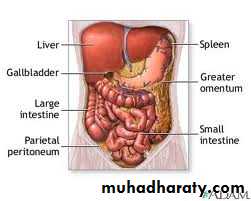
Peritoneum
It is a single layer of flat mesothelial cells resting on a bed of loose connective tissue .Divided to two part :
- parietal
- visceral
Innervations
The parietal is sensitive and innervated by both somatic and visceral afferent nerves.The anterior parietal is most sensitive.
The visceral receives innervations only from autonomic nervous system and is reletively insensitive .
Generalised septic peritonitis
Aetiology :m.o like E-coli ,aerobic and unaerobic strep. , bacteroids ,staph and pneumococci.Source of infection
1- Local spread:- infected organ: appendicitis
- leaking organ: perforated PU, anastamotic leak, extravasated urine.
2- Direct entry:operation
3- Blood spread:septicemia
4- Primary peritonitis :child,female,unknown .str. And pneumococci.
Pathology
Inflamed area become opaque and fibrin deposit.
Purulent exudate accumilate.
Paralytic ileus as a reflex
Fate depends on
Virulance of m.oEffect of treatment
Resistance of the body
Resolution
Localization: abscess.Flaring up(generalized)
Septicemia
Factors predispose to generalized peritonitis
High virulance m.oSudden perforation of viscous
Persistnt source of infection
Stimulation of peristalsis by e,ating,enema
Rough handling of localized collection during surgery
Immune suppretion (AIDS,STROID,D.M)
children ,elderly
Clinical picture
Increase pain at site of pathology with movement .
Vomiting
Abdominal distention
Constipation but in pelvic abscess diarrhoea
Examination
Patient looks ill ,fever ,tachycardia, distressed, avoid movementAbdominal distention , tenderness ,rebound T.
Negative bowel sounds
Advanced condition leads to sunken eyes , septic shock
Investigations
Blood pictureRadiology (gases ,air under diaphragm)
U/S
Diagnostic peritoneal lavage
Treatment
Preoperative :- NG suction
- I.V. Fluid
- Antibiotics
- Analgesia
-Urinary catheter
Surgery
UGA
Mid line or paramedian
Pus send for C/S
Dealing with the pathology(appendix,D.U)
Peritoneal toilet
Drainage
Post operative care
Continue antibioticsI.V fluid
NG suction
Chart for assessment
Prevent septicemia
Localized intraperitoneal abscess
Has better prognosis than generalized peritonitis.Indicate proper defense mechanism
Common sites of collection
RIFLIF
Pelvis
Subphrenic and subhepatic.
Iliac abscess
In the RT side : A. Appendicitis ,perforated D.UIn the left side: perforated diverticulitis ,Ca. colon.
In both sides :from genital organs ,perforated DU
Clinical picture
Pain, swelling, hectic temperature ,vomiting,constipation.O/E :tenderness ,rigidity or gaurding over site of abscess .
Investigation
Blood examination show leukocytosis.U/S
C T ,MRI
TREATMENT
Drainage of pusControlling the cause
Antibiotic
_ drainage should be done extraperitonealy through muscle cut incision.
_ percutaneous drainage under U/S or CT guide is preferable .
_ appendisectomy (interval)12 weeks

Pelvic abscess
Collection of pus in the recto-vesical pouch or Doglas pouch.Causes :
- Acute appendicitis
- localization of resolving diffuse peritonitis
- pelvic inflammatary disease in female
Clinical picture
Hectic temp.Deep pelvic pain
Diarrhea due to irritation of the rectum
Burning micturition ,friquency due to bladder irritation.
Suprapubic mass.
Rectal examination fullness ,tenderness in front of rectum
If neglected may rupture to rectum or vagina

Treatment
Drainage ,antibioticsIf abscess is pointing in rectum =trans – rectal
If in vagina = trans- vaginal through the post fornix
If suprapubic mass extraperitoneal drainage
Rectal drainage better than suprapubic drainage
Subphrenic abscess
Further divided to subhepatic and suprahepatic.the falciform ligament divide it to RT and LT.Sub- phrenic space
1- Right supra hepatic space :between R. leaf of diaph. And the sup. And ant. Surface of the liver. Medially falciform ligament.2- Right infrahepatic (hepato renal pouch of Morison):
above and ifront:the liver and GB
below and behind: upper pole of kidney ,lower part of RT suprarenal gland, 2nd part of the duodenum.
3- RT extra peritoneal space: between bare area of liver and the diaphragm.
4- Lt suprahepatic space:between diaph. Above and the stomach , spleen below.5- LT ant. Infrahepatic space :liver above ,stomach and lesser omentum below and behind.
6- LT post. Infrahepatic: liver above ,stomach anteriorly, pancrease posteriorly.
