
1
Fifth stage
Surgery
Lec-1
.د
أ
ر
ك
ا
ن
29/3/2016
Preoperative Evaluation
The goals of preoperative evaluation are:
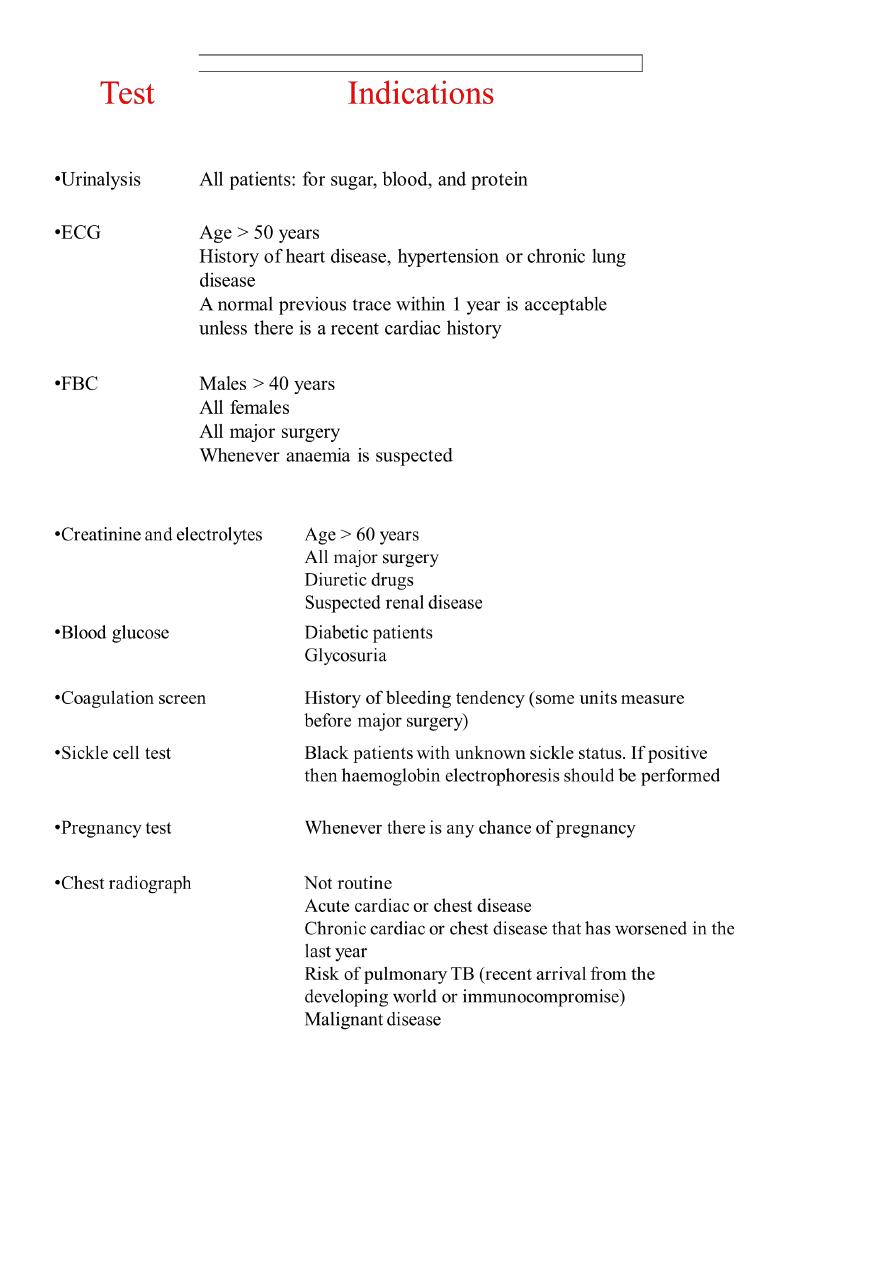
To screen for and properly manage comorbid conditions.
