BENIGN TUMORS OF UTERUSUterine fibroids
Dr. Ahmed jasimAss.Prof.
MBChB-DOG-FICMS
COSULTANT OF GYN. & OBST.
Definition
A uterine fibroid (also uterine leiomyoma, myoma, fibromyoma, leiofibromyoma, fibroleiomyoma, and fibroma) (plural of ... myoma is ...myomas or ...myomata) is a benign (non-cancerous) tumor that originates from the smooth muscle layer (myometrium) and the accompanying connective tissue of the uterus.Fibroids are the most common benign tumors in females and typically found during the middle and later reproductive years. While most fibroids are asymptomatic, they can grow and cause heavy and painful menstruation, painful sexual intercourse, and urinary frequency and urgency. Some fibroids may interfere with pregnancy although this appears to be very rare.
Prevalence
Uterine fibroids Present in up to 25% of women of reproductive age.Fibroids are most common in women aged 30-40, but they can occur at any age.
Fibroids occur more often in black women than in white women.
They associated with nulliparity and more common in women with family history of fibroids and obesity.
The incidence is decreased with:
Prolonged use of the oral contraceptive pill .Prolonged use of Depo-provera.
increasing numbers of term pregnancies.
smoking.
Fibroids regress in size and undergo degeneration after the menopause.
Aetiology and pathogenesis
The exact causes of fibroid are not well understood but research and clinical experience point to several factors:
Genetic alterations. Many fibroids contain alterations in genes that code for uterine muscle cells.
Hormones. Estrogen and progesterone, two hormones that stimulate development of the uterine lining in preparation for pregnancy, appear to promote the growth of fibroids. Fibroids contain more estrogen and estrogen receptors than do normal uterine muscle cells.
Other chemicals. Substances that help the body maintain tissues, such as insulin-like growth factor, may affect fibroid growth.
Fibroid location
Intramural Fibroids are located within the wall of the uterus and are the most common type; unless large, they may be asymptomatic. Intramural fibroids begin as small nodules in the muscular wall of the uterus. With time, intramural fibroids may expand inwards, causing distortion and elongation of the uterine cavity.Subserosal fibroids are located underneath the mucosal (peritoneal) surface of the uterus and can become very large. They can also grow out in a papillary manner to become pedunculated fibroids. These pedunculated growths can actually detach from the uterus to become a parasitic leiomyoma.
Submucosal fibroids are located in the muscle beneath the endometrium of the uterus and distort the uterine cavity; even small lesion in this location may lead to bleeding and infertility. A pedunculated lesion within the cavity is termed an intracavitary fibroid and can be passed through the cervix.
Cervical fibroids are located in the wall of the cervix (neck of the uterus). Rarely fibroids are found in the supporting structures (round ligament, broad ligament, or uterosacral ligament) of the uterus that also contain smooth muscle tissue.


Tumors in subserosal and intramural locations comprise the majority (95%) of all fibroids while submucous fibroid comprise 5%.
M.Emam
Leiomyomata Uterus
Pathology
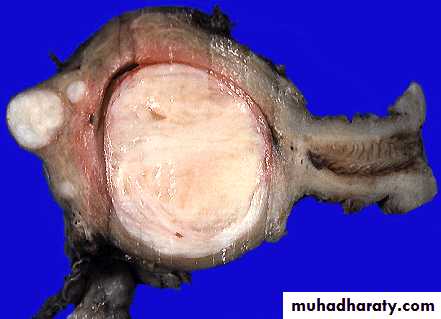
Leiomyomas grossly appear as round, well circumscribed (but not encapsulated), solid nodules that are white or tan, and show whorled appearance on histological section. The size varies, from microscopic to lesions of considerable size. Typically lesions the size of a grapefruit or bigger are felt by the patient herself through the abdominal wall.

Microscopically, tumor cells resemble normal cells (elongated, spindle-shaped, with a cigar-shaped nucleus) and form bundles with different directions (whorled). These cells are uniform in size and shape, with scarce mitoses. There are three benign variants: bizarre (atypical); cellular; and mitotically active.

