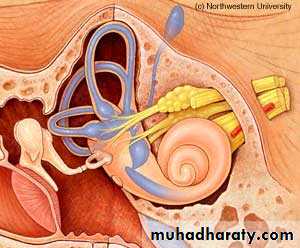
وهو الذي جعل لكم السمع والابصار والافئدة قليلا ما تشكرونINNER EAR
د. هيثم النوري
FIBMS- ENT
Vertigo
Hallucination of movement.It includes sensation of rotation, linear motion and tendency to stagger to one side.
Cortical representation of balance in the brain is very small leading to difficulty of the patient to describe his complaint.

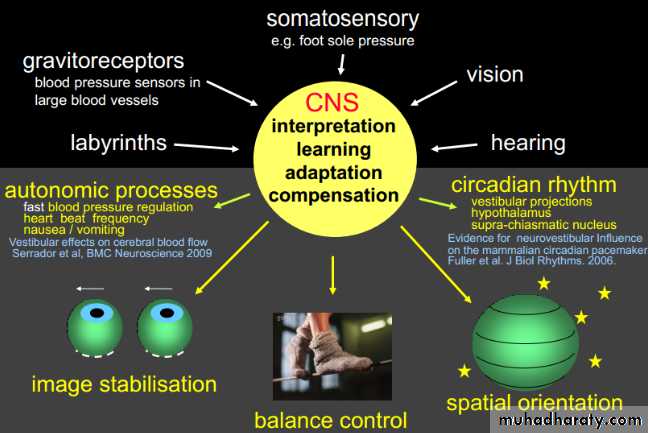
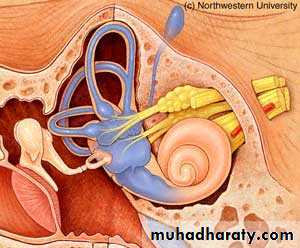
Physiology of vestibular system
Normal balance is maintained by visual, vestibular and proprioceptive stimuli.These are integrated and modulated in the brain stem, cerebellum and higher cortical centers.
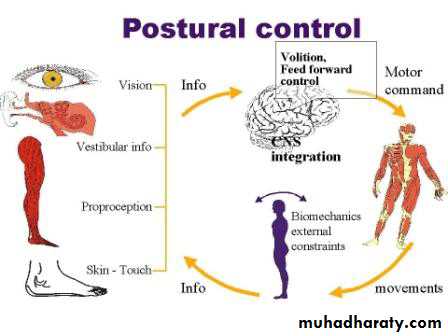
Physiology of vestibular system
Peripheral vestibular lesions
Affect labyrinth or vestibulardivision of VIII nerve.
Produce severe vertigo
and nystagmus,Nausea, vomiting
and sweating.Nystagmus is horizontal
or rotatory.Central vestibular lesions
Affect brainstem nuclei ortheir connections.
Produce severe postural
imbalance with minimal
vertigo and nystagmus.
Nausea and vomiting are
infrequent.Nystagmus is vertical or
horizontal or sometimes absent.Dizziness is light headedness NOT associated with sensation of movement of environment. It is not a vestibular symptom.
Vertigo is the symptom of vestibular system impairment whereas the sign is nystagmus.