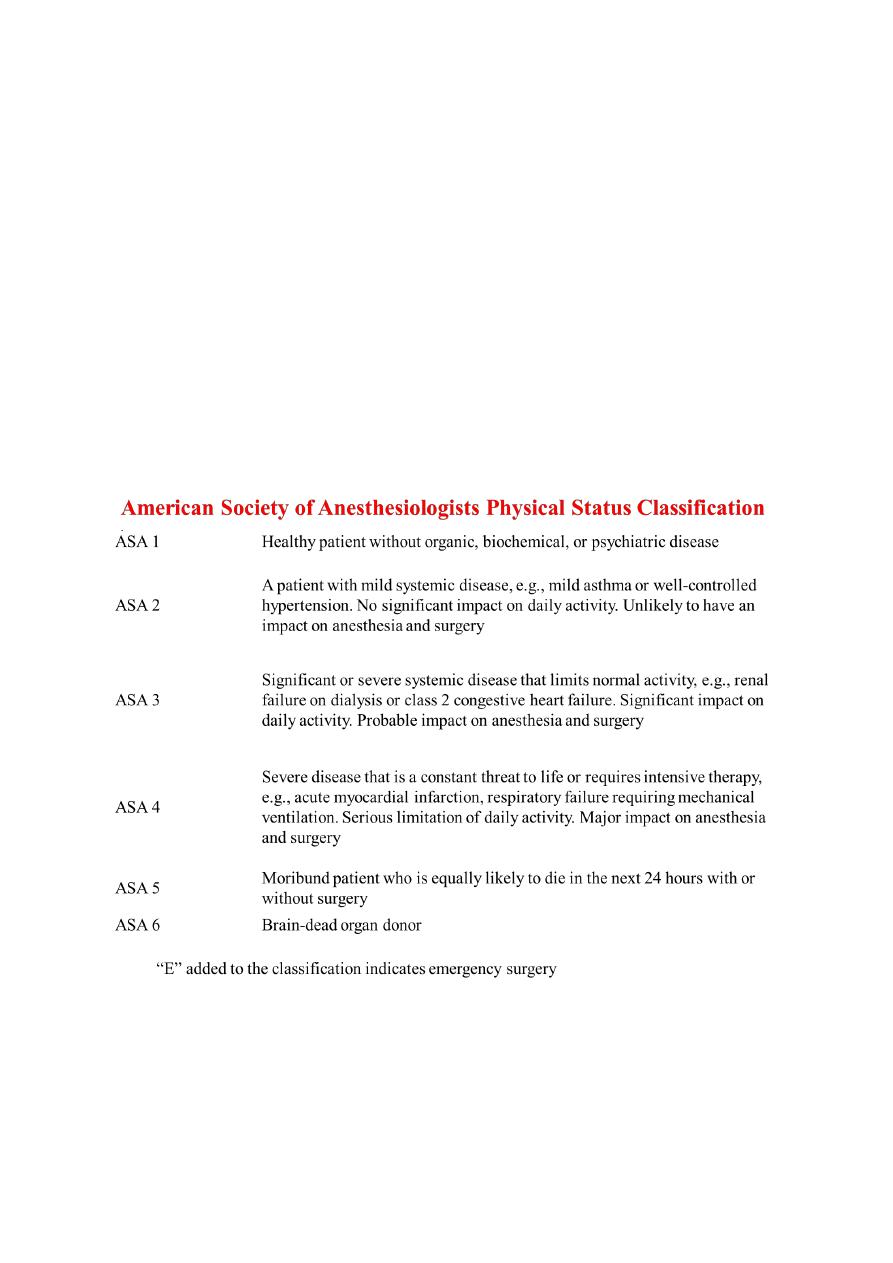
To assess the risk of anesthesia and surgery and lower it.
To identify patients who may require special anesthetic techniques or postoperative
care.
To educate patients and families about anesthesia and the anesthesiologist’s role.
To obtain informed consent.
Cardiovascular
• Patients with ischemic heart disease are at risk for myocardial ischaemia or infarction
in the perioperative period
• A thorough history should ascertain whether angina is new or has recently changed
from a previously stable pattern
• A description of the patient's exercise tolerance .