Clinical features
symptomsIt depened on the size, location, and number of tumors.
A. Asymptomatic:
Most fibroids (50%) not cause any symptoms& accidentally discovered on abdominal or pelvic examination or during ultrasound examination.
B. Symptomatic:
About 20–50% of women with fibroids present with symptoms.(1). Abnormal uterine bleeding ;include
Menorrhagia (Heavy menstrual bleeding)
is usually caused by intramural fibroids or submucosal fibroids.
Intermenstrual bleeding , mainly in pedunculated submucosal fibroid
Postcoital bleeding, mainly in pedunculated submucosal fibroid
(2). Pressure symptoms:pressure on surrounding structures.
1.Urinary bladder:Urinary frequency.
Incontinence.
urine retention.(rarely)
hydroureter or hydronephrosis
2.Venous system;
varicosities, lower extremity edema, hemorrhoids.
3.nerves that supply the pelvis and the legs, causing pain in the back, flank, or legs.
(3). Pain:
Pain occurs in approximately 30% of women with uterine fibroids.Feeling of pelvic heaviness that can radiate to the back or lower extremities.
Congestive Dysmenorrhea
Dyspareunia.
Causes of pain in fibroid
Torsion of a pedunculated fibroids.*Prolapse of pedunculated submucosal fibroids.
* Red degeneration.
* Infection.
* Sarcomatous changes (Malignant changes).
* Adhesion
(4).infertility; (less than 3% of cases).
It Compromise of the patency of the fallopian tube.A.Large intramural tumors located in the cornual regions may obstruct the tubes.
B. intraligamentous fibroids may cause tubal obstruction.
Distortion of the endometrial cavity and Continuous bleeding in patients with submucous fibroids may impede implantation.
5. A palpable abdominal-pelvic mass and abdominal swelling.
6. Malignant changing Transformation to uterine leiomyosarcomas is extremely rare (0.1% ).
It must always be suspected when the following signs are present:
A. Enlargement of the uterus in postmenopausal patients.
B. Rapid changes in size and consistency of the tumor.
C. Ascites and recurrence after surgery.
Signs
The signs depends on type, size ,number, any changes of fibroids.By Abdominal examination:
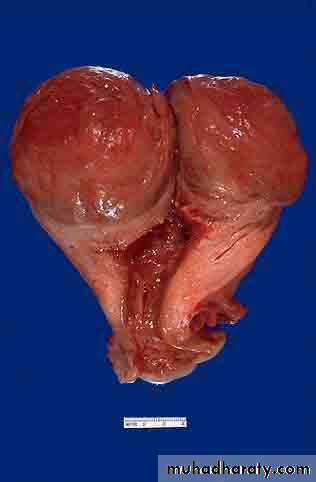
Very large fibroids can cause abdominal distension and can be palpated abdominally as irregular nodular tumor firm mass arising from pelvis.
Those smaller than 13 weeks gestational size are usually confined to the pelvis (abdominally not palpable).
).
Pelvic examination
By speculum examination ,Polyp coming out cervical os can be seen.Bimanual examination show uterine enlargement. The mass felt to be part of the uterus usually with some mobility.
Uterine enlargement:
Symmetrically enlarged uterus (submucosal fibroid).
Asymmetrically enlarged uterus(subserous fibroid).
25
Degeneration

