
1
Fifth stage
Neuro-Surgery
Lec-6
د. عبدالرحمن
2/5/2016
Management of Head Injuries
The key aspects in the management of head injury
Accurate clinical assessment of neurological and other injuries.
Determination of the pathological process involved.
Changes in the neurological signs indicate a progression or change in the pathological
process.
The management planned programme
Dealing with the life saving priorities.
Initial evaluation and examination.
Necessary investigations.
Continuing care and observations.
Possible need for surgery to evacuate an intracranial haematoma.
I. The life saving priorities: (ABC)
1. Protection of the AIRWAY.
2. Maintenance of adequate BREATHING.
3. CIRCULATION.
4. TWO important NOTES:
o Patients are more likely to die from airway obstruction.
o The presence of shock in a patient with a head injury is most likely due to internal
haemorrhage in the thorax or abdomen.
5. Secure the neck and spine
II. Initial evaluation and examination
1. Important points in the History
2. Initial examination
3. Indications for admission to the hospital
a. Important points in the History
Cause, Circumstance and Mechanism of injury.
2
Period of loss of consciousness.
Period of post-traumatic amnesia.
Presence of headache and vomiting.
Level of consciousness at scene and on transfer.
Evidence of seizures.
Probable hypoxia or hypotension.
Pre-existing medical conditions.
Medications (especially anticoagulants).
Illicit (illegal) drugs and alcohol.
b. Initial examination
Vital signs.
Scalp.
Skull.
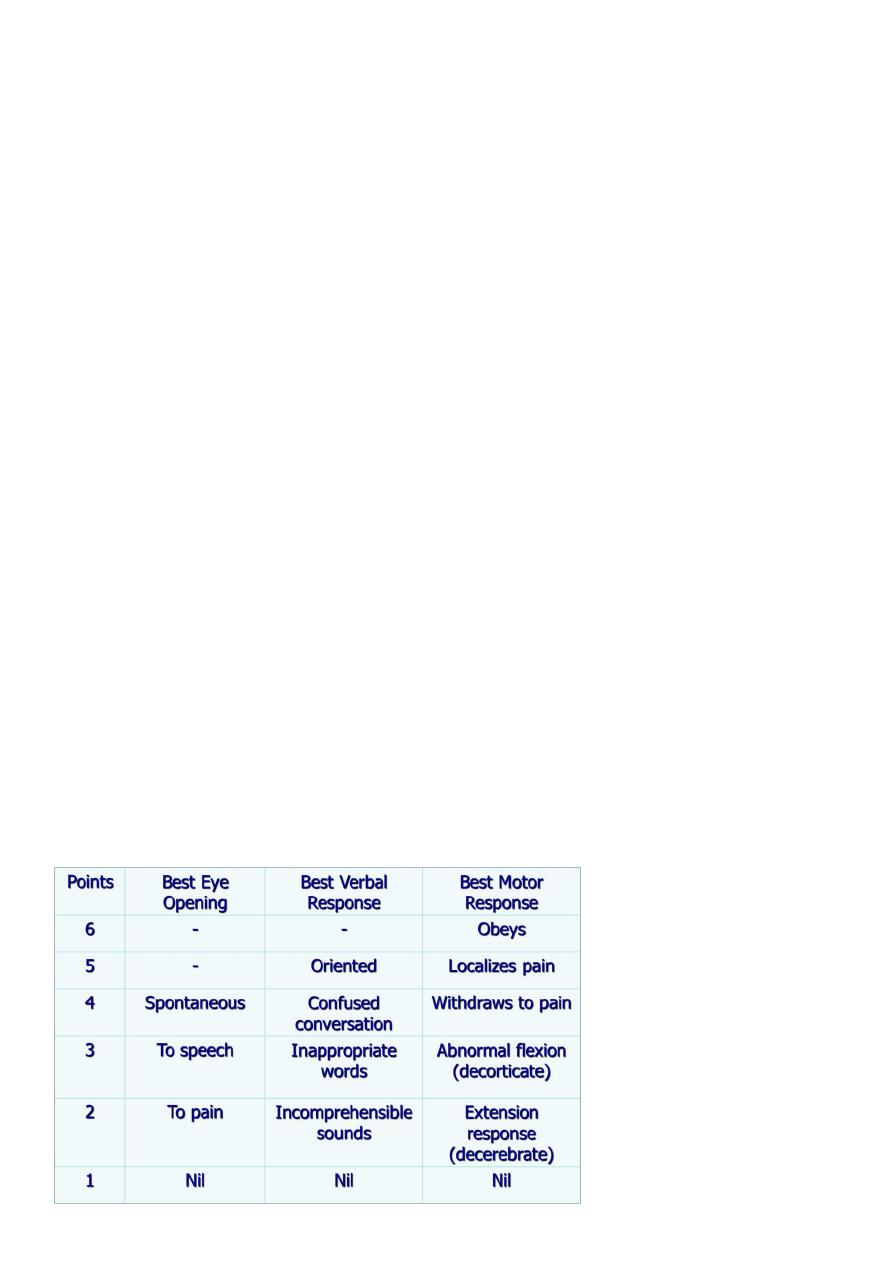
Level of Consciousness: by using “The Glasgow Coma Score”
Pupils: size and reaction to light:
a. Immediately dilated pupil: direct trauma of the orbit or the oculomotor nerve.
b. Pupil dilated later : lateralization due to supratentorial haematoma.
