1
Fifth stage
ENT
Lec-19
د.سعد
21/4/2016
Deafness (Hearing loss)
Definition: it is subjective impairment of hearing.
I. Conductive
A. Congenital: congenital meatal atresia.
B. Acquired:
1. External ear: Wax and foreign bodies.
2. Middle ear:
a. Trauma: TM perforation and ossicular disconnection.
b. Inflammatory: acute and chronic suppurative otitis media.
c. Eustachian tube: secretory otitis media.
d. Tumors: glomus jugulare & sq. cell carcinoma.
3. Otic capsule: otosclerosis.
II. Sensorineural hearing loss.
Sensory (cochlear) hearing loss, i.e. cochlear lesion.
Neural (Retrocochlear) hearing loss, i.e. auditory nerve lesion.
A. Congenital:
a. Syndromes: Pendred's and trisomy 18.
b. Intrauterine infections: Rubella, Syphilis & toxoplasmosis.
c. Toxins: kernicterus.
B. Acquired
1. Cochlear
a. Traumatic; head injury and blast injury.
b. Infective: labyrinthitis, measles, mumps and syphilis.
c. Metabolic: Meniere's disease.
d. Toxins: Ototoxic drugs.
e. Degenerative: Presbyacusis.
2. Retrocochlear:
a. Neoplastic: acoustic neuroma.
b. Meningitis.
c. Multiple sclerosis.
2
Hearing Aids ( HA )
A hearing aid is an electro-acoustic device used to amplify sounds.
Design
The basic components of any hearing aid are:
1- Receiver ( microphone)
2- Amplifier
3-
Sound transmitter (Ear phone)
4- Power supply
Types of hearing aid
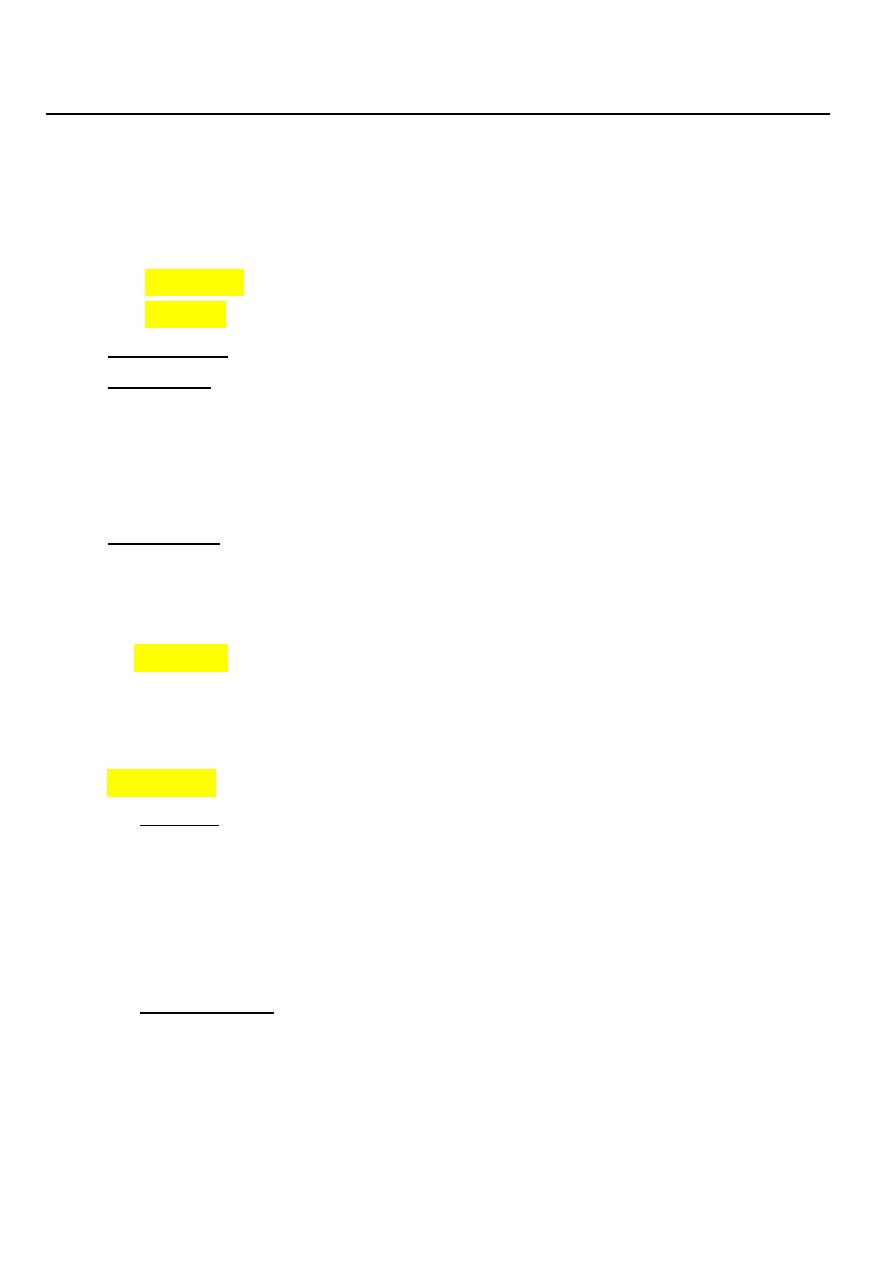
1- Behind-The-Ear:
Behind-The-Ear hearing aid
2- In-The-Ear and In-The-Canal Aids
3- Body-worn aids
4- Bone conduction HA
5- Bone-anchored hearing aids (BAHA): surgically implanted abutment to transmit
sound by direct conduction through the bone to the cochlea.
Cochlear implant:
an electronic device that can provide useful hearing for persons who have severe
SNHL who cannot benefit from HA. It is composed of: A. External component:
which consists an external speech processor and transmitter. B. Internal
component: is surgically implanted and comprises the receiver / stimulator package
with an electrode array.
Otosclerosis (Otospongiosis)
Otosclerosis is a disease of otic capsule or bony labyrinth, causing hearing loss. The
hard compact bone of the labyrinth is replaced by patches of spongy bones, hence the
French name otospongiose. This abnormal bone is thought to produce toxins that can
3
affect the cochlea causing SNHL. However, more commonly, the bony overgrowth
affect the footplate of stapes, which can result in its fixation, and this leads to CHL.
Aetiology: is unknown but the following may be considered:
1. Hereditary factors: there is family history in 50% of cases. It is inherited by
autosomal dominant pattern with incomplete penetration.
2. Racial distribution: white races (Caucasian) are more commonly affected than
coloured.
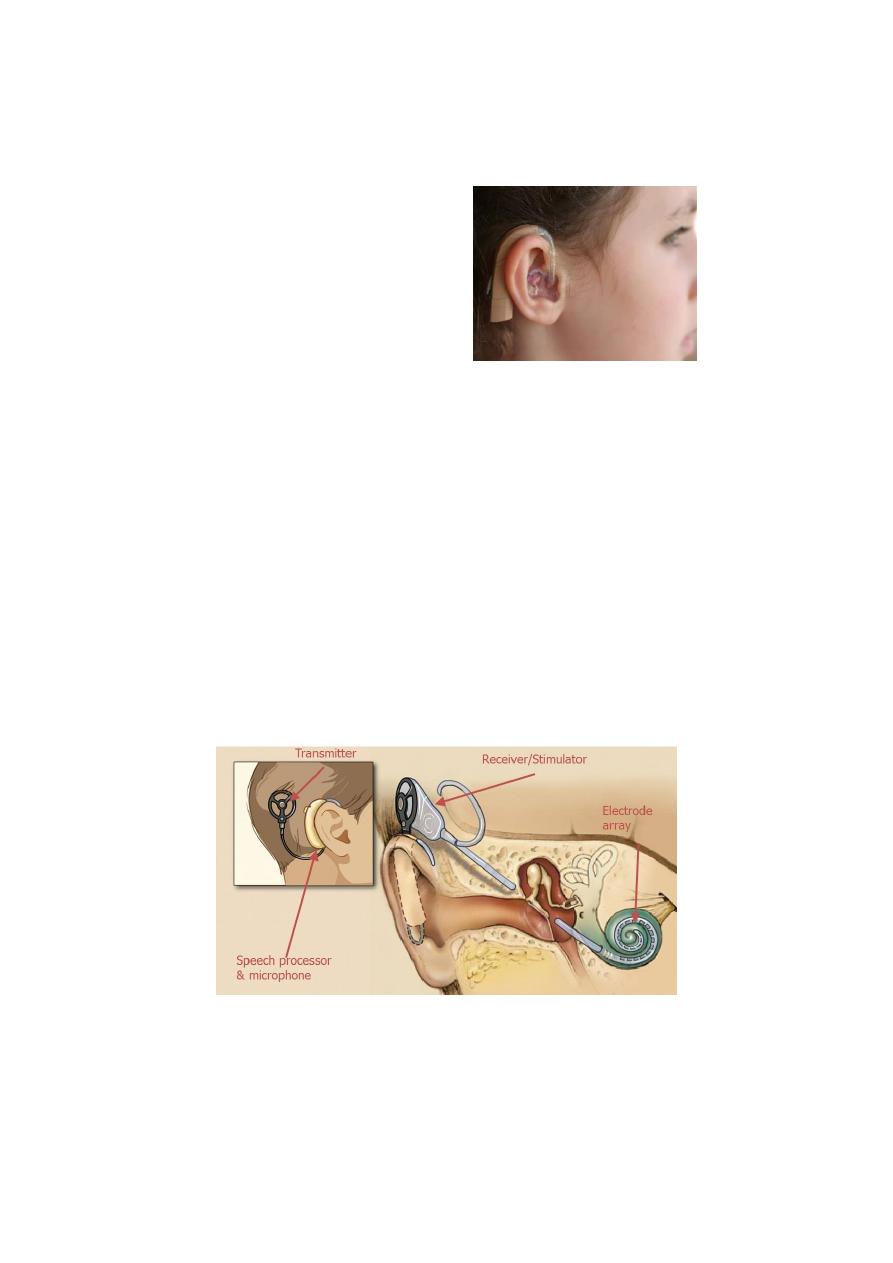
Pathology