Benign Paroxysmal Positional Vertigo BPPV
Recurrent short lived attacks of vertigo provoked by certain critical positions of the head.There are NO other aural or neurological findings.
Aetiology
Idiopathic.
Head injury.
Viral infection.
Degenerative ( aging).
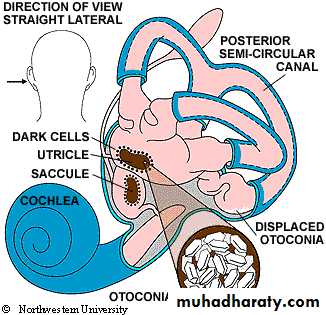
Patho-physiology
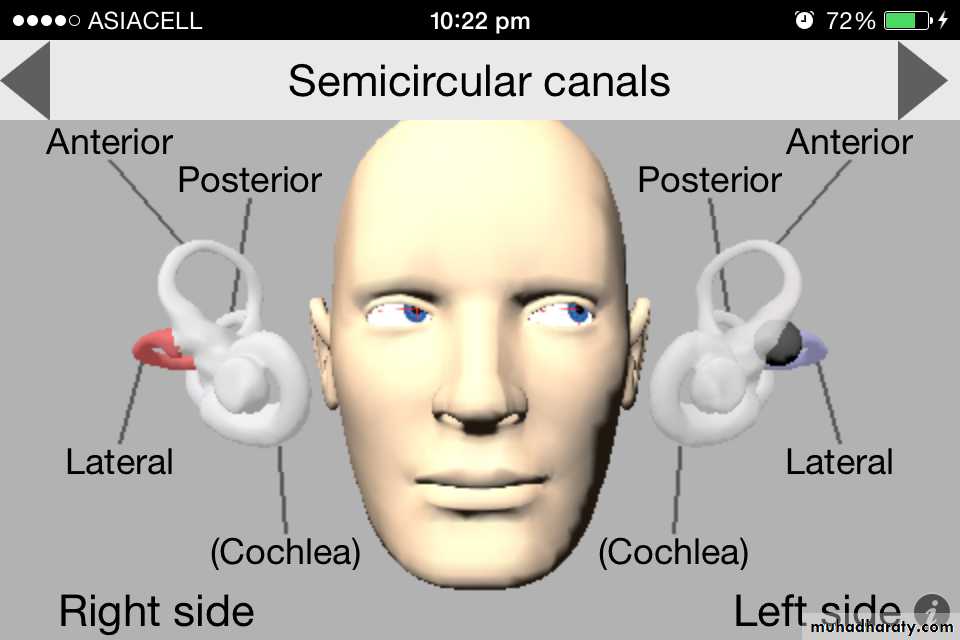
The disease is thought to be due to displacement of otoliths (calcium carbonate particles) from the utricle and saccule to the copula of the posterior semicircular canal ( copulo-lithiasis).

Clinical picture
Brief attacks of severe vertigo with any head movement but specially when rolling in bed and putting the affected ear down.After vertigo subsides patients complain of dizziness and/ or disequilibrium for hours or even days. Hearing is normal and there is no tinnitus.
Typically vertigo recurs for few days and then subsides spontaneously or with treatment for months or years.
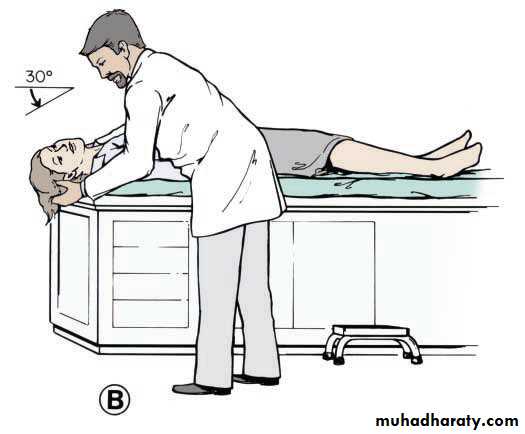
Examination
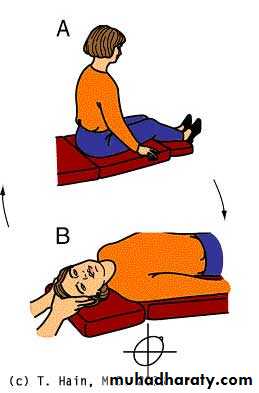
Diagnosis is clinical and supported by normal otoscopy and audiometry.Dix-Hallpike test.
The classical features are horizontal or rotatory nystagmus which has latency for few seconds and duration of less than one minute. It is fatigable when repeating the test.

Treatment
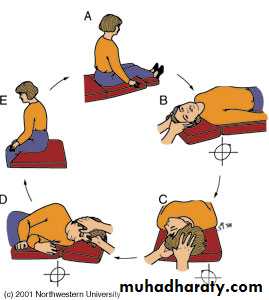
Reassurance and avoidance of the provocating position.Epley's maneuver: it is particle repositioning maneuver, it has high success rate.
Cinnarzine (stugeron) and betahistine (betaserc) have limited value.
Posterior semicircular canal denervation for resistant cases.
Epley's maneuver

