INNER EAR
د. هيثم النوريFIBMS- ENT
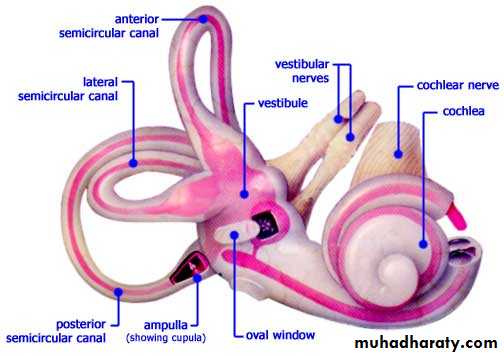
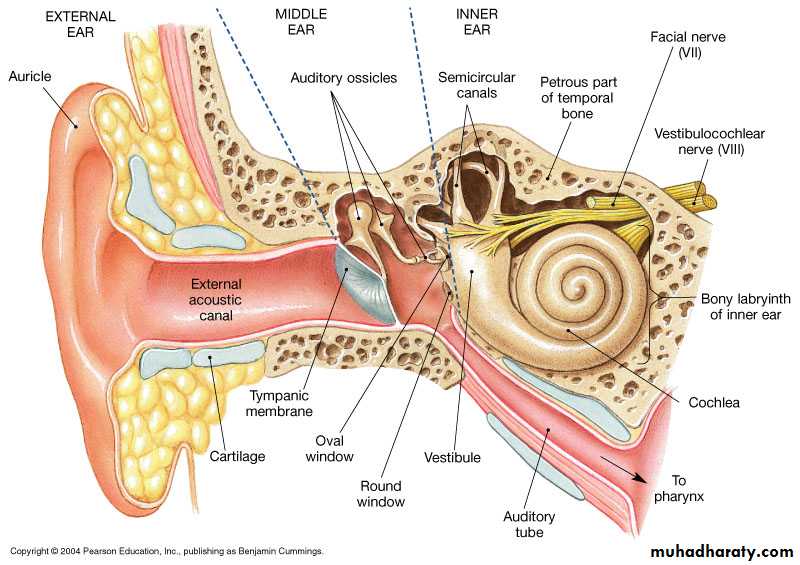
Inner Ear
OtosclerosisDeafness Sudden hearing loss
Ototoxic drugs
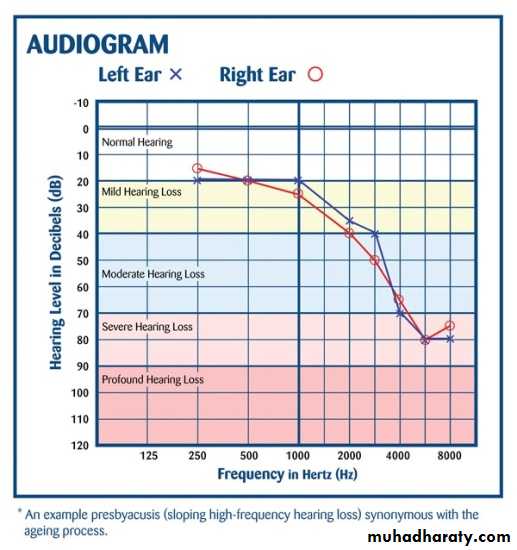
Presbyacusis
Acoustic trauma
Vertigo BPPV
Menier's disease
Vestibular neuronitis
Tinnitus Vestibular schwannoma( acoustic neuroma)
Deafness (Hearing Loss)
Subjective impairment of hearing
Conductive deafness
Sensorineural deafness
Mixed deafness
C H L
S N H LConductive Hearing Loss
Sound appears quieter
but it is not distorted.Sounds are well heard
when amplified.Paracusis Willisii positive
especially otosclerosis
The quality of speech is
well maintained.Tinnitus usually absent
Sensorineural Hearing LossSound distorted leading to loss
of speech discrimination.Sounds ' distortion limits
the benefit of amplification.Paracusis Willisii negative.
In severe cases speechbecomes indistinct and
expressionless because patient
does not hear his own voice.
Tinnitus present
• A. Congenital: meatal atresia.
• B. Acquired• Ext ear: impacted wax,F.B, SCC.
• Middle ear:
• a. Trauma: TM perforation
• & ossicular disconnection.
• b. Inflam: CSOM, OME
• d. Tumors: glomus jugulari.
• Otic capsule: otosclerosis
SNHL
Cochlear , retrocochlear
A. Congenital:
a. Intrauterine infection.
b. Toxins: kernicterus.
B. Acquired:
Traumatic; head injury and
blast injury.
Infective; Labyrinthitis, measles
, mumps ,syphilis, meningitis
Meniere’s disease.
Ototoxic drugs.
Degenerative: presbyacusis.