The condition is commonly bilateral. The normal bone is absorbed and replaced by
vascular spongy osteoid bone. The most
common site of disease is on the
promontory immediately anterior to the
oval window (Fissula ante fenestram). In
advanced cases the stapes become
ankylosed in position causing conductive
deafness. Cochlear involvement may also
occur leading to SNHL.
Clinical picture
Age: 15-45 years of age.
Sex: the disease appears more frequently in females 2:1.
Pregnancy: may accelerate the condition but NEVER cause it.
The symptoms are:
1. Hearing loss: This is the presenting symptom. It is painless and progressive with
insidious onset. Often it is bilateral (80%) and of conductive type.
2. Paracusis Willisii: An otosclerotic patient hears better in noisy than quiet
surroundings.
3. Tinnitus: is present in 75% of cases.
4. Vertigo: is rare symptom.
5. Speech: Characteristically, the patient speaks in quite voice, very different from
the loud and harsh speech of those with SNHL.
4
Examination
1. Otoscopy: The TM is normal. In 10% of cases a "flamingo pink blush" (Shwartze's
sign) may be seen through the membrane due to hyperaemia of the promontory.
This usually indicates rapid progression of the disease.
2. Tuning fork test....
3. P.T.A.: conducive deafness.
Treatment
1. Medical: There is no medical treatment that cure otosclerosis. Sodium fluoride has
been tried to arrest cochlear loss.
