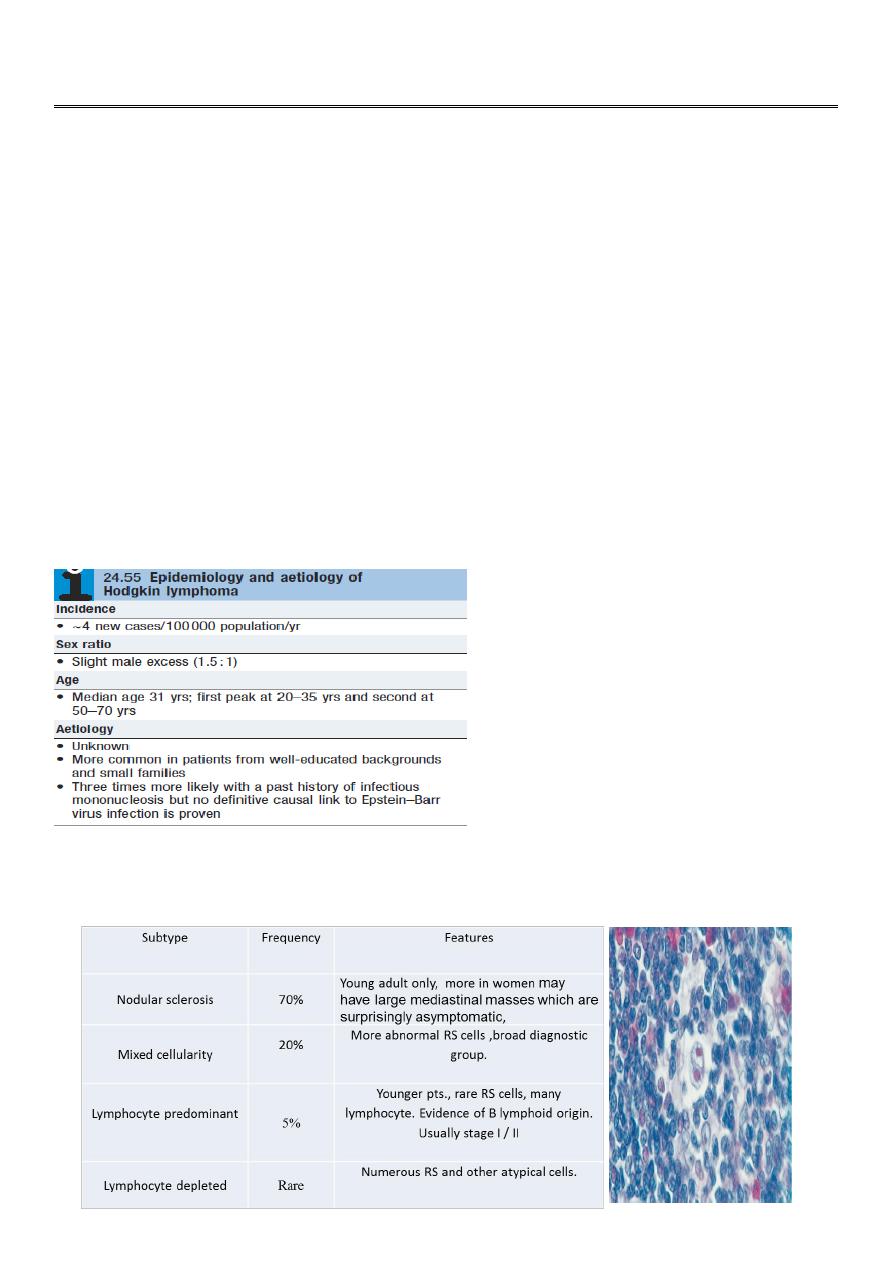
Hodgkin lymphoma
Histological WHO classification
1-CLASSICAL HL
2
2- NODULAR LP HLis now clearly recognized to be indolent NHL 5%
Clinical features
There is painless, rubbery lymphadenopathy, usually in the neck or supraclavicular fossae;
the lymph nodes may flucuate in size(wax an wan).