Neoplastic: acoustic neuroma
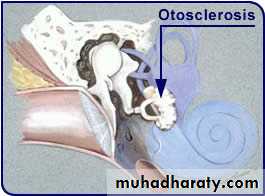
Otosclerosis (Otospongiosis)
Deafness
Tinnitus
Vertigo
Otosclerosis (Otospongiosis)
Hereditary osseous dyscrasia localized to otic capsule.resorption and re-formation of new bone.
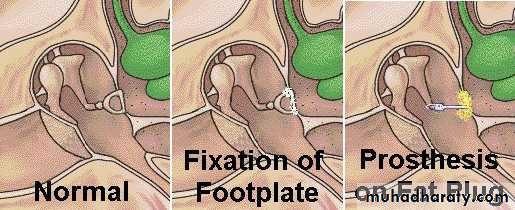
ankylosis of the foot plate of stapes leading to conductive deafness.
Aetiology
Hereditary factors: family history in 50%Autosomal dominant
Racial distribution: white races (Caucasian)
Age: 15-45 years of age.
Sex: the disease appears more frequently in females 2:1.
Pregnancy: may accelerate the condition.

Pathology
phase of otospongiosisNormal bone is absorbed and replaced by vascular spongy osteoid bone
sclerotic phase
spongy bone will is replaced later on with dense sclerotic bone
•
Pathology
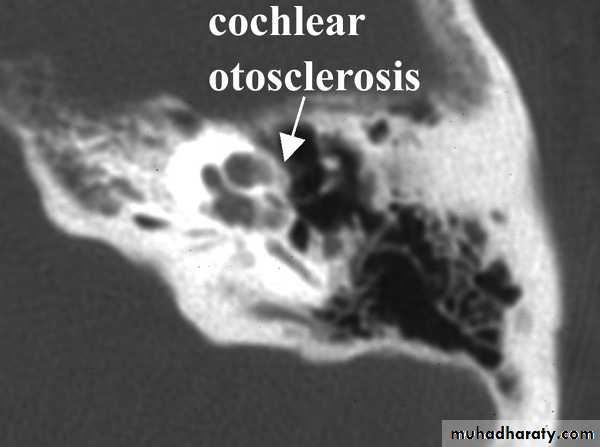
Bilateral (80%).Cochlear involvement may occur later on leading to sensorineural hearing loss.
Clinical Picture ( Deafness Tinnitus Vertigo)
Young adult femaleslowly progressive hearing loss, bilateral and conductive.
The patient speaks in a quiet voice, very different from the loud and harsh speech of those with sensorineural hearing loss.