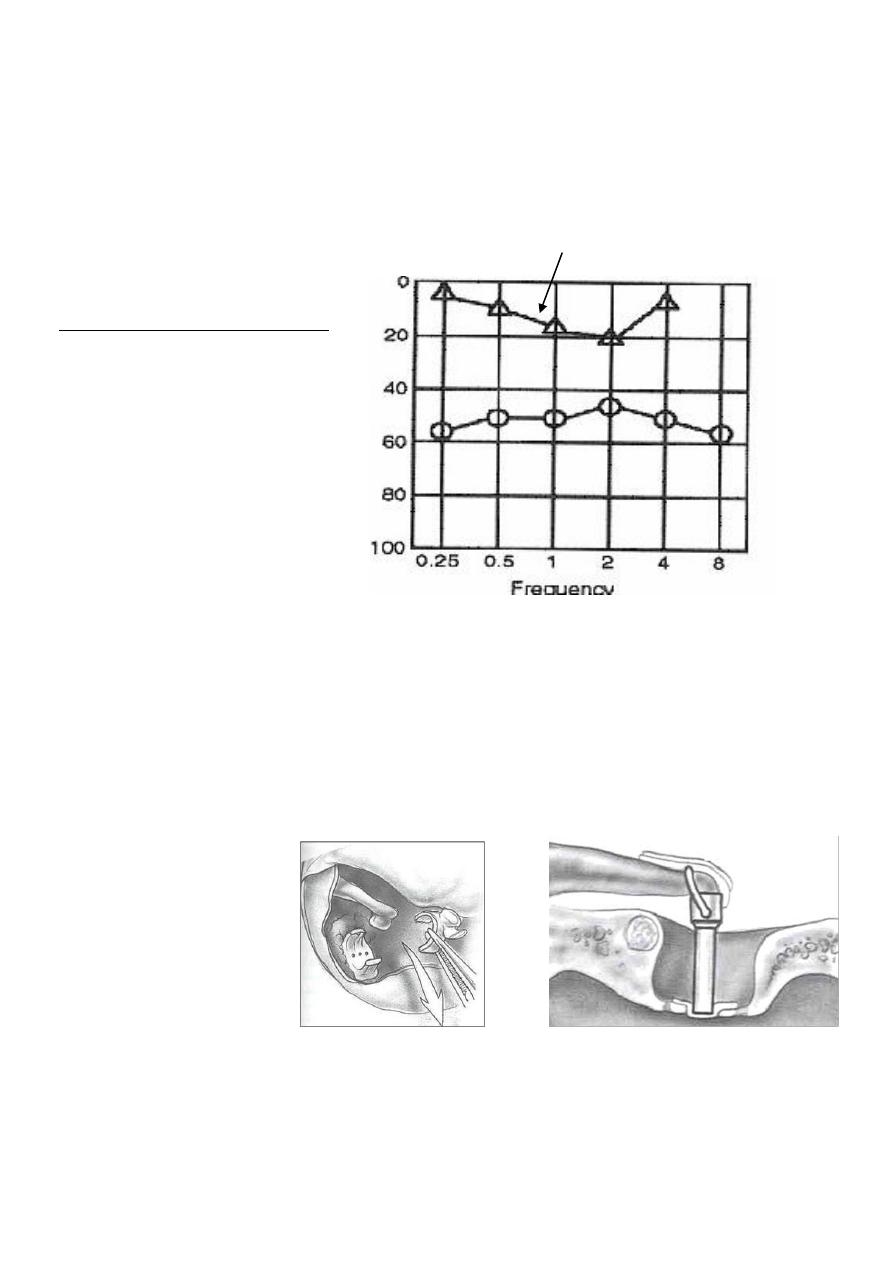
2. Surgical: stapedectomy which is total or partial removal of the foot plate of the
stapes and replacement by prosthesis.
Complication of stapedectomy: perilymph fistula which is characterized by sudden
SNHL and vertigo. It is liable to occur after sudden changes of pressure, so the
patient should avoid diving and only fly in pressurized aircrafts.
3. Hearing aid is an effective alternative.
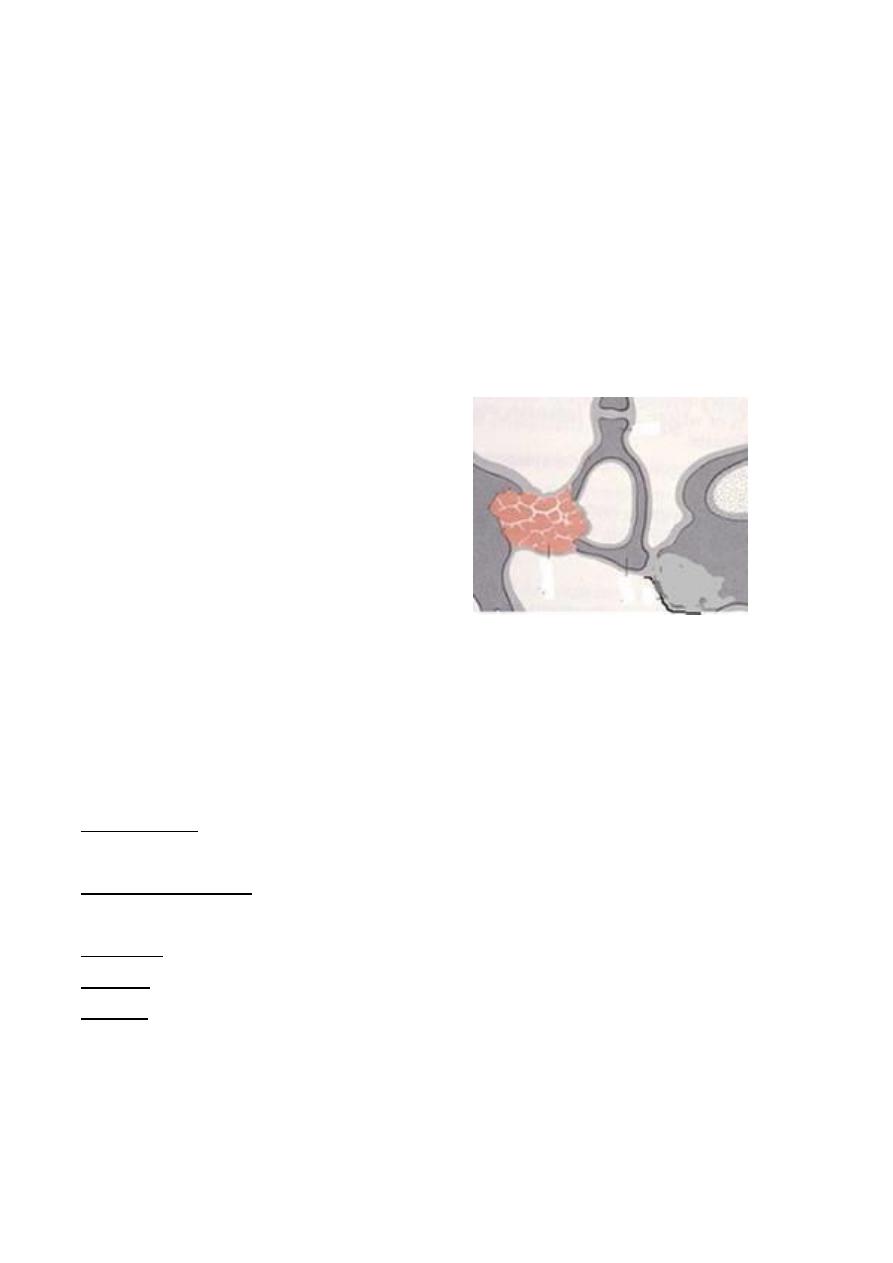
diometric finding
An au
characteristic of otosclerosis
is an increase in bone
conduction threshold with a
peak at 2,000 Hz known as
Carhart’s notch.
In advanced cases there may
be SNHL which is associated
with masses of otosclerotic
bone involving the cochlea.
Carhart's notch
Bone conduction
KHz

5
Sudden Sensorineural Hearing Loss
Deafness that comes on extremely suddenly so that the patient is actually aware of
the moment of onset of deafness.
Aetiology
1. Idiopathic: in 2/3 of cases no cause could be found.
2. Vascular: spasm, thrombosis or haemorrhage of the internal auditory artery.
3. Viral infection: mumps, measles, rubella or Herpes zoster.
4. Head injury with temporal bone fracture, blast injury, and ear surgery as
stapedectomy.
5. Tumors: acoustic neuroma.
Clinical Picture
1. Hearing Loss: The usual story is that the patient awakes in the morning and finds
that he has become deaf.
2. Tinnitus: occur in 80% of cases. It is a good prognostic sign and means that hair
cell still functioning.
3. Vertigo: is common in those with vascular aetiology and caries a bad prognosis.
Examination
1. The TM is usual normal.
2. Tuning fork test….
3. PTA: hearing loss in high frequency.
Treatment
1. Bed rest and sedation.
2. Steroids in tapering dose.
3. Vasodilators: Betahistine (Betaserc) or breathing 5% CO2 in air (carbogen) to
improve the cochlear circulation.
4. Low molecular weight dextran: to lessen sluding of blood in the small vessels of
cochlea.
Prognosis
In 1/3 of patients there is quick recovery from deafness within hours, days or weeks.
If there is no recovery within 3 weeks it is unlikely to occur spontaneously. One third
experience partial recovery and a third have none. A severe high frequency hearing
loss and the presence of vertigo are unfavorable prognostic features.
6
Drug ototoxicity
Damage to the cochlear and/or vestibular part of the inner ear by certain drugs.
Ototoxic drugs include:
1. Aminoglycosides; e.g.; streptomycin
& gentamycin.