Hepatosplenomegaly may be present but does not always indicate disease in those organs.
Spread is contiguous from one node to the next and extranodal disease, such as bone,
brain or skin involvement, is rare.
Investigations
FBC may be normal. If a normochromic, normocytic
anaemia or lymphopenia is present, this is a poor
prognostic factor. An eosinophilia or a neutrophilia
may be present.
• ESR may be raised.
• Renal function tests are required to ensure function is normal prior to treatment.
• Liver function may be abnormal in the absence of disease or may reflect hepatic
infiltration. An obstructive pattern may be caused by nodes at the porta hepatis.

3
LDH measurements showing raised levels are an adverse prognostic factor.
• Chest X-ray may show a mediastinal mass.
• CT scan of chest, abdomen and pelvis permits staging. Bulky disease (> 10 cm in a single
nodemass) is an adverse prognostic feature.
• Lymph node biopsy may be undertaken surgically or by percutaneous needle biopsy under
radiological guidance
Management
1-chemotherapy;
The ABVD regimen (doxorubicin,vinblastine,bleomycin and dacarbazine)
*cardiac and pulmonary toxicity, due to doxorubicin and bleomycin respectively.
2-radiotherapy
* The majority of HL patients are now treated with chemotherapy and adjunctive
radiotherapy.
* Early-stage patients usually includes additional treatment with radiotherapy to the
involved lymph nodes after four courses of ABVD.
* Advanced-stage disease are most commonly managed withchemotherapy alone. 6–8
cycles of ABVD.
* Patients with disease which is resistant to therapy may be considered for autologous
HSCT.
* Treatment response is assessed clinically and by repeat CT and newer (scanning
modalities such as positron emission tomography (PET
4
Non-Hodgkin lymphoma
Non-Hodgkin lymphoma (NHL) represents a monoclonal proliferation of lymphoid cells of B
cell (70%) or T cell (30%) origin.
Working formulation for lymphoma classification:
• Low grade :
o diffuse small lymphocytic.
o follicular small cleaved cell.
o follicular mixed small and large cell.
• Intermediate grade :
o diffuse small cleaved cell.
o diffuse small and large cell.
o diffuse large cell lymphoma.
o follicular large cell lymphoma.
• High grade :
o immunoblastic lymphoma.
o small non cleaved cell (Burkitt-type).
o lymphoblastic lymphoma.
5
Clinical presentation
1- most pt present with one or several enlarge painless LN. cervical, inguinal and axillary's
nods are most frequently involved. Hepatosplenomegaly may be present
2- 1/5-1/3 of pt with intermediate and high grade lymphoma present in extra- nodal site
such as waldeyers ring, GIT, skin, salivary gland, bone.
3- compression syndromes may occur, gut obstruction, ascites, superior vena caval
obstruction and spinal cord compression.
4 - BM involvement in high grade 10% and 50-60% in low grade.
5- T cell lymphoma are usually first diagnosed in the skin lead to cutaneous T cell
lymphoma (sezary syndrome), erthro-derma and circulating lymphoam cells with hyper
convoluted nuclei.
