Vascular Diseases:
Vascular abnormalities cause clinical disease by two principal mechanisms:• Narrowing or complete obstruction of the lumen by atherosclerosis or thrombo-embolism respectively.
• Weakening of the wall leading to dilation or rupture.
Normal:
The basic constituents of the wall are:1. Endothelial cells.
2. Smooth muscle cells.
3. Extracellular matrix (ECM), including elastin, collagen and glycosaminoglycans.
The 3 concentric layers-intima, media and adventitia-are most clearly defined in the larger vessels particularly arteries. Arteries consist of:
1. Intima.
2. Internal elastic lamina.
3. Media.
4. External elastic lamina.
5. Adventitia.

Congenital Anomalies:
Mostly are important in surgery during which an unexpected vessel can be injured. The anomalies are rarely symtomatics except in the coronary tree. Among the anomalies which are pathologically important are:• Arteriovenous fistula (AVF) is rare small abnormal communications between arteries and veins.
• Causes
Developmental defects
• Or produced from rupture of an arterial aneurysm into adjacent vein,
• Trauma (penetrating injuries)
• Inflammatory necrosis of adjacent vessels.
They may be of clinical significance because
• they short circuit blood from the arterial to the venous side causing cardiac volume overload which lead to high output cardiac failure.
• They can rupture causing hemorrhage especially in the brain.