2. Loop diuretics; e.g.; frusemide
3. Salicylates.
4. Quinine.
5. Antiepileptics; phenytoin.
6. B-blockers.
7. Cytotoxic; cisplatin.
If two potentially ototoxic drugs are given at the same time, such as Aminoglycosides
and diuretics, their toxic effects may be synergistic. The dangers are especially
great if excretion is impaired as in renal failure.
Treatment
1. Preventive: keep the plasma level in a safe range and avoid or discontinue ototoxic
drugs whenever there are signs of ototoxicity.
2. Therapeutic: hearing aids.
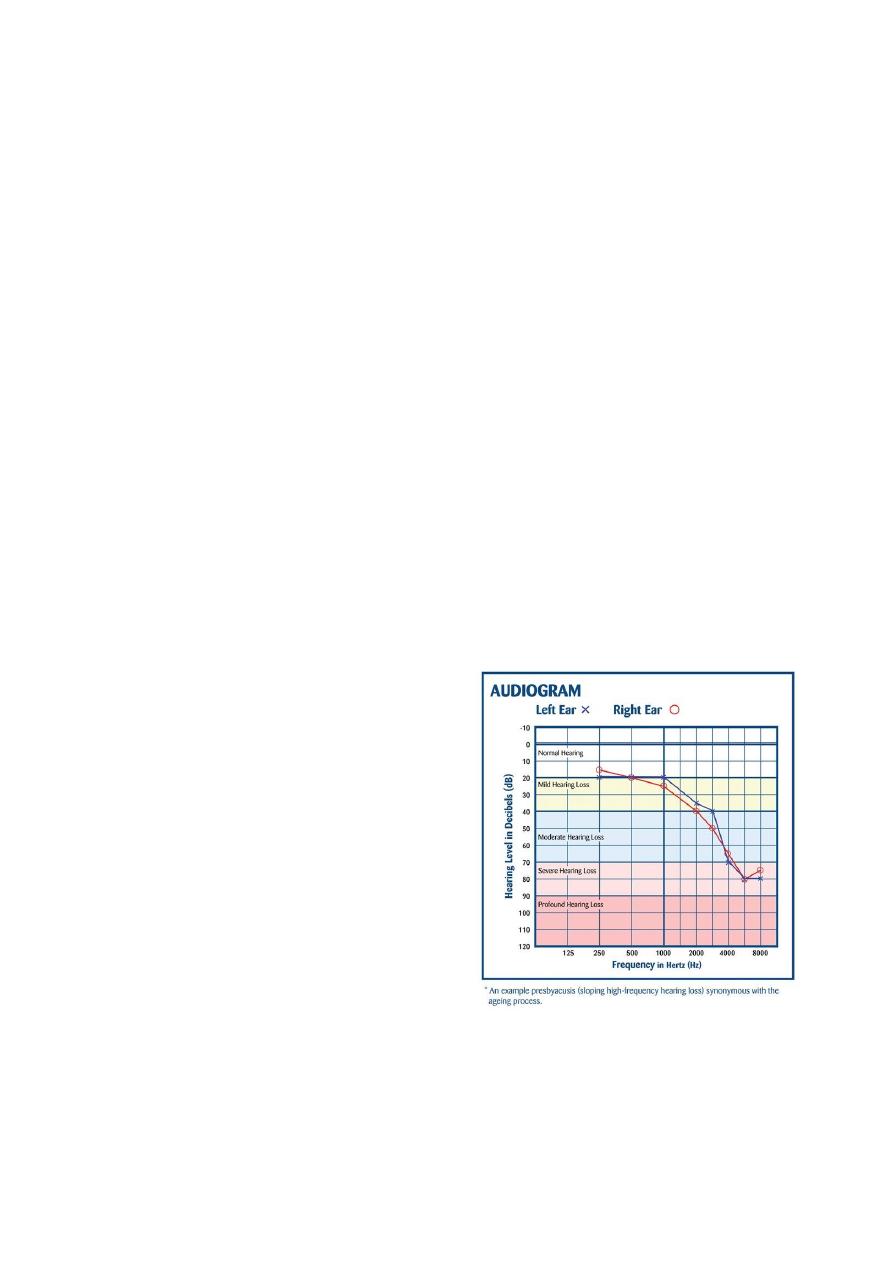
Presbycusis (Senile hearing loss)
A symmetrical bilateral SNHL which occurs after the age of 65 years with no
underlying cause. The degenerative changes occur as a result of aging process,
vascular insufficiency or noise exposure.
