بسم الله الرحمن الرحيم
1
Rickets
Objectives
1.To know the definition of rickets
2.To know the clinical manifestations of rickets
3.To know the diagnosis &treatment of rickets
Rickets
Is defined as failure of mineralization of growing bone or osteoid tissue due to vitamin D deficiency .Vitamin D deficiency appear as rickets in children before epiphysial center (growth plates ) closure and as oteomalacia in post pubertal adolescents and adults.
2
Vitamin D synthesis
In the skin the substance 7-dehydro cholesterol in sun exposure changed by the effect of ultra violet ß radiation to Vitamin D3 (3-cholecalciferol ) this substance bind to Vitamin D binding protein , transferred to the liver and by 25 hydroxylase enzyme changed to form ( 25 hydroxy vitamin D ) and this substance transferred to the kidney and in the presence of 1α hydroxylase enzyme changed to (1-25 dihydroxy vitamin D) (calcitriol ) which is the active form and act by increasing the absorption of calcium and phosphorus from the intestine .3
Vitamin D function
Both vitamin D2(plant &yeast source) &D3are hydroxylated in the liver to 25-hydroxy vitamin D (calcidiol ) which is further hydroxylated in the kidney to 1-25dihydroxy vitamin D (calcitriol ) which act as hormone &the most biologically active form of the vitamin it :1.It stimulate calcium absorption in the small intestine .
2.Increase bone formation &growth plate mineralization by providing sufficient circulating calcium also mediating resorption .
3.May have a direct anabolic effect on the bone .
4.Has direct feed back to the Para thyroid gland & inhibit secretion of parathyroid hormone .
Mineralization can not occur unless adequate calcium & phosphorus are present .
4
Vitamin D sources :
1.Cutaneous synthesis .2.Dietary sources :
.Breast milk has low vitamin D content approximately(12-60 )IU\L .
Fortified food especially fortified formula which contain (400 IU\L)
Fish liver oil have a high vitamin D content ,other good sources is fatty fish & egg yolk & diary products .
Supplemental vitamin D like ergocalciferol which comes from plants or yeast & cholecalciferol (mammalian form ) both can be produced synthetically & available as dietary supplements .
5
Causes of vitamin D deficiency :
1.Inadequate direct sun exposure .2.Decreased vitamin D intake .
3.Breast fed infants .
4.Dark pigmented skin .
5.Secondary vitamin D deficiency
a. Malabsorption (cholestatic liver disease ,defect in bile acid metabolism ,cystic fibrosis ,coeliac disease ,crohns disease ).
b.Increase degradation by medications as Phenobarbitone & Phenytoin
c.Decrease phosphate absorption by Aluminum containing antacids
d.Chronic renal failure
6
Clinical manifestations :
Are most common during the first 2 years of life & may become evident only after several months of vitamin D deficient diet ,vitamin D deficient rickets is rare later in child hood .The head :
1.Craniotabes is one of the early signs of rickets due to thinning of the outer table of the skull it is felt as aping-pong ball sensation when pressing firmly over the occiput or posterior parietal region .
Non rachitic craniotabes seen in normal infants in the immediate post natal period & disappear by the second to fourth month but also can be seen in hydrocephalus &osteogenesis imperfecta .
7
Clinical manifestations
2.Frontal bossing3.The anterior fontanel is enlarged & its closure may be delayed until after the second year of life .
4.Caput quadratum means box like appearance of the head .
The teeth:
Eruption of the temporary teeth may be delayed & there may be defect of the enamel & extensive caries .
Permanent teeth that are calcifying during period of vitamin D deficiency may also be affected .
Extremities :
1.Thickening of the wrist & ankle felt as widening of the wrist is an early sign of rickets .
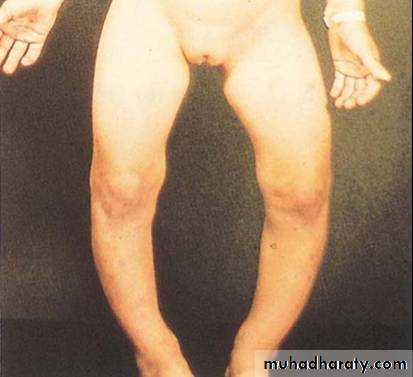
2.Bowing of the legs .
3.Wind swept deformity (combination of valgus deformity of leg &varus deformity of other leg ) .
4.Anterior of tibia & femur
5.Coxa vara
8
Clinical manifestations
The chest :Rachitic rosary :is palpable enlargement of the costochondral junction .
Pigeon chest deformity due to projected sternum forward .
Harrison groove or sulcus seen on the lower border of the chest due to pulling of the softened ribs by the diaphragm during inspiration .
Recurrent respiratory infections due to softening of the ribs which impair air movement &predispose patients to atelctasis .
Pelvis:
Deformity of the pelvis in girls lead to obstructive labor
9
Clinical manifestations
Muscles' : are poorly developed & lack tone as a result children with moderately severe rickets don’t stand & walk at usual ages .(Delayed walking )Relaxation of ligaments leading to deformities like knock knees ,(kyphosis & scoliosis ) of the back.
In advanced rickets :
1.scoliosis & lordosis may be present .
2.Bow legs (genu varus ) & knock knees (genu valgus ) .
3.Green stick fractures in long bones .
10
Bowed legs and swollen wrists in rickets
11
Harrison groove