Lateralising signs: Hemiplegia in the acute phase is more likely due to primary cerebral
injury rather than due to a compressing intracranial haematoma.
Signs of base of skull fracture.
Full neurological examination: tone, power, sensation and reflexes.
Limbs: for any fracture or vascular injury.
Chest: examine for fractured ribs, pneumothorax or haemothorax.
Abdomen: examine for internal haemorrhage or peritonitis.
Back: for the possibility of fractures or dislocations of spines.
“The Glasgow Coma Score”

3
C. Indications for admission to the hospital
Any depression of level of consciousness (or any history of loss of consciousness for
more than 5 minutes).
Skull fracture.
Focal neurological sign.
Persistent headache or vomiting.
Patients who are difficult to assess - for example, those who are also intoxicated.
Concomitant diseases or medications that pose increased risk (for example,
coagulopathies and anticoagulants).
Absence of responsible relatives who can observe the patient for the first 24 hours.
III. INVESTIGATIONS
a. Plain skull x-ray:
b. Cervical spinal x-ray
c. CT scan
a. Plain skull x-ray
1. Can demonstrate the site and type of a skull fracture.
2. A foreign body can also be seen.
Indications for skull x-ray in head injury
Impaired consciousness or neurological signs.
History of loss of consciousness, amnesia, or fits.
High speed injury or suspected penetrating injury.
Scalp laceration to bone, large haematoma, or suspected fracture on palpation.
Persisting vomiting or headache.
Loss of cerebrospinal fluid or blood from ear or nose.
Difficulty in assessing the patient (children, drug or alcohol intoxication).
b. Cervical spinal x-ray
To exclude fracture or dislocation of spines
c. CT scan
Done immediately and sometimes need to be repeated.

4
Indications for immediate CT scan in head injury:
Glasgow Coma Score (GCS) <13 at any point.
GCS 13 or 14 at 2 hours.
Focal neurological deficit.
Suspected open, depressed, or basal skull fracture.
Seizure.
Vomiting more than one episode.
Age more than 65.
Coagulopathy (e.g. on warfarin).
Dangerous mechanism of injury (CT within 8 hours).
Antegrade amnesia more than 30 minutes (CT within 8 hours).
Indications to repeat CT scanning
Delayed deterioration in the mental state.
A persistent rise in intracranial pressure (ICP).
Failure to improve over 24 hours.
IV. Continuing Care and Observations
The aims of conservative treatment are:
1. To give the patient the maximum care until spontaneous recovery occurs.
2. To detect at the earliest possible moment the development of complications that
may need surgical interference.
a. Continuous care
Attention to the airway.
A Foley’s catheter: to facilitate the nursing care and to estimate the urine output.
Frequent change of posture to avoid bed sores.
Physiotherapy of the joints and massage to the muscles.
Intravenous isotonic maintenance fluids should be given (crystalloids) until
nasogastric feeding.
Nasogastric tube feeding.
Measures to decrease the intracranial pressure, pay good attention to the following
points:
o Before Mannitol is given it is essential to exclude an intracranial haematoma and
to check that the renal function is satisfactory.

5
o As Mannitol reduces normal brain volume, it will increase the size of extradural
haematoma and so it will increase the mass effect.
o Steroids in severe head injury are associated with increased mortality and should
not be used.
b. Repeated observations
Level of consciousness using the Glasgow Coma Scale.
Pulse, blood pressure, and temperature.
Respiration.
Pupils.
Reflexes.
c. Causes of DETERIORATION of the patient:
BRAIN OEDEMA .
Airway obstruction and/or hypoventilation leading to brain swelling .
Intracranial haematoma.
FEVER due to respiratory infection or meningitis.
Overtransfusion by hypotonic fluid or dehydration.
Epilepsy
V. Surgery to evacuate an acute intracranial haematoma
Once the clinical picture of the patient deteriorates, the possibility of an intracranial
haematoma is raised and it is so important to exclude or verify this because surgical
interference at this stage can save the patient, otherwise progressive deterioration
and fatal herniation of the cerebellar tonsils and medulla through the foramen
magnum will occur.
Long-Term Sequelae Of Head Injury
Neurological deficits: This needs neurorehabilitation by medical, nursing,
physiotherapy and speech and occupational therapy teams.