Clinical Picture
The deafness is characteristically
progressive, bilateral SNHL with
marked loss of speech discrimination
due to inability to hear the higher
frequencies (consonant sounds). Thus,
the speech is difficult to understand
especially if fast, too loud or in a noisy
background.
Audiometry
Bilateral symmetrical SNHL
Treatment
1- Lip reading and auditory training: It is important to speak slowly, distinctly and
not to shout with these patients.
2- Hearing aids: if the hearing loss is greater than 30dB.
7
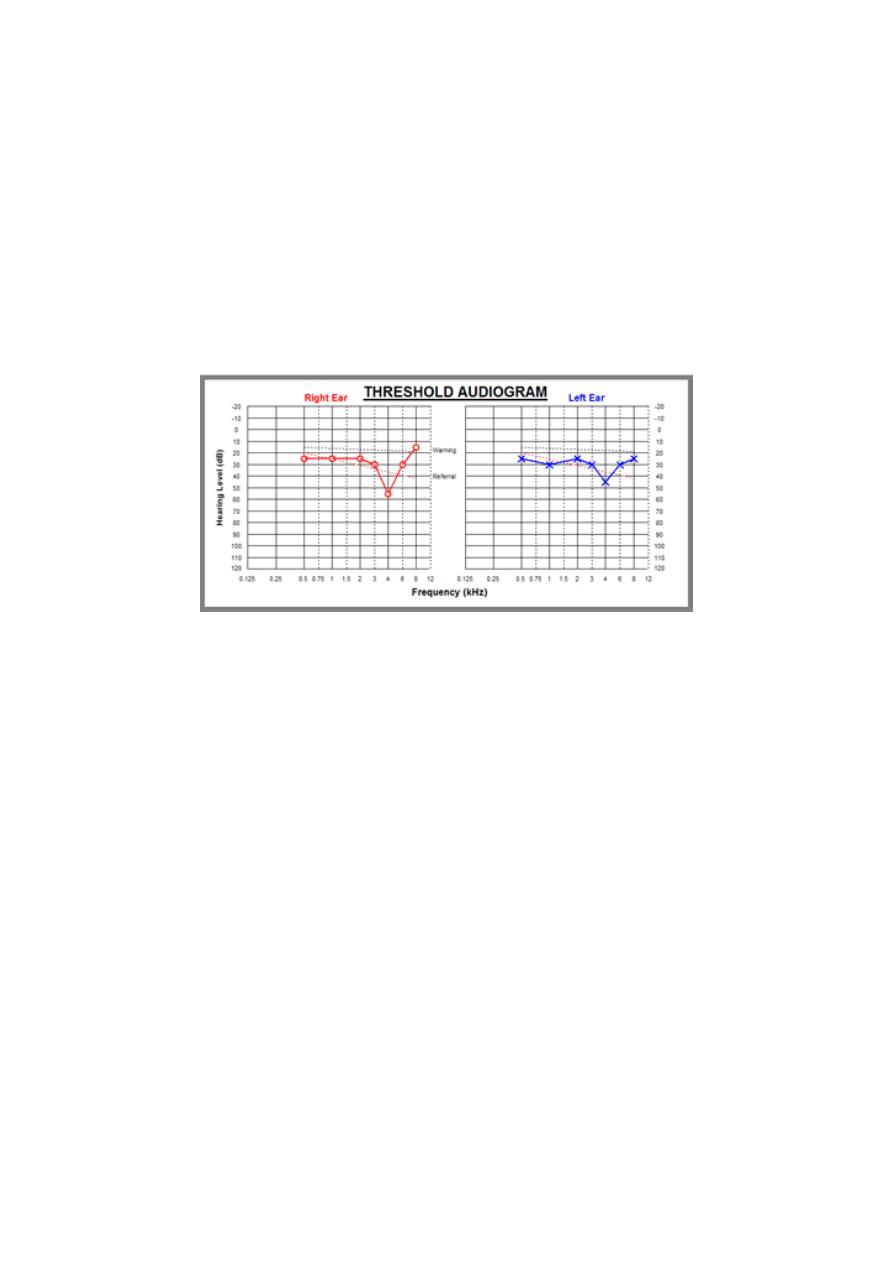
Deafness and Noise
It is deafness that results from excessive sound stimulation. It is of two types:
1- Acoustic trauma: SNHL due to very brief exposure to very loud noise e.g.
gunfire and explosions.