2- Berry Aneurysms, are saccular congenital of unknown etiology seen in smaller arteries of the brain especially in the circle of Willis:
• Although the majority occur sporadically, genetic factors may be important.
• Cigarette smoking and hypertension are considered as predisposing factors.
• Although the aneurysms" are labeled as congenital, they are not present at birth but develop over time owing to the underlying defect in the media.
• Morphologically, they measure few millimeters up to 3cm. There is lack of intimal elastic tissue and muscle fibers in the wall, which are replaced by hyalinized tissue.
• Rupture of the aneurysm leads to subarachnoid hemorrhage, most frequent at the fifth decade and slightly more common in female. The rupture is associated with acute increase in intracranial pressure.
• In 20% of cases, multiple Berry aneurysms occur this type associated with adult polycystic kidney diseases.









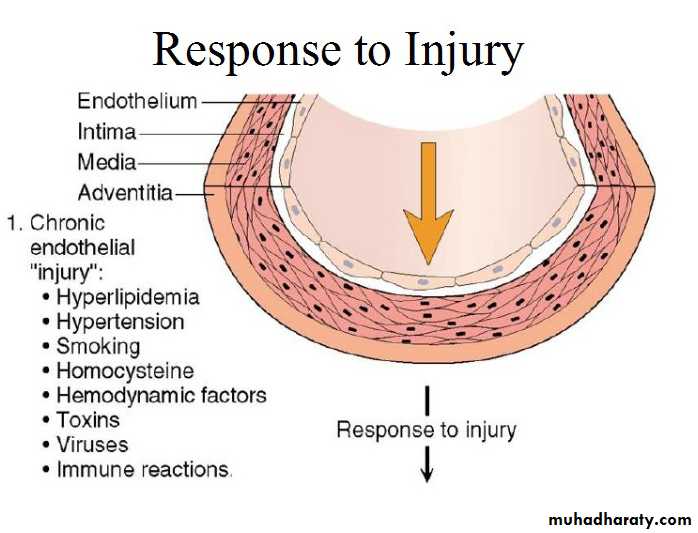







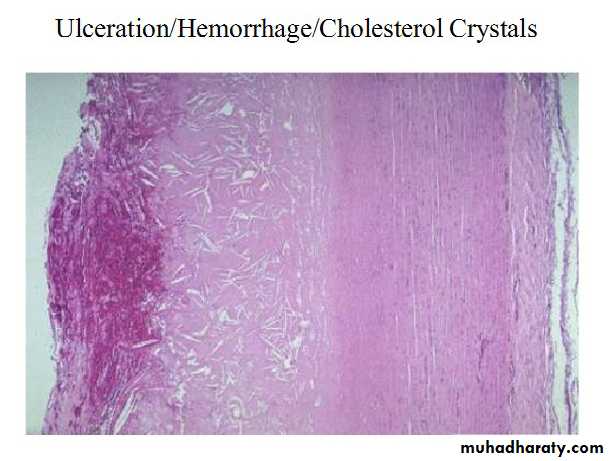
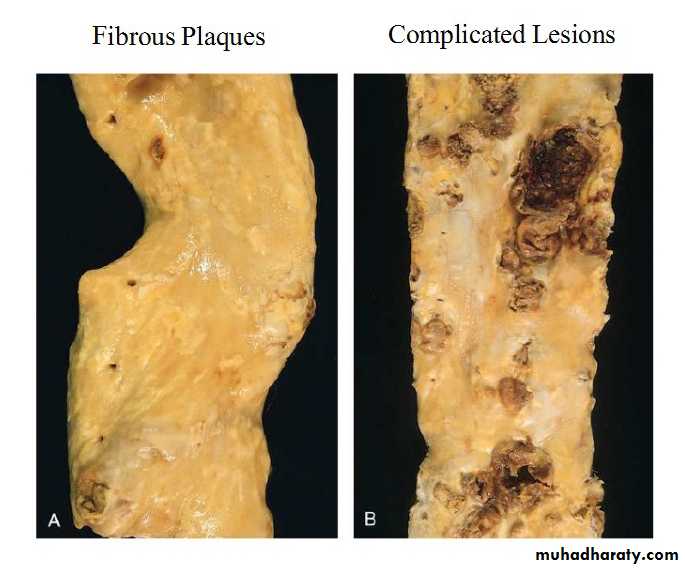
Atheromatous plaque
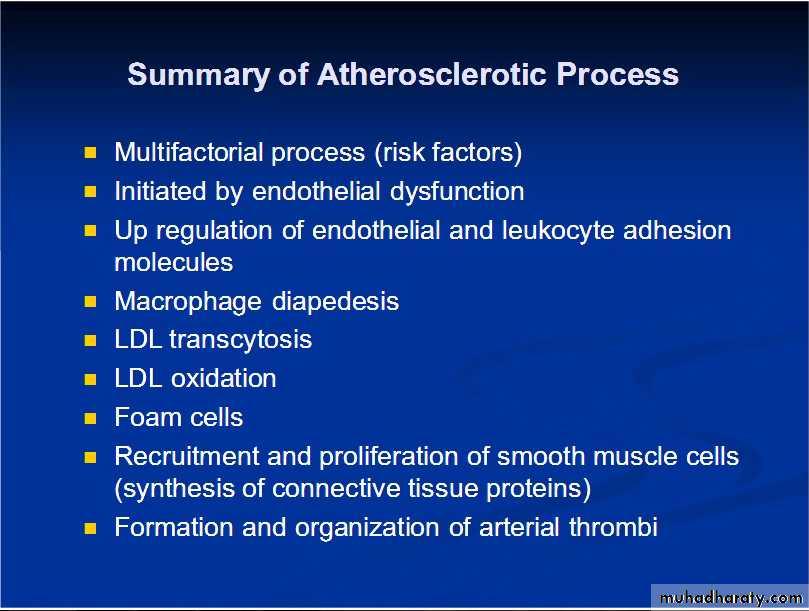




Consequences of Atheroscerosis

• Consequences of coronary artery atherosclerosis (Ischemic Heart Diseases (IHD))


Hypertensive Vascular Disease:
It is a multifactorial disorder defined as sustained elevation of blood pressure above 140/90 mmHg. According to this criterion about 25% of populations are regarded as hypertensives. There are two types:
• Essential (idiopathic) in 95% of cases.