7- LT extra peritoneal space :around the upper part of the left kidney
Aetiology
Residual pus collection from generalized peritonitis.
Perforated viscous.
Lymphatic spread from chest infection.
Post operative collection(bile, blood).
Clinical picture
Eigastric Pain may referred to shoulder.Hectic temp.
Tachycardia .
Anorexia, vomiting, sweating and wasting.
Persistent hicough
Examination
Inspection : diminished chest wall movement with respiration and rarely bulging upper abdomen.Palpation :- tenderness below costal margin.
- rigidity on upper abdomen
- downward displacement of the liver and upward displacement of apex beat.
Percussion :
- dullness of the pleural effusion- resonance in the gas of abscess
- dullness of the liver and the pus of the abscess
Auscultation : impaired air entry over the lung base .
Investigations
1- WBC count2- CXR shows:
-thickened elevated diaph.
- pleural effusion
- air under diaph.(gas forming)
3- U/S
4- CT
Treatment
If conservetive treatment failed ,Drainage by aspiration extraperitoneal or extrapleural better.
1-post. Extraperitoneal by excision of 12th rib +drain
2- ant. Extraperitoneal by incision subcostal.
3- aspiration under CT or U/S guide .
4- open drainage .
TB peritonitis
Secondary to primary focus that reach the peritoneum :1- direct spread from L .N. ,salpingitis ,enteritis.
2- blood spread from pulmonary TB
3- lymphatic spread from pleura to bowel.
Pathology
1- Acute type: the peritoneum studded with tubercles, straw color exudates.
2- Caseous :also tubercles ,multiple collections, cold abscess , sinus.
3- Ascetic type:(commonest)also tubercles , straw color fluid ,thickened greater omentum,fibrous.
4- Encysted type(localized ascetic type).
5- Adhesive type: adhesions leads to I. O.
Clinical picture
Children,young adultAbdominal pain ,distention,vomiting.
High fever, anorexia, night sweating
Palpable swelling,ascitis.
Tenderness ,guarding may be.
Mass of rolled omentum above umbalicus.
PV. May reveal pelvic mass.
Investigation
CBP and ESRTuberculin test Positive.
CXR
U/S
Ascetic fluid aspiration
Diagnostic laparoscopy, biopsy
Exploration laparotomy
Treatment
Medical anti TB like INH, Rifadin
Surgery for Intestinal obstruction
Ascitis
Pathological accumulation of fluid in the peritoneal cavity. It can be diagnosed clinically when >1500 ccCauses
General causes:-liver ,cardiac, renal and nutritional diseaseLocal:- TB peritonitis, malignancy,chylous ascitis or pancreatic ascitis
Rare :- Meig’s syndrom(ovarian fibroma)- pseudomyxoma peritoni
Peritoneal tumors
1- Carcinoma peritonea: pathologyimplantation from stomach, colon,overy.
peritoneal nodules, bloody fluid
Treatment :
Radioactive gold intraperitonealy
Pseudomyxoma peritoni
Causes :- rupture of pseudomucinous cyst of the overy.-rupture of mucocele or mucoid carcinoma of the appendix
Pathology
Abdomen full with jelly like material,Clinically : abdomen distended with multiple masses
Treatment :- laparatomy and removal of the material and the primary pathlogy.
- liable for recurence.
Mesothelioma
Primary neoplasm of the peritoneum .either present with ascitis or abdominal mass.
Mesenteric cyst
Collection of fluid between 2 layers of small bowel mesentry.2 type:1- False mesenteric cyst: - no epithelial lining like blood cyst due to trauma or caseating L N (cold abscess)
2- True cyst:- chylolymphatic cyst
- enterogenous cyst
- teratomatous dermoid cyst
- hydatid cyst
Clinical picture
Abdominal mass,pain,vomiting,dyspepsia
The site near the umbalicus
Moved in one direction
Dull on percussion
Treatment : excision
Mesenteric lymphadinitisCommonest cause of acute abdominal pain in children
Causes : unknown, viral following respiratory tract infection
Clinical picture
Affect childrenUpper abdominal pain and localized to RT side
Pain colicky ,nausea, vomiting, anorexia and fever.
On examination
GuardingTenderness
PR tenderness positive
Shifting tenderness
Treatment : conservative and in doubtful cases appendicectomy
The retroperitoneum
Bounded by post. Perit. Anteriorly and spine and post. Abdominal muscles posteriorly.Superiorly the 12th rib and the diaphragm and inferiorly the pelvis.
Retroperitoneal tumors
1- Renal ,adrenal gland tumors and L N2- Retroperitoneal sarcoma
presented with mass (abdominal),pain,uretric obstruction and hadronephrosis.
Dx : CT,MRI,u/s.
Treated by surgery,radiotherapy as pallative .
3- Retroperitoneal lipoma