2- Noise-induced hearing loss: SNHL caused by prolonged exposure to loud noise in
certain occupations. A noise level in excess of 85dB for 8 hours/day is to be
regarded as hazardous. Tinnitus is usually a feature.
Audiometry
The earliest change is SNHL at 4 kHz which disappears as the condition deteriorates
and later involves all the higher frequencies.
Treatment
1- Preventive: by using protective ear plugs and screening personnel in noisy
occupation by routine audiometry.
2- Therapeutic:
a. Rest and avoidance of future trauma.
b. Hearing aids and auditory training.
Non-Organic Hearing Loss
It means deafness without organic cause. It is of two types:
1. Psychogenic (hysterical); hear the patient is unaware that he is simulating
deafness. The onset is usually due to some acute stress.
2. Malingering: here the subject is quite aware that his hearing is normal and that
the feigning deafness to avoid some situation of responsibility.
Diagnosis
1. History; certain things do not fit e.g. there may be gross discrepancy between
whispered and conversational vice.

8
2. Examination; clinical examination shows no abnormality but hearing tests show a
great degree of deafness.
3. Audiometry; repeated audiograms give different results on each occasion.
Treatment
1. Psychogenic deafness is treated by psychotherapy.
2. Malingerers are cured once discovered.
Fracture base of skull.
Direct or indirect trauma to the petrus bone may cause fracture (Longitudinal
or transverse).
The longitudinal is more common and it is parallel to the long axis of the petrus
bone.
There may be haemorrhage of varying degree in the cochlea, vestibule or
internal auditory meatus.
Microscopical fractures of the otic capsule often occur in severe head injury
and this may account for permanent type of deafness.
Clinical feature
Deafness: Sensorineural in type usually severe and permanent.
Tinnitus and Vertigo: present at first then disappear.
Tympanic membrane may be intact, sometimes it may be ruptured.
Facial nerve palsy is seen more often in transverse fracture (50%).
X-ray base of skull: May show fracture. Negative X-ray findings do not
exclude fracture.
Treatment
This is decided at first according to the general condition of the patient and
severity of the injury. The following must be considered in the treatment:
Never syringe the ear.
No instrumentation of the ear.
No caloric test.
Systemic antibiotic to prevent intracranial complication.

9
Facial nerve paralysis: delayed onset; conservative treatment while
immediate onset may require surgery in the form of decompression or re-
anastomosis.
Tinnitus
Tinnitus is subjective sensation of noise in the ear or head in the absence of any
relevant external signal. Tinnitus is usually subjective but occasionally objective
(palatal myoclonus and glomus tumor).
Aetiology
I. Central:
1. Hypertension and hypotension.
2. Cerebrovascular disease.
3. Intracranial vascular tumor.
4. Benign intracranial hypertension.
5. Migraine.
II. Peripheral (ear):
A. External and middle ear.
1. Wax.
2. Middle ear effusion.
3. Otosclerosis.
4. Glomus tumor: Rhythmic beating tinnitus synchronized with the pulse.
B. Cochlear:
1. Meniere's disease.
2. Presbyacusis.
3. Ototoxic drugs: aminoglycosides and aspirin.
4. Noise induced hearing loss.
C. Retrocochlear:
1. Acoustic neuroma.
2. Syphilis.
Clinical picture
Tinnitus usually has buzzing, hissing, or ringing quality. It may be intermittent or
continuous. Stress and tiredness often make it worse. It is usually more noticeable in
bed at night when background noise is at its quietest.

10
Investigation
1. Heamatology: CBC, FBS and lipid profile.
2. Radiology:
a. CT scan, MRI (acoustic neuroma).
b. MRA and angiography (glomus jugulare).
3. PTA.
Treatment:
1. Treatment of underlying cause and reassurance. Avoid smoking and caffeine
beverages.
2. Drugs: I.V. lidocaine, antidepressants and anxiolytics like alprazolam. Ginkgo
biloba improves brain function by increasing blood flow and oxygenation.
3. Tinnitus masking: a tinnitus masking is a small electronic generator that
provides noise that is used to mask out a patient tinnitus. Suppression occurs
and this continues even after the device is removed.
4. Hearing aids: are helpful to those who have hearing loss . The awareness of the
background sound will make the tinnitus less apparent.