• Secondary due to some underlying cause :
• Renal (glomerulonephritis, renal artery stenosis and polycystic kidney diseases.
• Endocrine (adrenocortical, pheochromocytoma, hyper and hypothyroidism).
• Cardiovascular (coarctation of aorta and polyarteritisnodosa).
• Neurogenic (psychogenic, increase intracranial pressure).
Clinical features
Atherosclerosis can begin in childhood but is typically asymptomatic for decades until it finally manifests as the following :• Insidious narrowing of vascular lumens (e.g. gangrene of the lower leg because of stenosing atherosclerosis in the popliteal artery).
• Plaque rupture of superficial erosion followed by superimposed thrombus causing sudden luminal occlusion (e.g. MI).
• Vessel wall weakening followed by aneurysm formation.
• Providing a source of thromboembolic
Pathogenesis, basically there is alteration in the relationship between cardiac output and peripheral vascular resistance. The major factors that determine blood pressure variation are:
• 1. Age.
• 2. Gender.
• 3. Body mass index.
• 4. Diet principally sodium intake.
Kidneys play an important role in blood pressure regulation through:
• 1. Renin-angiotensin system.
• 2. Vasodilators (prostaglandins, nitric oxide).
• 3. Glomerular filtration.
• 4. Natriuretic factors.
•
Essential hypertension results from an interaction between genetic and environmental factors include; stress, obesity, cigarette smoking, physical inactivity and heavy consumption of salt.