Post-traumatic epilepsy affect <5% of patients admitted with head injury.
Cerebrospinal fluid (CSF) fistula.
Neuropsychological sequalae: Post-concussion syndrome: is a complex of symptoms
persisting months after head injury and consist of various combinations of headache,
6
dizziness, impaired short –term memory and concentration, easy fatigability,
emotional disinhibition and depression.
Neuroendocrine and metabolic disorders.
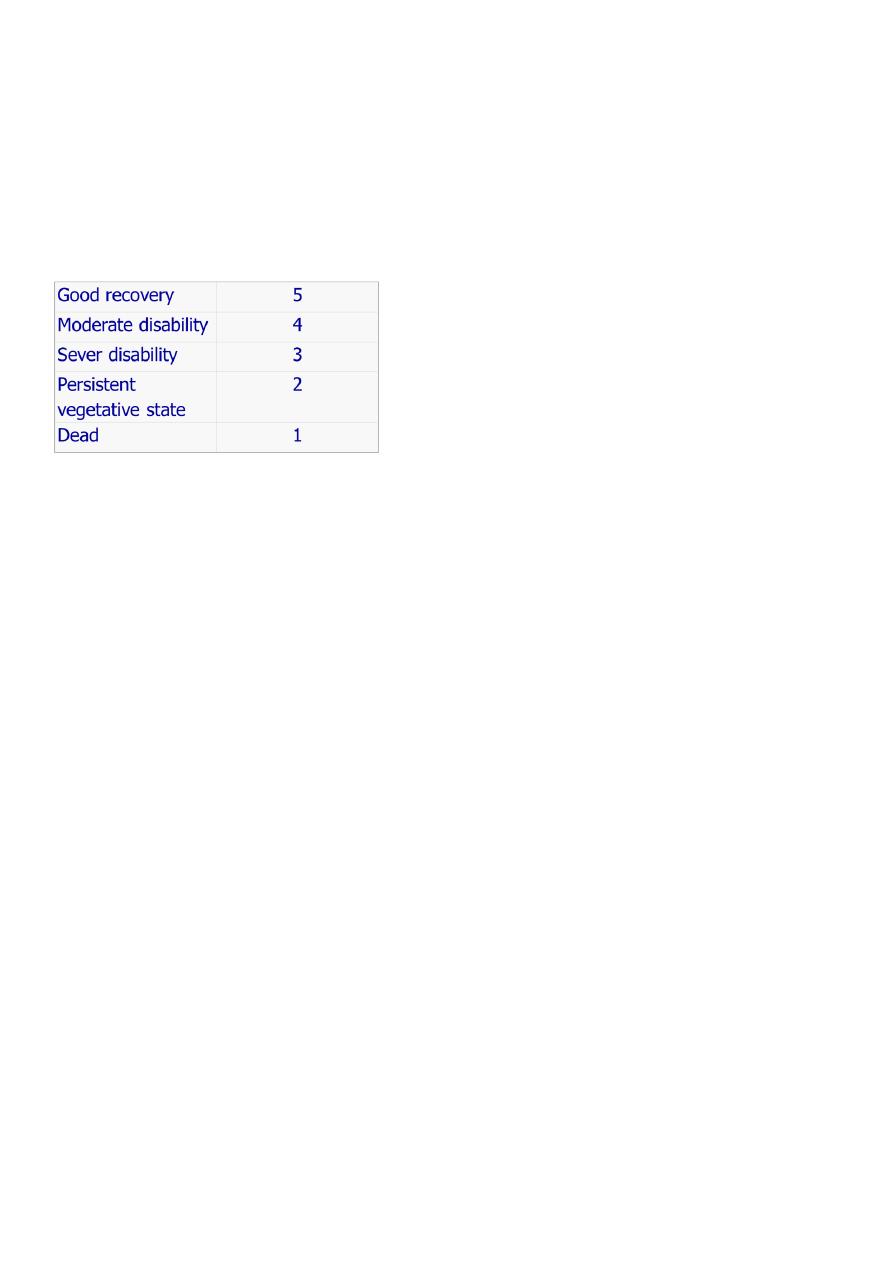
Outcomes after Head Injury
Outcome Scores: (The Glasgow outcome Score (GOS))
The Glasgow outcome Score (GOS)
GCS 5: independent functioning and possibility of returning to work even if deficit is
present.
GOS 4: remain independent though with a disabling deficit.
GOS 3: dependent on others for at least some of their care.
GOS 2: no awareness of themselves or their environment.
Head injury - DON'T FORGET
Changes in the Glasgow coma score are often of more importance than the absolute
score - monitor regularly.
Beware associated injuries - manage severe head injuries as multiply injured patients
until other injuries are excluded.
Stabilize the neck.
Beware intoxication with alcohol or drugs.
Record keeping beyond reproach.
If in doubt, ADMIT.