• Hx of hypertension , heart failure ; valvular heart disease; arrhythmias; etc
Respiratory
• Cigarette smoke has several adverse effects, including alteration of mucus secretion,
clearance, and decrease in small airway calibre. It also may alter the immune
response. The chronic smoker should be encouraged to abstain from smoking for at
least 8 weeks prior to the operation,' but stopping smoking for even 24 hours may
produce benefits in cardiovascular physiology and carboxyhemoglobin levels
• Patients with chronic obstructive pulmonary disease (COPD) are at increased risk of
perioperative respiratory complications. Anaesthesia, surgery and postoperative
analgesia all predispose the patient with COPD to respiratory depression, atelectasis,
retained secretions, pneumonia and respiratory insufficiency or failure
• The patient with asthma is at particular risk as manipulation of the airway and cold
dry anaesthetic gases are potent triggers of intraoperative bronchospasm
• Determine the presence of cough and the colour and amount of sputum. Ensure that
there is no acute upper respiratory infection

2
• Restrictive lung disease will be worsened by upper abdominal or thoracic surgery,
and place the patient at increased risk for perioperative failure
• Any disease process which leads to an altered control of breathing (obstructive sleep
apnea, CNS disorders, etc.) may lead to profound respiratory depression from the
drugs used in the perioperative period, and may require postoperative monitoring in
a critical care setting
Neuromuscular
• If the patient has an intracranial lesion, seek early signs and symptoms of raised
intracranial pressure such as headaches, nausea, vomiting, confusion and
papilledema
• A history of TIA's or CVA's suggests significant cerebrovascular disease
• A history of seizures, and determine the type, frequency and time of last occurrence.
Note any anticonvulsant medications the patient is receiving
• The patient with a history of spinal cord injury is at risk for a number of perioperative
complications including respiratory failure, arrhythmias, autonomic hyperreflexia,
hyperkalemia, pathologic fractures and pressure sores.
• Disorders of the neuromuscular junction such as myasthenia gravis, myasthenic
syndrome, etc.
Endocrine
• Patients with diabetes mellitus require careful management in the perioperative
period, as the stress of surgery and perioperative fasting can cause marked swings in
blood glucose. Diabetics frequently have widespread end organ damage involving the
cardiovascular, nervous and renal systems
• Patients with thyroid disease may experience difficulties under anaesthesia.
Profound hypothyroidism is associated with myocardial depression and exaggerated