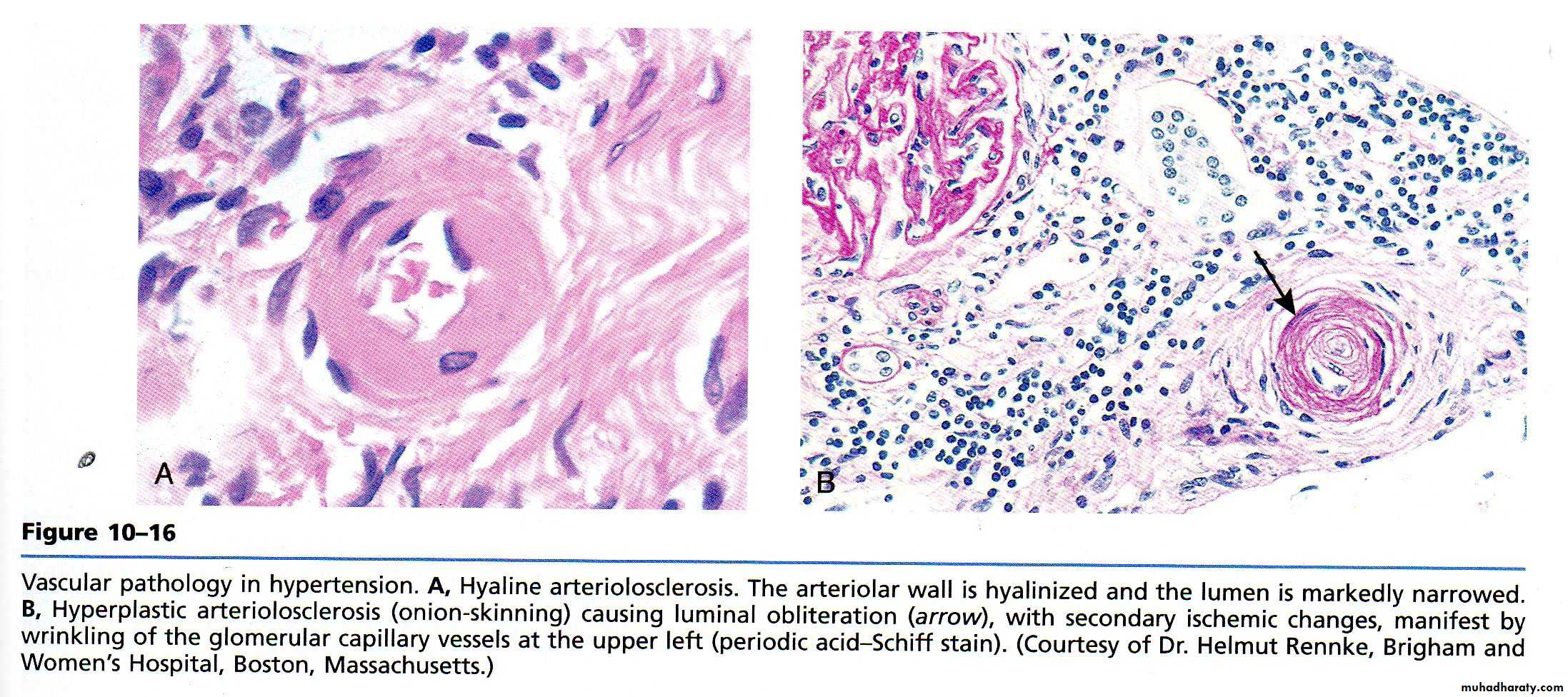
Morphology, there are two changes:
l. Hyaline arteriosclerosis.
• Occur in elderly patients particularly those with mild hypertension and diabetes.
• The lesion probably reflect EC injury with plasma leakage into arteriolar walls and ECM synthesis from SMCs.
• Microscopically there is diffuse pink hyaline thickening.
2. Hyperplastic arteriolosclerosis :
• Characteristic of malignant hypertension.• There is concentric laminated (onion skin) thickening
Aneurysms:
It is a localized dilatation of the vessel or heart wall. We have two types:• True,
• False.
Causes, include:
• Atherosclerosis.• Congenital.
• Trauma.
• Infection (syphilis).
• Inflammation.
Morphologically: there are 2 types
1.Saccular.
2.Fusiform.
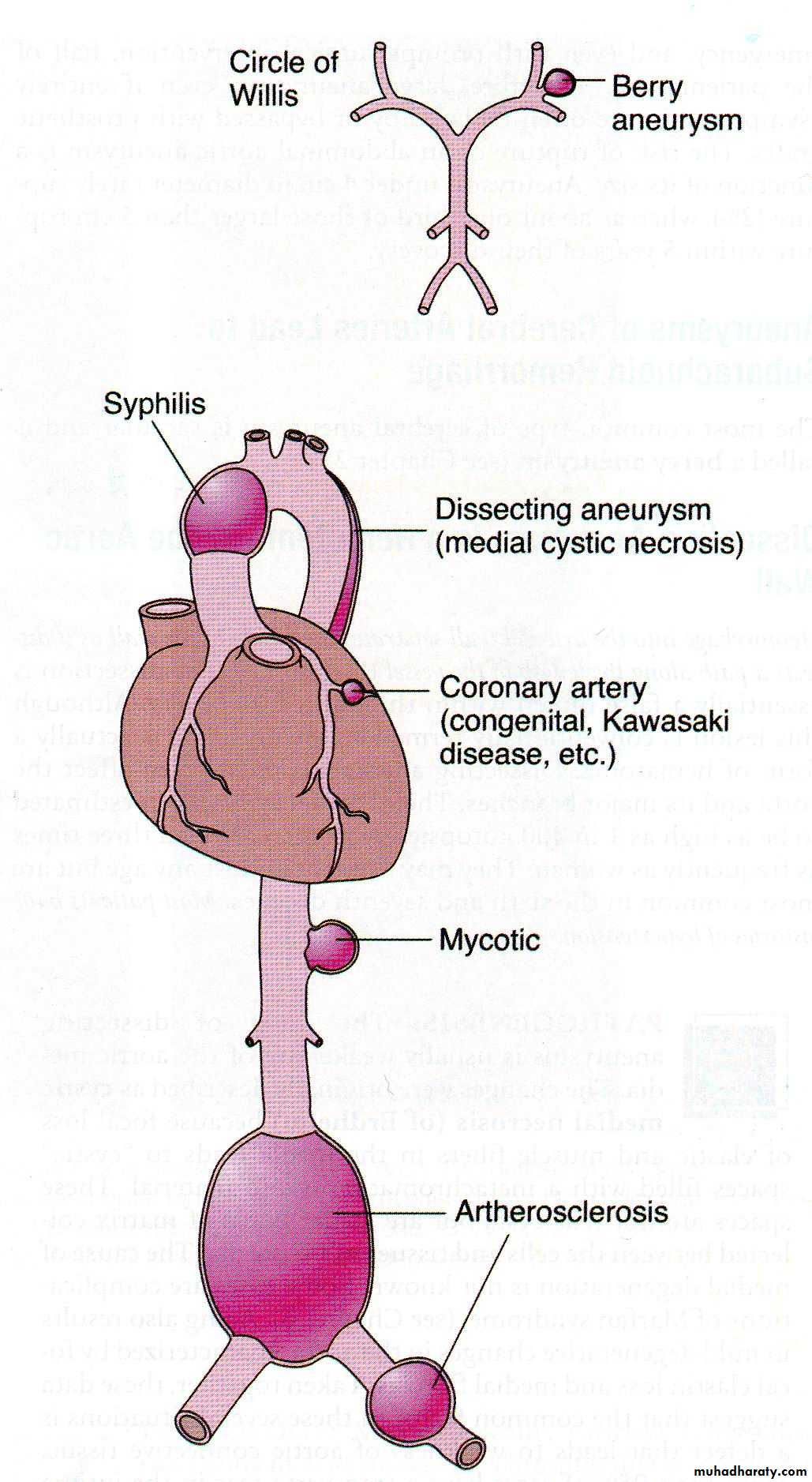
Types and sites of Aneurysm
Abdominal aortic aneurysm (AAA):Is a localized abnormal dilation of a blood vessel, it is due to atherosclerosis, which may involve also the" common iliac arteries, aortic arch and descending part of thoracic aorta.
Morphology, positioned between renal arteries origin and bifurcation of aorta. It is either saccular or fusiform up to 15cm in diameter and 25cm in length.
There is an inflammatory AAA of unknown cause.
Mycotic AAA is a complicated atherosclerotic due to infection by bacteria such as salmonella.
Pathogenesis, there are 2 theories:
• Genetic defects in connective tissue component leading to dissection then to aneurysm.• Recently attention was focused on altered balance of collagen degradation and synthesis mediated by local inflammatory cells. So altered collagen could provide a susceptible substrate on which atherosclerosis or hypertension or both could act to weaken the wall.
Matrix-metalloproteinases produced by inflammatory cells cause proteolysis of the extracellular matrix proteins. A decreased level of tissue inhibitors of metalloproteinases has been reported in aortic aneurysm.
Clinical course, the condition is rare before the age of 50 years and it is more common in males. Symptoms appear in case there are:
• Rupture, potentially fatal hemorrhage related to size.
• Obstruction of iliac, renal, mesenteric or vertebral vessels.
• Embolism.
• Pressure on adjacent structures (ureter, vertebra).
• Abdominal mass.
Treatment is by using stent grafts (expandable wire frame).
Syphilitic aneurysm:
Syphilitic obliterative endarteritis of the vasa vasorum of the thoracic aorta leads to aneurysm which may involve aortic annulus.
Pathogenesis, obliterative endarteritis of adventitial vasa vasorum causes patchy loss of medial elastic fibers and muscle cells followed by inflammation and scarring that leads to weakening of the wall and aneurysmal dilation. Involvement of the aortic annulus leads to aortic valve incompetence and left ventricular hypertrophy.
Clinical course, there are several outcomes:
• Pressure on mediastinal structures (lung, airways, esophagus, recurrent laryngeal nerve, vertebrae and ribs).• Heart failure.