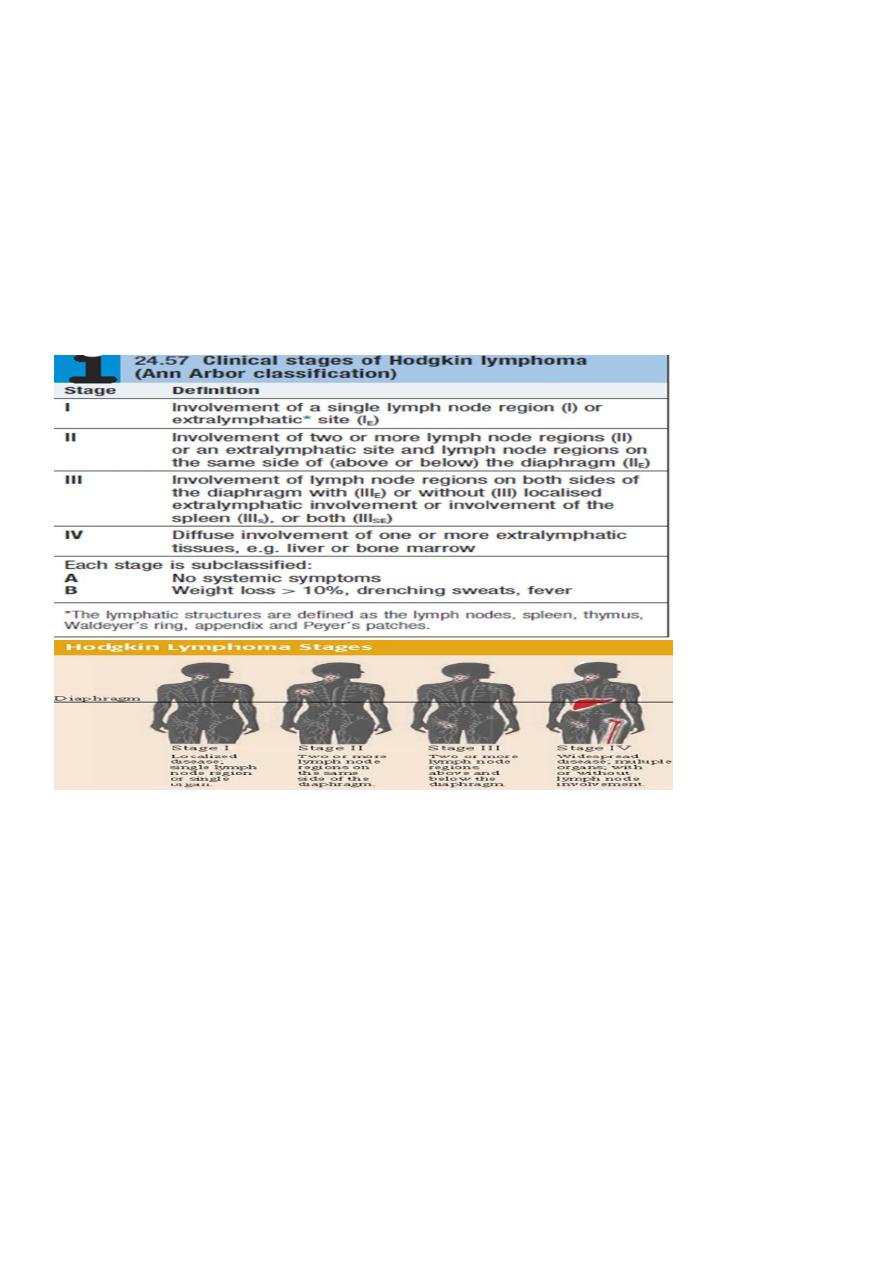
**The same staging system is used for both HL and NHL, but NHL is more likely to be stage
III or IV at presentation.
Investigations:
Same as HD inaddition;
1. Bone marrow aspiration and trephine.
2. Immunophenotyping of surface antigens to distinguish T from B cell tumours.
3. Cytogenetic analysis to detect chromosomal translocations.
4. Immunoglobulin determination.
5. Measurement of uric acid levels.
6. HIV testing.
Treatment
Low grade NHL |:
o A symptomatic pts may not require treatment
o Radiotherapy : for stage I disease.
o Chemotherapy : oral therapy with chlorambucil.
o The anti-CD20 antibody rituximab.
Rituximab (R) in combination with cyclophosphamide, vincristine and prednisolone
(R-CVP).
Transplantation.
High-grade NHL *Prognosis
o Chemotherapy; R-CHOP
o Radiotherapy
o HSCT
6
HAEMATOPOIETIC STEM ELL TRANSPLANTATION (HSCT)
A process in which abnormal, malignant, or non-functioning marrow cells are replaced with
normal marrow stem cells.
Two Kinds of Stem Cells
Embryonic (also called “pluripotent”) stem cells are capable of developing into all the cell
types of the body.
Adult stem cells are less versatile and more difficult to identify, isolate, and purify.