12
Widening of the wrist

13
Rachitic rosary

14
Diagnosis :
1.Clinical2.X-ray of the wrist :will show characteristic radiographic changes of the distal ulna &radius include :
.widening
.concave cupping &fraying (poorly demarcated ends ).
.There is increased distance between the distal ends of radius &ulna &the metacarpal bones .
3.Lab investigations :
.Serum Calcium usually is normal but may be low .
.Serum phosphorus level usually is reduced due to PTH induced renal loss of phosphate combined with decrease in intestinal absorption .
.Serum alkaline phosphatase activity is elevated .
15
Rickets &hypocalcaemia
Normal serum Ca.level is ( 8.5-10.5 )mg\dl when it become 7.5 mg tetany will occur .Symptomatic hypocalcaemia is treated by I.V Calcium infusion followed by oral Calcium supplement for 2-6 weeks of about 1000 mg \day .
Hypocalcaemia either causing :
Tetany
Stridor secondary to laryngeal spasm
Convulsion
16
Radiological changes of rickets

17
Prevention :
1.Direct sun exposure .2.Vitamin D supplementation of all breast infants in the amount of (200-400 )IU\day started in the first 2 months of life .
18
Treatment :
1.Single dose of (300.000-600.000) IU of vitamin D orally or IM the effect will be seen after 2-4 weeks radiologically healing is rapid allowing earlier differential diagnosis from genetic vitamin D resistant rickets .2.The alternative is oral administration of daily high dose vitamin D in a dose (2000-5000 )IU\day of vitamin D3 over 4-6weeks followed by daily vitamin D intake of 400 IU\day .
Healing rickets :
Calcification takes place in the zone of preparatory calcification ZPC which will be seen radiologically .
19
Congenital vitamin D deficiency
1.Severe maternal vitamin D deficiency during pregnancy2.Lack of adequate sun exposure
3.Closely spaced pregnancies
Newborn presented with symptomatic hypocalcaemia ,IUGR , decrease bone ossification with classic rachitic changes with defect in dental enamel .
Prevention by maternal supplementation of multi vitamins including vitamin D during pregnancy .
20
Other types of rickets
Vitamin D dependant rickets type 1 :
It is autosomal recessive disorder ,due to defect in gene encoding 1α hydroxylase enzyme in the kidney so conversion of 25-vitamin D to 1-25 vitamin D will not occur .
Diagnosis :low level of 1-25 vitamin D
Treatment by 1-25 vitamin D (calcitriol 0.25-2 )μg\day
21
Vitamin D dependant rickets type -2
There is mutation in gene encoding the vitamin D receptor preventing the normal physiologic response to 1-25 vitamin D .Diagnosis : elevated 1-25 vitamin D
Treatment : 3-6 mg /day of vitamin D with oral calcium (1000-3000 ) mg\day
22
X-linked dominant hypo phosphatemic rickets XLH
Among the genetic disorders causing rickets due to hypophosphatemia, X-linked hypophosphatemic rickets (XLH) is the most common, with a prevalence of 1/20,000. The defective gene is on the X chromosome, but female carriers are affected, so it is an X-linked dominant disorder.There is increase phosphate excretion in renal
tubules & decrease synthesis of 1-25 vitamin D calcitriol .
Treatment ; combination of oral phosphorus 1-3 gm /day divided to 4-5 doses with 1-25 vitamin D calcitriol
23
Autosomal dominant hypo phosphatemic rickets
There is decrease reabsorption of phosphorus in the renal tubules & decrease hydroxylation of 25-vitamin D to1-25 vitamin D ,due to inhibition of 1 α hydroxylase in the kidney
Treatment is similar to the approach used in XLH
24