Prognosis
Usually the attack is self-limiting within few days. There is tendency for recurrence , which may be delayed for several months.It is very vital to differentiate BPPV from central positional vertigo.
Central positional vertigo
Disequilibrium and nystagmus provoked by certain head movement, with less severe vertigo.
It is due to cerebellar hemorrhage or posterior fossa tumor
Dix-Hallpike test: nystagmus has no latent period and persists for minutes. This nystagmus is not fatigable when repeating the test.
Frequently, there are other associated CNS signs.
Vestibular neuronitis
It is also called epidemic vertigoSudden unilateral vestibular failure resulting in imbalance of the vestibular input to the brain.
Frequently preceded by a virus infection.
Aetiology
The condition is thought to be due to viral infection of the vestibular nerve.
Clinical picture
It is characterized by severe vertigo for several days without deafness or tinnitus and no signs of neurological involvement.Severe neuro-vegetative symptoms: nausea and vomiting, and the patient is confined to bed.
Diagnosis
The patient has horizontal nystagmus and caloric test reveals canal paresis on the affected side.Treatment
I.V. fluid if there is severe vomiting.
Prochlorperazine (stemetil) is antiemetic and sedative, cinnarzine (stugeron) is labyrinthine suppressant, and betahistine (betaserc) is H3 antagonist and vasodilator.
There is gradual recovery resulting from central compensation.
Young people recover quickly but an old person may be unsteady for months following an attack.Early mobilization
Cinnarzin for only few days in old people.
Meniere's Disease
paroxysmal attacks of vertigo, deafness and tinnitus.Prosper Meniere1861.
Pathology
Endolymphatic hydrops(dilatation of the endolymphatic compartment of both cochlea and vestibule).
Aetiology
Unknown, different theories have been postulated to explain the condition:hereditary factor
defective absorption of endolymph
local ischemia .
Clinical picture ( Vertigo, Deafness, Tinnitus)
Any ageFemale are affected more than male.
The disorder is usually unilateral, but the other labyrinth is eventually affected.
Recurrence of attacks is typical and may vary from a few weeks to several years.
Vertigo: sudden onset of severe vertigo lasting for few hours, and associated with vomiting, nystagmus, sweating and bradycardia.
The patient may fall and injure himself but he is fully conscious.
Some patients get warning before attack by fullness sensation in the ear (aura).
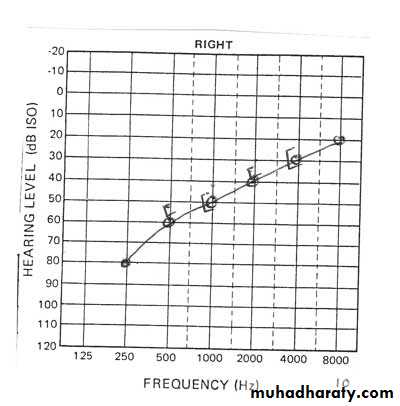
Deafness: SNHL starts during the attack and returns to normal after the attack. As the disease progresses, hearing deteriorates and finally severe deafness results in the affected ear.
Tinnitus in the affected ear, later on becomes permanent.
Aural fullness: Due to increase pressure in the endolymph.
Diagnosis
Between the attacks, clinical examination may be completely normal.During the attack, the patient is unsteady with nystagmus.
Otoscopy: normal.
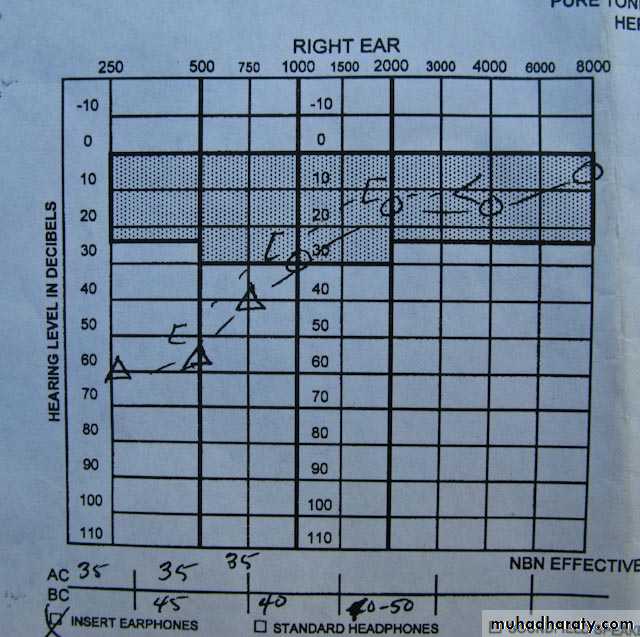
Audiogram: low frequency SNHL.
Caloric test: canal paresis in the affected ear.
Treatment
I. MedicalBed rest, anxiolytic: I.V. diazepam,
fluid and salt restriction with diuretics.
Prochlorperazine , cinnarzine and betahistine (betaserc), the latter is often prescribed for few months.
II. Surgical
Endolymphatic sac decompression and shunt.
Vestibular nerve section.


THANK YOU