Source of Stem cells
Stem cells may be derived from autologus, allogeneic or xenogenic sources.
Histocompatability is prerequisite for transplantation of allogeneic stem cells.
Fetal tissue is the best current tissue source for human neural stem cells, however ethical
issues are a major concern.
Sources of haemopoetic stem cells
Bone marrow.
Peripheral blood stem cells(PBSC).
Placental (cord blood) blood transplant.
Fetal liver.
Placenta a Source of Stem Cells
Placental stem cells, like umbilical cord blood and bone marrow stem cells, can be used to
cure chronic blood-related disorders such as sickle cell disease, thalasemia, and leukaemia.
Umbilical Cord Blood Stem Cell Transplant
Umbilical cord blood stem cell transplants are less prone to rejection than either bone
marrow or peripheral blood stem cells.
This is probably because the cells have not yet developed the features that can be
recognized and attacked by the recipient's immune system
7
Types of HSCT
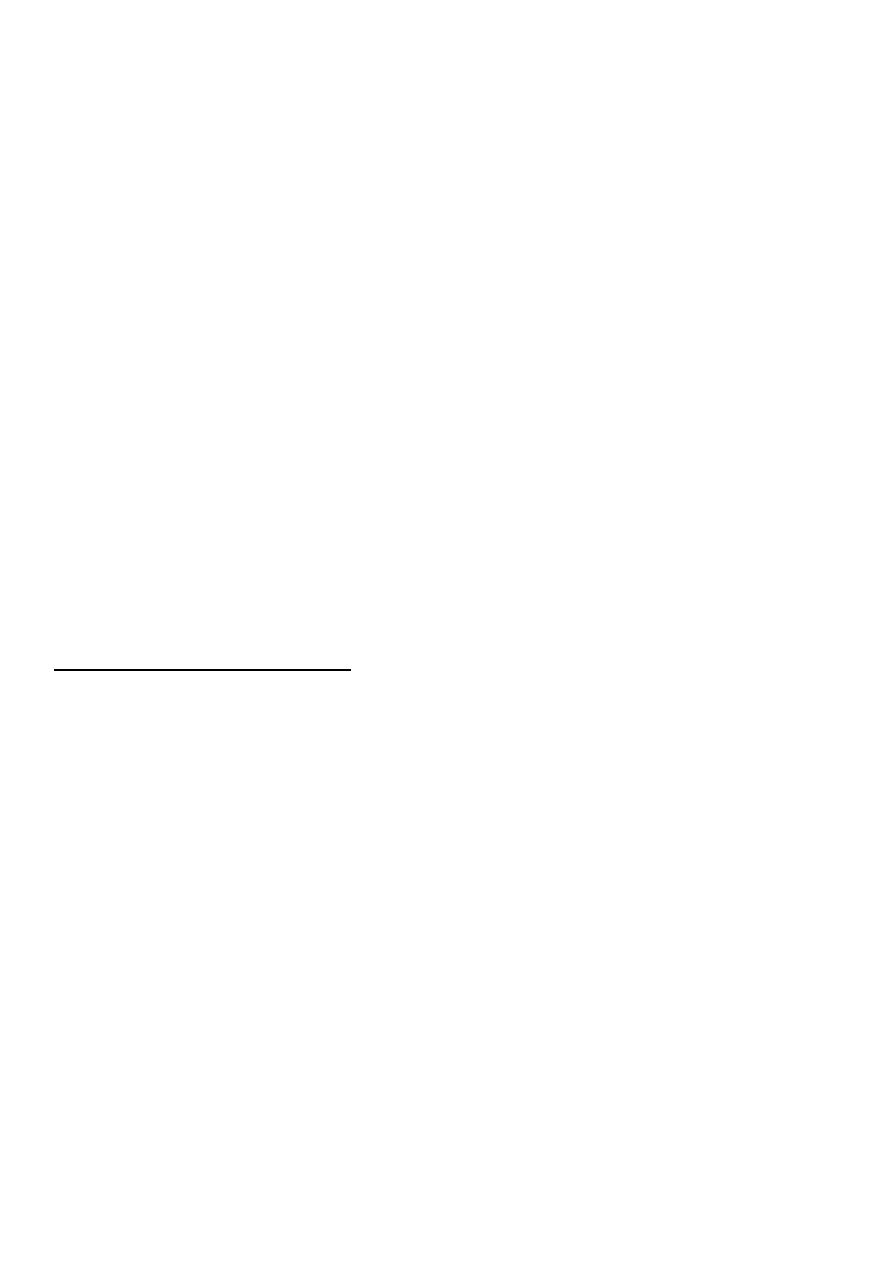
Allogeneic stem cell transplantation:
Normal BM cells are harvested from the donor& infusion into the pts after aggressive
marrow ablative therapy.