Paracusis Willisii
Tinnitus: It tends to be worse in patients with cochlear involvement and during periods of rapid progression.
Vertigo: is a rare symptom more likely to be provoked by sudden changes of posture. Usually it is just dizziness rather than true vertigo.
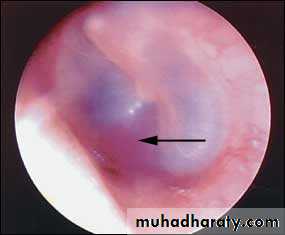
Examination
Otoscopy: tympanic membrane is normal.Schwartze’s sign.
Tuning fork tests: negative Rinne's test and the Weber test is lateralized to the more affected ear.


PTA: Conductive deafness with Carhart notch
Type As “ stiff ” tympanogram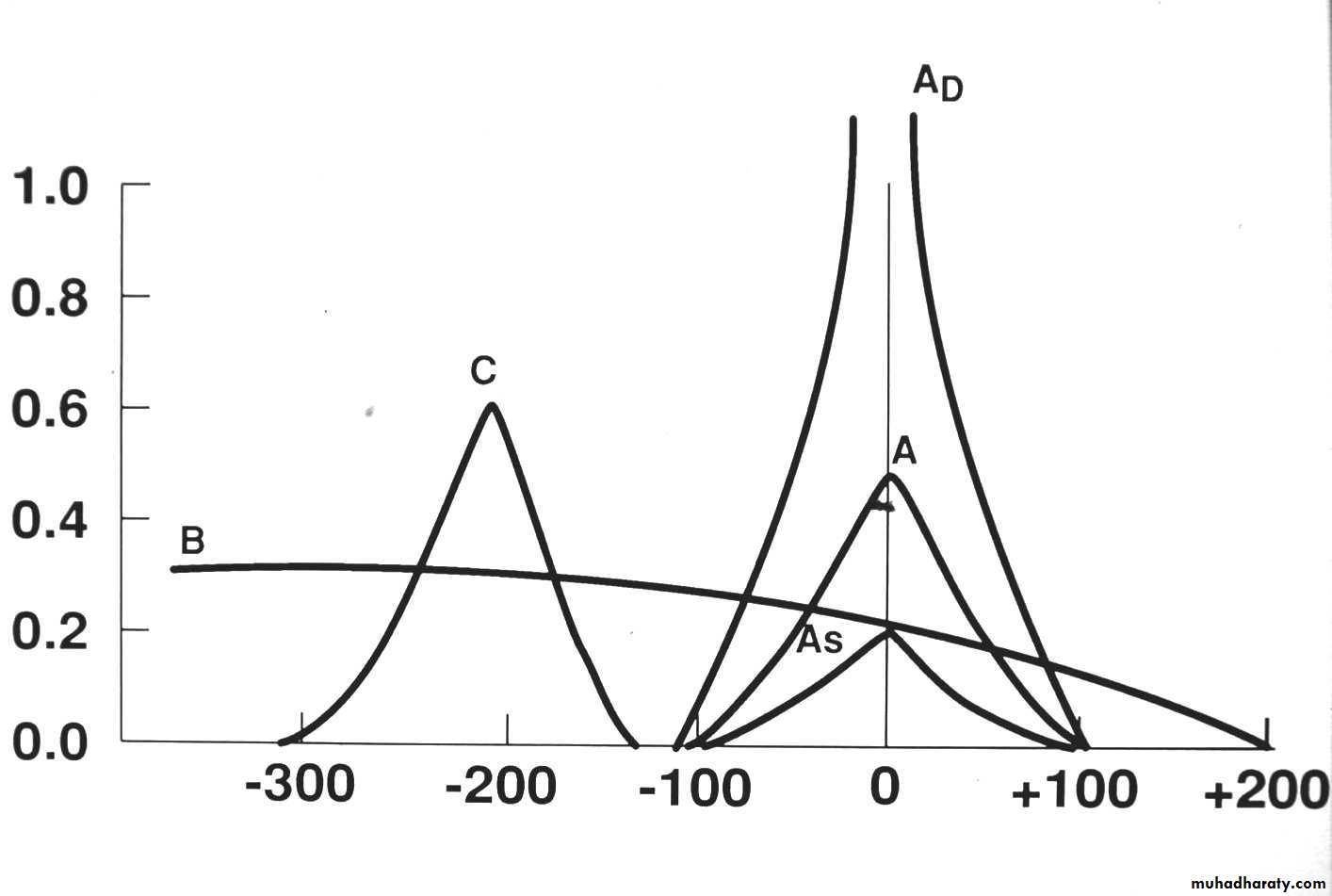
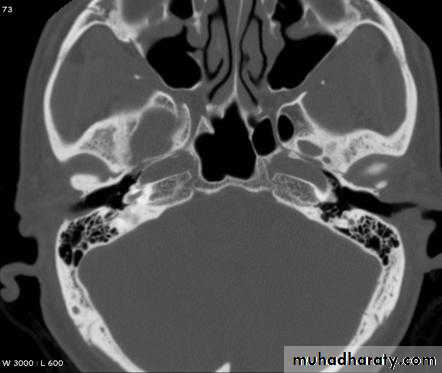
CT scan: to assess extent of otosclerosis.
Differential Diagnosis
Secretory otitis media (glue ear).Congenital ossicular fixation.
Paget disease..
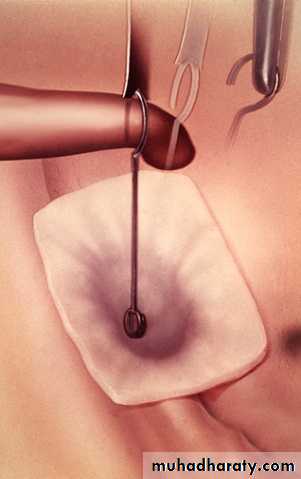
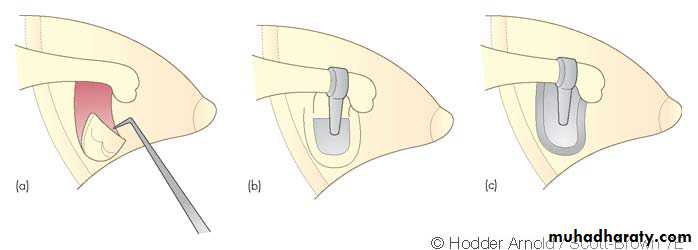
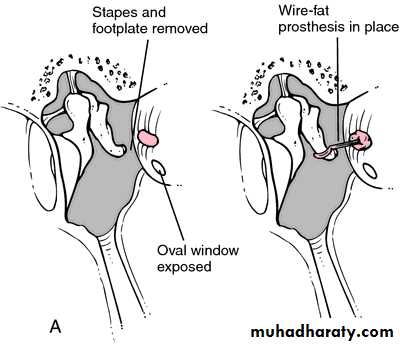
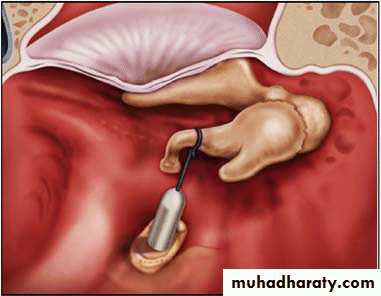
Treatment
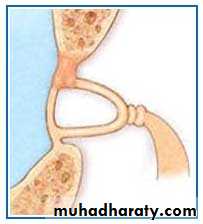
Surgical: stapedectomy which is total or
partial removal of the foot plate of the stapes and replacement by a prosthesis.