responses to sedative medications. Hyperthyroid patients are at risk for perioperative
thyroid storm. Thyroid goitres may compress the airway and involve the recurrent
laryngeal nerve leading to vocal cord palsy
• Phaeochromocytoma. These patients are at risk for extreme swings in blood pressure
and heart rate in the perioperative period, and require intensive preoperative
therapy .

3
• Patients at risk for adrenal suppression (history of exogenous steroid therapy) may
not be able to increase their own corticosteroid production to match the imposed
stress of surgery.
GI-Hepatic
• Patients with hepatic disease frequently present problems with fluid and electrolyte
imbalance, coagulopathies and altered drug metabolism
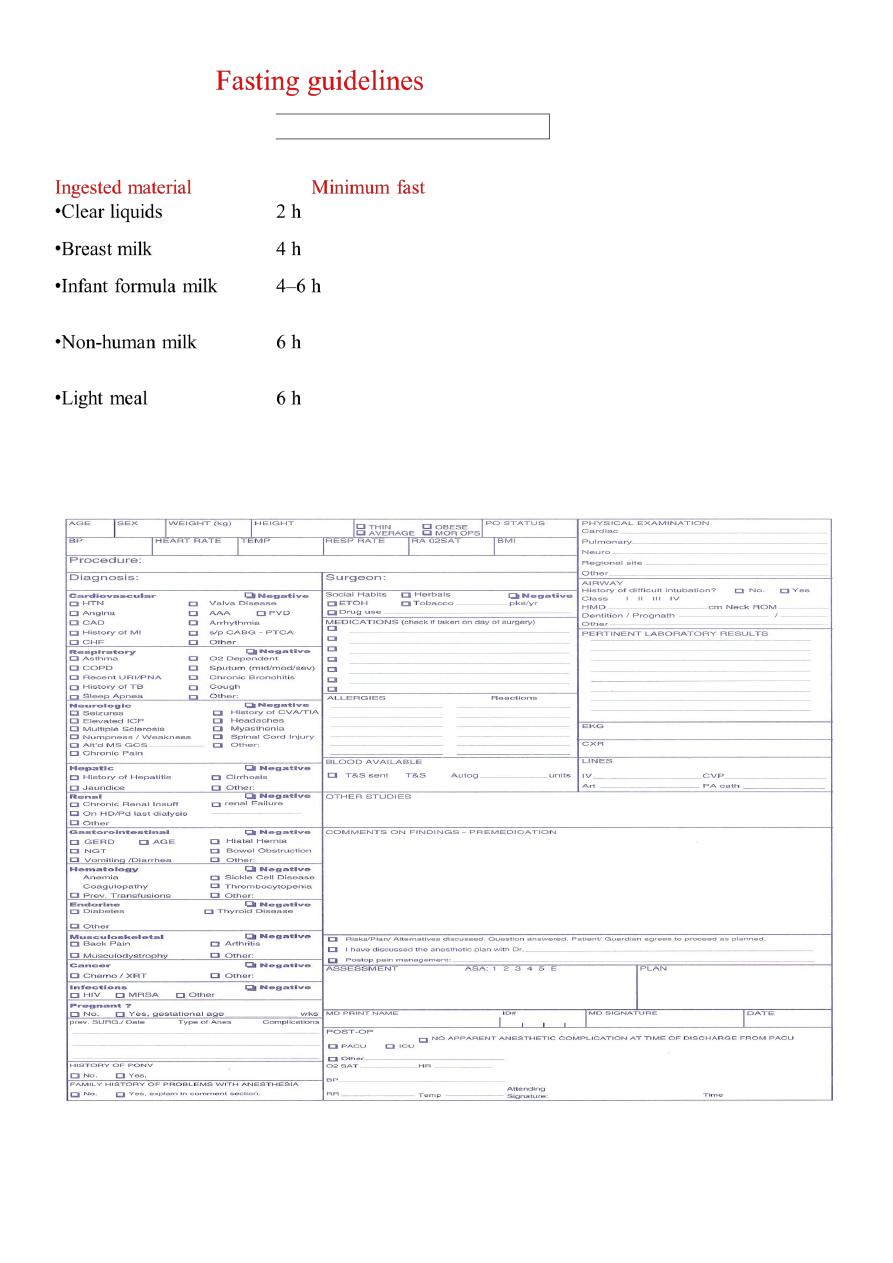
• Patients with gastroesophageal reflux (GER) are prone to regurgitation of gastric
contents and aspiration pneumonitis during the perioperative period
Renal
• Disorders of fluid and electrolyte balance are common in the perioperative period.
• Generally all fluid and electrolyte disorders should be corrected prior to elective
surgery
Haematologic
• Anemias of a variety of causes are common in the patient undergoing surgery. A
minimum haemoglobin level of 10 gm/dL was traditionally required before a patient
could undergo elective surgery
• Now the "transfusion trigger" must be individualized to the patient, bearing in mind
the chronicity of the anemia, the likelihood of perioperative blood loss, and the
patient's co-existent disease
• Coagulopathies involving clotting factors and platelets, both congenital and acquired,
require careful management
Medications and Allergies
• A detailed list of the patients' medications and allergies is an essential part of the
preoperative assessment.
• As a general rule, all cardiac and pulmonary medications and most other necessary
medications should be taken with sips of water at the usual time, up to and including
the day of surgery. Possible exceptions to this include warfarin, NSAID's, insulin
(adjustment of the dose is needed on the day of surgery), oral hypogylcemics and
antidepressants.
4
Prior Anaesthetics
The patient undergoing anaesthesia and surgery should be carefully questioned on their
response to previous anaesthetics and a family history of problems with anaesthesia
Physical Examination
• The physical examination should focus on evaluation of the airway, the
cardiovascular system, the respiratory system, and any other systems identified as
having symptoms or disease from the history.
• General
A general assessment of the patient's physical and mental status is performed. Note
whether the patient is alert, calm, and cooperative.
5
6