The success is compromised by the fact that the transplanted lymphocytes may treat with
recipients tissues.
Sources of stem cells from another donor (allogeneic) are primarily relatives (familial-
allogeneic) or completely unrelated donors (unrelated-allogeneic). The stem cells in this
situation are extracted from either the donor's body or cord blood
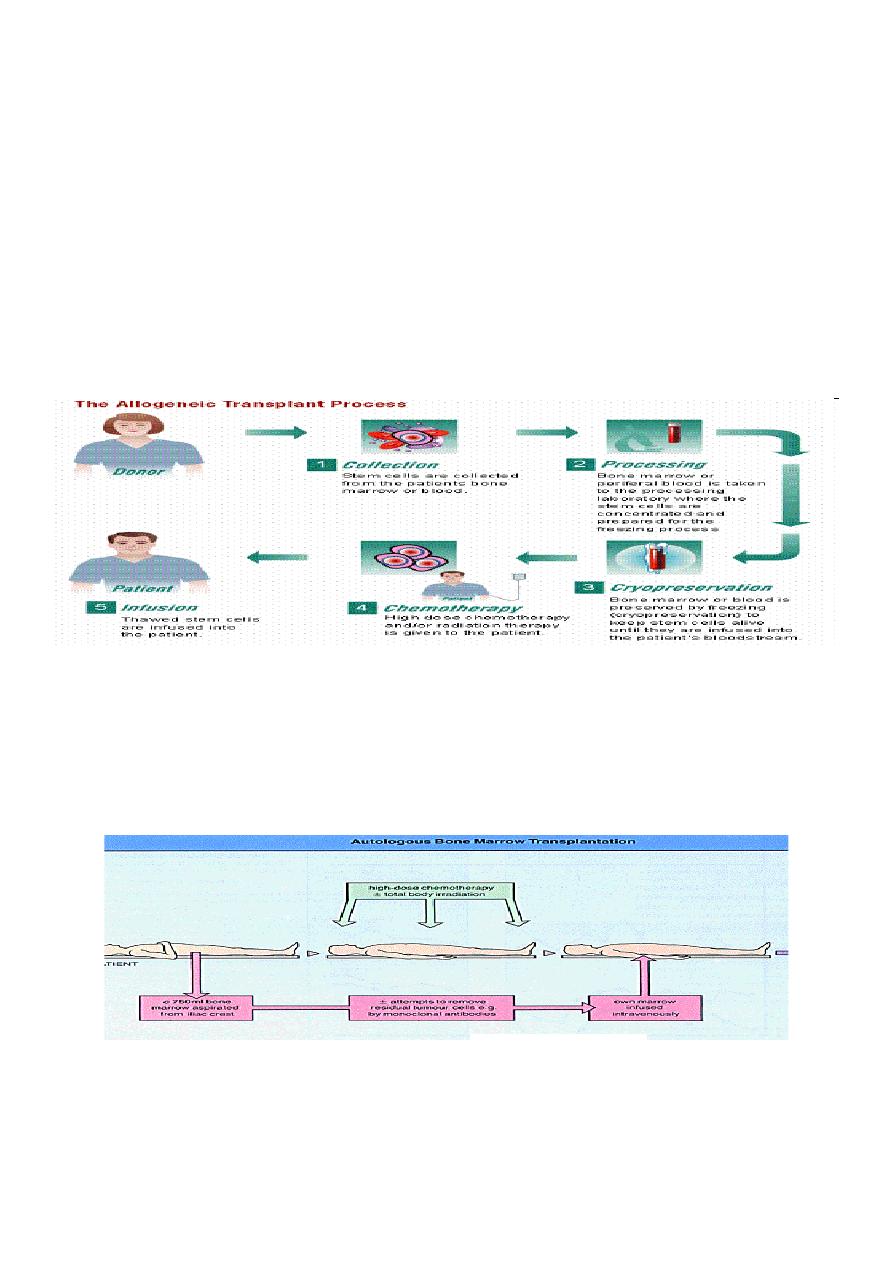
Autologus stem cell transplantation:
Is the process of harvesting, purging (treating for residual malignancy) and cryopreserving
the patient's own marrow cells for re-infusion after high does chemotherapy or total body
irradiation(TBI).