Medical: Sodium floride oral tab 20-60 mg for 6 months, together with hearing aids.
Floride is thought to slow-up progression of disease.
Hearing aids are used only when surgery is contraindicated or refuse.
Sudden Hearing Loss
Sudden conductive hearing loss may be due to :impacted wax
traumatic perforation
ossicular chain disruption
Sudden SNHL
Idiopathic: in 2/3 of cases no cause could be found.Vascular: spasm, thrombosis or haemorrhage of the internal auditory artery.
Viral infection: mumps, measles, rubella or Herpes zoster.
Trauma: Head injury, blast injury, ear surgery as stapedectomy.
Raised intracranial pressure as it occur in straining , coughing and bending down position , these may lead to rupture of round window .
Tumours: Acoustic neuroma (10%).
Clinical Picture of sudden SNHL
Hearing loss: occurs over minutes, hours or days.Tinnitus: good prognostic sign, means that hair cells still functioning.
Vertigo: common in those with vascular aetiology , carries bad prognosis.
Examination
TM is usually normal.
Tuning fork test: Rinne test is positive and Weber test is lateralized to the better hearing ear.
PTA: Hearing loss in high frequency, sometimes total hearing loss.
Treatment of sudden SNHL
Bed rest.Steroids 1-2 mg/kg prednisolon for 5 days.
Vasodilators: Betahistine 16 mg tid ± breathing 5% CO2 in air (carbogen) to improve the cochlear circulation.
Low molecular weight dextran: to lessen sludging of blood in the
small vessels of the cochlea.
Prognosis
1/3 : quick recovery.If there is no recovery within 3 weeks it is unlikely to occur.
1/3: partial recovery.
1/3: No recovery
A severe loss, high frequency loss, absence of tinnitus and the presence of vertigo are unfavourable prognostic features.
Drug Ototoxicity
Aminoglycosides: gentamycin, amikacin, neomycin.
Loop diuretics: frusemide and ethacrynic acid.
Salicylates: transient deafness and tinnitus.
Quinine.
Antiepileptics: phenytoin.
B-blockers.
Cytotoxics: cisplatin.

Clinical Picture
Tinnitus is often the first symptom followed by SNHL at high frequency. Vertigo is less common.Management
Keep the plasma level in a safe range and avoid or discontinue ototoxic drugs whenever there are signs of otoxicity.Presbyacusis (senile Hearing Loss)
Symmetrical Bilateral SNHL which occurs after the age of 65 years with no underlying cause.The degenerative changes occur as a result of aging process, vascular insufficiency or noise exposure.
Clinical Picture
Deafness is characteristically progressive, bilateral SNHL with marked loss of speech discrimination due to inability to hear the higher frequencies(consonant sounds).Thus, speech is difficult to be understood especially if fast, too loud or in a noisy background.
PTA: Bilateral symmetrical SNHL.
Treatment
Lip reading and auditory training.It is important to speak slowly, distinctly and not to shout with these patients.
Hearing aids: If the hearing loss is greater than 40dB.

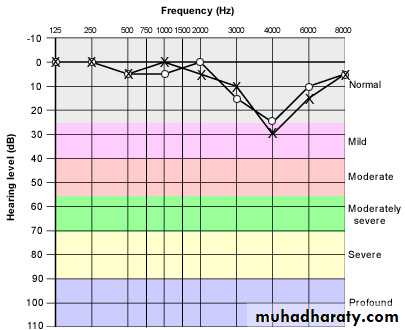
Deafness and Noise
Deafness that results from excessive sound stimulation.Acoustic trauma: SNHL due to brief exposure to very loud noise e.g. gunfire and explosions.
Noise-induced hearing loss: prolonged exposure to loud noise in certain occupations. A noise level in excess of 85 dB for 8 hours/ day is hazardous.
Tinnitus is usually a feature.
PTA: The earliest changes of acoustic trauma is SNHL at 4kHz which may be transient( temporary threshold shift).
If the condition is repeated, SNHL will affect all frequencies.
Treatment
preventive: by using protective ear plugs and screening personnel in noisy occupations by routine audiometry.Therapeutic:
Avoidance of further trauma.
Hearing aids and auditory training.