Eczema
Omar AbdullahEczema (eczematous inflammation) is the most common inflammatory skin disease.
Although the term dermatitis is often used to refer to an eczematous eruption, the word means inflammation of the skin and is not synonymous with eczematous processes.Stages of eczema
acute, subacute, and chronic.Each represents a stage in the evolution of a dynamic inflammatory process. Clinically, an eczematous disease may start at any stage and evolve into another.
Most eczematous diseases, if left alone (i.e., neither irritated, scratched, nor medicated), resolve in time without complication.
This ideal situation is almost never realized; scratching, irritation, or attempts at topical treatment are almost inevitable.
Some degree of itching is a cardinal feature of eczematous inflammation.
Acute Vesicles, blisters, intense redness. Intense itch. Contact allergy (poison ivy), severe irritation, id reaction, acute nummular eczema, stasis dermatitis, pompholyx (dyshidrosis).
Subacute Redness, scaling, fissuring, parched appearance, scalded appearance. Slight to moderate itch, pain, stinging, burning. Contact allergy, irritation, atopic dermatitis, stasis dermatitis, nummular eczema, asteatotic eczema, fingertip eczema.
Chronic Thickened skin, skin lines accentuated (lichenified skin), excoriations, fissuring. Moderate to intense itch. Atopic dermatitis, habitual scratching, lichen simplex chronicus, chapped fissured feet, nummular eczema, asteatotic eczema, fingertip eczema, hyperkeratotic eczema.



Hand Eczema
Inflammation of the hands is one of the most common problems encountered by the dermatologist.Hand dermatitis causes discomfort and embarrassment and, because of its location, interferes significantly with normal daily activities.
Hand dermatitis is common in industrial occupations: it can threaten job security if inflammation cannot be controlled.






Treatment Options for Hand Eczema
Skin protection
Gloves
Barrier creams
Bland emollients
Lifestyle changes
Workers’ education
Topical treatments
Corticosteroid creams, ointments, emollient foamsTacrolimus, pimecrolimus
Coal tar and derivatives
Irradiation with UV light
Irradiation with x-rays
Systemic treatments
AntihistaminesAzathioprine
Methotrexate (MTX)
Cyclosporine
Oral corticosteroids in short treatment course
Irritant And Allergic
Contact Dermatitis
Irritant VS Allergic
People at risk Everyone vs Genetically predisposedMechanism of response Nonimmunologic (a physical and chemical alteration of epidermis) vs Delayed hypersensitivity reaction
Number of exposures Few to many (depends on individual’s ability to maintain an effective epidermal barrier) vs One or several to cause sensitization
Nature of substance Organic solvent, soaps vs Low-molecular-weight hapten (e.g., metals, formalin, epoxy)
Concentration of substance required Usually high vs May be very low
Mode of onset Usually gradual as epidermal barrier becomes compromised vs Once sensitized, usually rapid; 12 to 48 hours after exposure
Distribution Borders usually indistinct vs May correspond exactly to contactant (e.g., watchband, elastic waistband)
Investigative procedure Trial of avoidance vs Trial of avoidance, patch testing, or both
Management Protection and reduced incidence of exposure vs complete avoidance




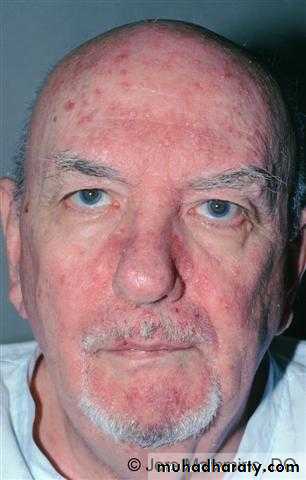
Seborrheic
DermatitisSeborrheic dermatitis is a common, chronic, inflammatory disease with a characteristic pattern for different age groups.
The yeast Malassezia ovalis probably is a causative factor, but both genetic and environmental factors seem to influence the onset and course of the disease.
Many adult patients have an oily complexion, the so-called seborrheic diathesis.
In adults, seborrheic dermatitis tends to persist, but it undergoes periods of remission and exacerbation.
The extent of involvement among patients varies widely.
Infants (Cradle Cap)
Infants commonly develop a greasy adherent scale on the vertex of the scalp.Minor amounts of scale are easily removed by frequent shampooing with products containing sulfur, salicylic acid, or both (e.g., Sebulex shampoo, T/Gel shampoo).
Scale may accumulate and become thick and adherent over much of the scalp and may be accompanied by inflammation. Secondary infection can occur.



Derma-Smoothe/FS lotion (peanut oil, mineral oil, fluocinolone acetonide 0.01%) to the scalp and washing several hours later.
Remissions possibly can be prolonged with frequent use of salicylic acid or tar shampoos.
Ketoconazole is another option for the treatment of infantile seborrheic dermatis, to avoid the side effects of topical corticosteroid in long-term use and on large surface areas of treatment.
Adolescents and Adults (Classic Seborrheic Dermatitis)
Most individuals periodically experience fine, dry, white scalp scaling with minor itching; this is dandruff.They tend to attribute this condition to a dry scalp and consequently avoid hair washing.
Avoidance of washing allows scale to accumulate and inflammation may occur.
Patients with minor amounts of dandruff should be encouraged to wash every day or every other day with antidandruff shampoos.
Fine, dry, white or yellow scale may occur on an inflamed base.
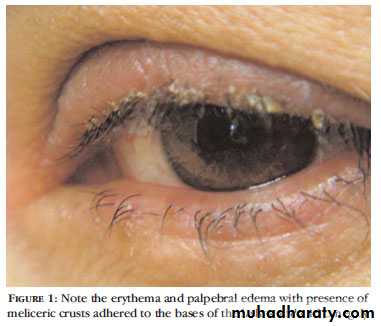
The distribution of scaling and inflammation may be more diffuse and occur in the seborrheic areas: scalp and scalp margins, eyebrows, base of eyelashes, nasolabial folds, external ear canals, posterior auricular fold, and presternal area .




Treatment
Frequent washing with Shampoos (ketoconazle 2%)Topical Steroids (foams and solutions)
Oral antifungals (itraconazole capsules 100mg)