Sources of the patient's own stem cells (autologous) are either the cells from patient's own
body or his or her cord blood. For autologous transplants physicians now usually collect
stem cells from the peripheral blood rather than the marrow.

8
This procedure is easier, unlike a bone marrow harvest, it can take place outside of an
operating room and the patient does not have to be under general anaesthesia.
INDICATIONS OF BMT
1-Malignancy
AML (1st remission)
ALL (high risk 1st CR, good risk 2nd CR)
CML
CLL
MDS
Hodgkins disease
NHL
Multiple myeloma.
2-Defective haemopoiesis
Aplastic anaemia.
Sickle cell anaemia.
Thalassimia major.
Granulocyte disease.
3-Immunedeficiency
sever combined immune deficiency(SCID).
Adenosine deaminase(ADA) deficiency
Complications:
20-50% of pts will experience one or more of the following :
1-Chemotherapy and radiation toxicity :
mucositis : GIT, respiratory tract, bladder.
Intrahepatic vascular occlusive disease (VOD).
Toxic pneumonitis .
CNS toxicity.
Endocrine dysfunction lead to hypothyoidisim.
Cataract.
2. Graft Versus host disease (GVHD):
Acute 20-100 days
* Due to engrafment of donor T cell, that react against the recipient tissues.

9
It can affect the skin,causing rashes, the liver, causing jaundice, and the gut, causing
diarrhoea, and may vary from mild to lethal. Prevention includes HLA-matching of the
donor, immunosuppressant drugs, including methotrexate, ciclosporin, alemtuzumab or
antithymocyte globulin.
Chromic 6-12 months
It often resembles a connective tissue disorder (scleroderma-like), treated with
corticosteroids and prolonged immunosuppression with, for example, ciclosporin.
Graft versus leukaemia effect?.
3. Infections:
Due to immundeficiency & granulocytopenia :
a-Bacterial infection G+ve, G.-ve .
b-Fungal infection : candida albicans.
c-Viral : Herpes zoster, CMV.
d-Parasitic infection : Interstitial pneumonitis caused by Pneumocystis jiroveci
Interstitial pneumonitis :
-chemotherapy & radiation toxicity.
-Mortality 50-90%.
Myelodysplastic syndrome(MDS)
Myelodysplastic syndrome (MDS) consists of a group of clonal haematopoietic disorders
which represent steps in the progression to the development of leukaemia.
MDS presents with consequences of bone marrow failure (anaemia, recurrent infections or
bleeding),usually in older people (median age at diagnosis is 69 years).
The blood film is characterised by cytopenias and abnormal-looking (dysplastic) blood cells,
including macrocytic red cells and hypogranular neutrophils with nuclear hyper-or
hyposegmentation.