Hyaline degeneration
Cystic degeneration
Red degeneration
Sarcomatous change
The others:fat degeneration
calcification
the secondary infection
Result from the diminished
vascularity of the
connective-tissue element
26
Red Degeneration
Occasionally seen as a complication of pregnancy(during pregnancy or immediate postpartum period)
The pathogenesis is unknown,may be the result of the accumulation of blood in the tumour because of venous obstruction.
The cut surface resembles raw meat.
Clinical features:a cause of pain(acute)
fever
rapid growth,tender
产褥期
27
Here is a very large leiomyoma of the uterus that has undergone degenerative change and is red (so-called "red degeneration"). Such an appearance might make you think that it could be malignant. Remember that malignant tumors do not generally arise from benign tumors.
28
Sarcomatous Change
Rare:0.4%~ 0.8%
More common at 40~ 50 years old
Usually occur in intramural fiboids
grow quickly
vaginal bleeding
Differential Diagnosis
Pregnancy.Ovarian tumors
Adenomyosis.
Tubo-ovarian abscesses.
Endometrial cancer.
Liomyosarcoma .
Congenital anomalies of the uterus.
Investigations
1.gynecologic ultrasonographyI.transabominal and/or transvaginal ultrasound
A..identify uterine fibroid or any mass.
B.Assess uterine dimension
C.Location of fibroid.
II.Sonohysterography (saline infusion sonography):
inject a small amount of saline into the uterine cavity so
that the lining of the uterus can be seen,
Tumors sitting inside of the cavity can be readily seen.
2. Hysterosalpingography (HSG).
helpful specifically in the evaluation of lesions that affect the uterine cavity
3. Magnetic resonance (MR) imaging
It is expensive and not used routinely. Only use if there is any doubt about the nature of a fibroid mass.
4. Hysteroscopy
5. Laparoscopy6. Endometrial Sampling
performed to evaluate abnormal bleeding in patients who are at risk for endometrial polyps, hyperplasia, or carcinoma.
7. Immaging of renal tract: may be helpful in patient with large fibroids to excluded hydronephrosis
Treatment
Most fibroids do not require treatment unless they are causing symptoms. After menopause fibroids shrink and it is unusual for fibroids to cause problems.Symptomatic uterine fibroids can be treated by:
1.medication to control symptoms
2.medication aimed at shrinking tumours
3.ultrasound fibroid destruction
4.various surgically aided methods to reduce blood supply of fibroids
5.myomectomy or radio frequency ablation
6.hysterectomy
Treatment must be individualized according to:
Patient (age-parity-symptoms).
Fibroid (number-size-type-rate of growth).
Complications associated with fibroids.
Expectant Management:
Approximately 80% of fibroids are asymptomatic and are smaller in size than a twelve week gestation uterus do not need to be removed and may be followed clinically. Observation with periodic examination (every 3 to 6 months) is appropriate to rule out a rapidly growing uterine sarcoma. After assurance of slow growth or stable uterine size, annual follow-up may be appropriate.Medical treatment
1.medication to control symptomsTreatment of symptom as menorrhagia
GnRH agonists;
It induce a hypoestrogenic pseudo-menopausal state and causes shrinkage of the fibroids .
GnRH agonist treatment is not recommended for longer than 6 months because of the potential consequent development of osteoporosis.
Side effect; hot flashes and osteoporosis.
Side effect; hot flashes and osteoporosis.
Re-growth of fibroids is experienced within a few months, and for this reason its use is recommended for short-term treatment in selected cases which are:1.Treatment of women approaching menopause in an effort to avoid surgery.
2. Short-term therapy may be used preoperatively (at any age) in the following situations:
A. pre-surgical treatment to decrease symptoms and size which might make surgery easier or permit a more conservative approach such as a vaginal or laparoscopic surgical approach rather than abdominal approach
B. control bleeding prior to surgery (so that anemia might be corrected).
Levonorgestrel intrauterine devices
Danazol
Magnetic Resonance-Guided Focused Ultrasound
C. Surgical Treatment
There are two general types of surgery available for fibroids and its choice depends on:Patients wishes and parity
Fibroid size and number
Location of the fibroids.
Myomectomy
Polypectomy.Hysterectomy.
Myomectomy
Involves the removal of single or multiple fibroids while preserving the uterus.Myomectomy may be performed in a number of ways. The method used depends on the location and size of the fibroids.
1. Laparotomy (Abdominal myomectomy)
2. Laparoscopic myomectomy.
3. Hysteroscopic myomectomy (submucosal fibroids).

Complications of myomectomy
1.Abdominal myomectomy has been associated with more significant blood loss.2.Abdominal myomectomy has been associated with higher morbidity than hysterectomy.
3.The risk of recurrence after myomectomy has been estimated to be 27% after 10 years.
4.With larger fibroids, attempted myomectomy frequently results in hysterectomy due to uncontrollable bleeding in these highly vascular tumors.
5.if the endometrial cavity is entered during myomectomy , future deliveries must be by caesarean section.
B) Hysterectomy
It is a definitive therapy for uterinefibroids. (The only real "cure" for fibroids).
Hysterectomy may be considered when:
Pain or abnormal bleeding persists.
Fibroids are very large.(uterus is large >12-14weeks)
Other treatments are not possible.
A woman no longer wants children.
A rapid growth of the uterus caused by fibroids

Approach of hysterectomy:
Abdominal hysterectomyVaginal hysterectomy.
Laparoscopically assisted vaginal hysterectomy.
D). Uterine Artery Embolization:
Is a promising new method of treating symptomatic fibroids. In this procedure, Embolization of the uterine arteries supplying the fibroids.
Uterine Fibroids and Pregnancy
A small number of pregnant women have uterine fibroids.Effects of pregnancy on fibroid:
• Enlarge .• Become softer ,flatten out and become indistinct.
• May be mistaken for fetal parts.
• Certain accident and degenerations are more common in fibroids during pregnancy:
• Red degeneration of fibroids. occur in 5-10% of women with fibroids..
• Torsion of pedunculated fibroids.( more in puerperium).
• Infection in fibroids after delivery or abortion.
Effects of fibroid on pregnancy:
Fibroids can increase the risk of :
Large for date uterus
Abortion.
preterm labour
abruption placenta.
Fetal malpresentation.
Obstructed labour.
Increase incidence of caesarean section.
retained placental tissue.
Increase risk of post partum haemorrhage (PPH).
Delayed involuation of uterus
Usually no treatment of fibroids is needed during pregnancy. Myomectomy should not be performed in pregnant women because of the increased risk of uncontrolled bleeding.