The bone marrow is hypercellular, with dysplastic changes in all three cell lines. Blast cells
may be increased but do not reach the 20% level that indicates acute leukaemia
10
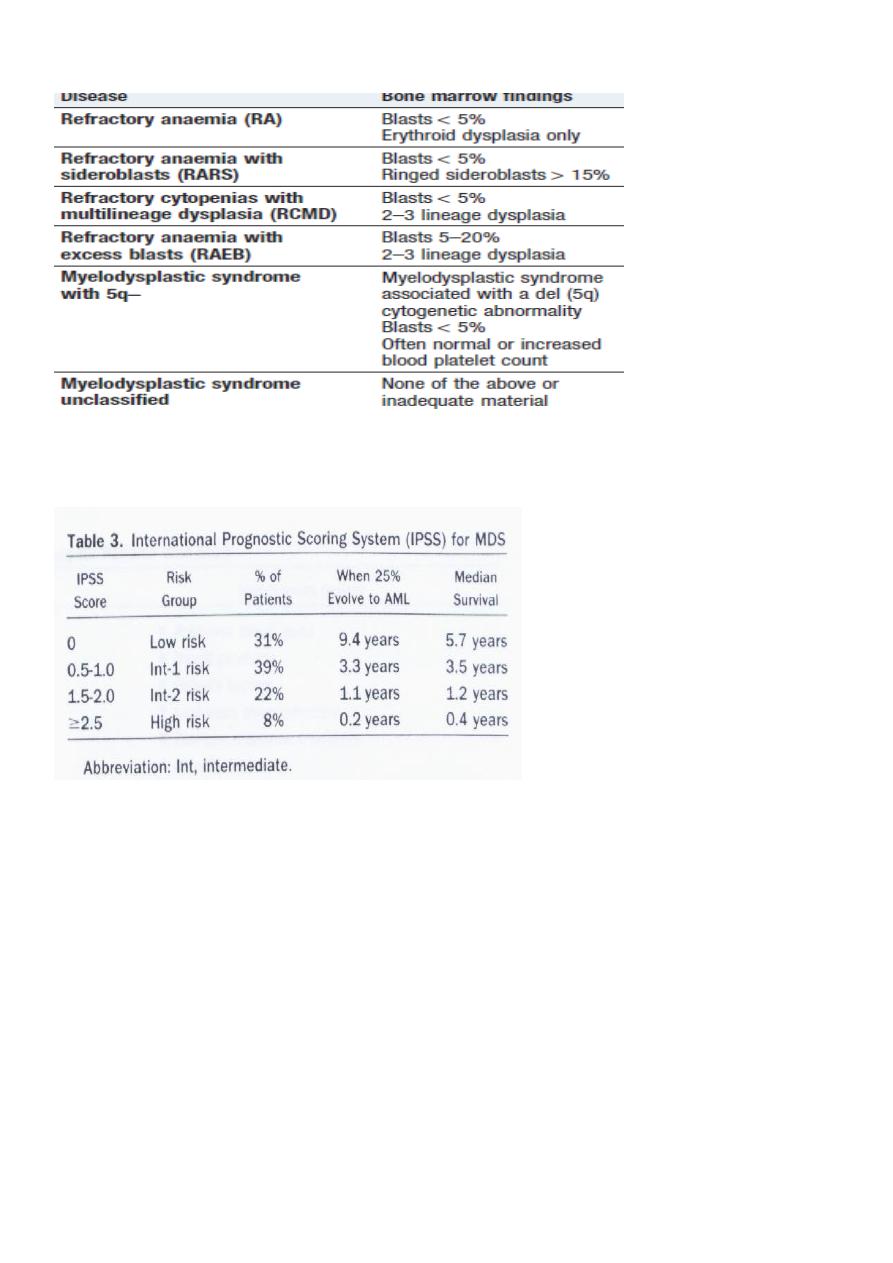
WHO classification of myelodysplastic syndromes
International Prognostic Scoring System (IPSS)
Management:
*For younger patients with higher-risk disease, allogeneic HSCT may afford a cure.
*A trial of erythropoietin and granulocyte–colony-stimulating factor (G–CSF) is
recommended in some patients with early disease to improve haemoglobin and white cell
counts.
*Hypomethylating agent azacytidine has improved survival by a median of 9 months for
high-risk patients, is recommended for those not eligible for transplantation