• Rupture.
Aortic dissection:
Catastrophic illness characterized by dissection of blood between and along the laminar planes of the media, with the formation of a blood filled channel within the aortic wall which often ruptures outward causing massive hemorrhage. Affecting 2 groups of patients:• More than 90% occur in men of 40-60 years of age who are hypertensive.
• In younger age group with systemic or localized abnormality of connective tissue.
• The condition may be iatrogenic as a complication of arterial cannulation (diagnostic catheterization or cardiopulmonary bypass).
• Rarely may occur during pregnancy.
Morphology, there is intimal tear usually within 10cm of aortic valve, which is either transverse or oblique, l-5cm in length. Dissection extends proximally and distally. The hematoma is located between the middle and outer thirds of the wall. It often ruptures outward but sometimes into the lumen with second distal tear. The most preexisting histologically detectable lesion in the aortic wall is cystic medial degeneration.
Pathogenesis, the trigger for intimal tear and intramural aortic hemorrhage is unknown in most cases. Once the tear has occurred,
increased systemic blood pressure maintains progression of the medial hematoma
Clinical course, there are 2 types:
• Type A (proximal), more common involving either the ascending portion only or both the ascending and the descending aorta.
• Type B (distal), starts distal to the subclavian artery origin. Sudden excruciating chest pain radiating to the back and moving downward is the common presenting feature. Most common cause of death is rupture to pericardial, pleural or peritoneal cavity. Currently 65-75% of patients will survive.
WHAT IS VASCULITIS?
Vasculitis is a clinicopathologic process characterized by inflammation and damage to blood vessels (Fibrinoid necrosis), leading to compromise of the vascular lumen resulting in ischemia of the tissues supplied by the involved vessels.Vasculitis
The 2 most common mechanisms are:1. Microbiological infection.
2. Immune-mediated.
Less common mechanisms are:
1. Physical injury (radiation).
2. Chemical toxins.
Pathogenesis of immune-mediated vasculitides, include:
1. Immune complex deposition.
2. ANCA mediated (pauci immune).
• Antiendothelial antibody.
Classification, depends on:
1. Size and anatomic site of the involved vessel.
2. Histology.
3. Clinical manifestation.
CLASSIFICATION
CLASSIFICATION
PRIMARY VASCULITIS SYNDROMESPREDOMINANTLY LARGE VESSEL VASCULITIS
GIANT CELL VASCULITISTAKAYASUS ARTERITIS
PREDOMINANTLY MEDIUM VESSEL VASCULITIS
PANKAWASAKIS DISEASE
PREDOMINANTLY SMALL VESSEL VASCULITIS
ANCA +VE---
c-ANCA +VE-
WEGENERS GRANULOMATOSIS
p-ANCA +VE
MICROSCOPIC POLYANGITIS
CHURG – STRAUSS SYNDROME
ANCA -VE
ESSENTIAL MIXED CRYOGLOBULINEMIA
HENOCH SCHONLEIN PURPURA
IDIOPATHIC CUTANEOUS VASCULITIS
BECHETS SYNDROME
PATHOGENIC MECHANISMS OF VESSEL DAMAGE IN VASCULITIS SYNDROMES
PATHOGENIC IMMUNE COMPLEX FORMATION AND/OR DEPOSITIONHSP
HEPATITIS ASSOSIATED PAN
PRODUCTION OF ANTINEUTROPHILIC CYTOPLASMIC ANTIBODIES
WEGENERS GRANULOMATOSIS
CHURG STRAUSS SYNDROME
MICROSCOPIC POLYANGITIS
PATHOGENIC T LYMPHOCYTIC RESPONSES AND GRANULOMA FORMATION
GIANT CELL ARTERITIS
TAKAYASUS ARTERITSWEGENERS GRANULOMATOSIS
CHURG STRAUSS SYNDROME
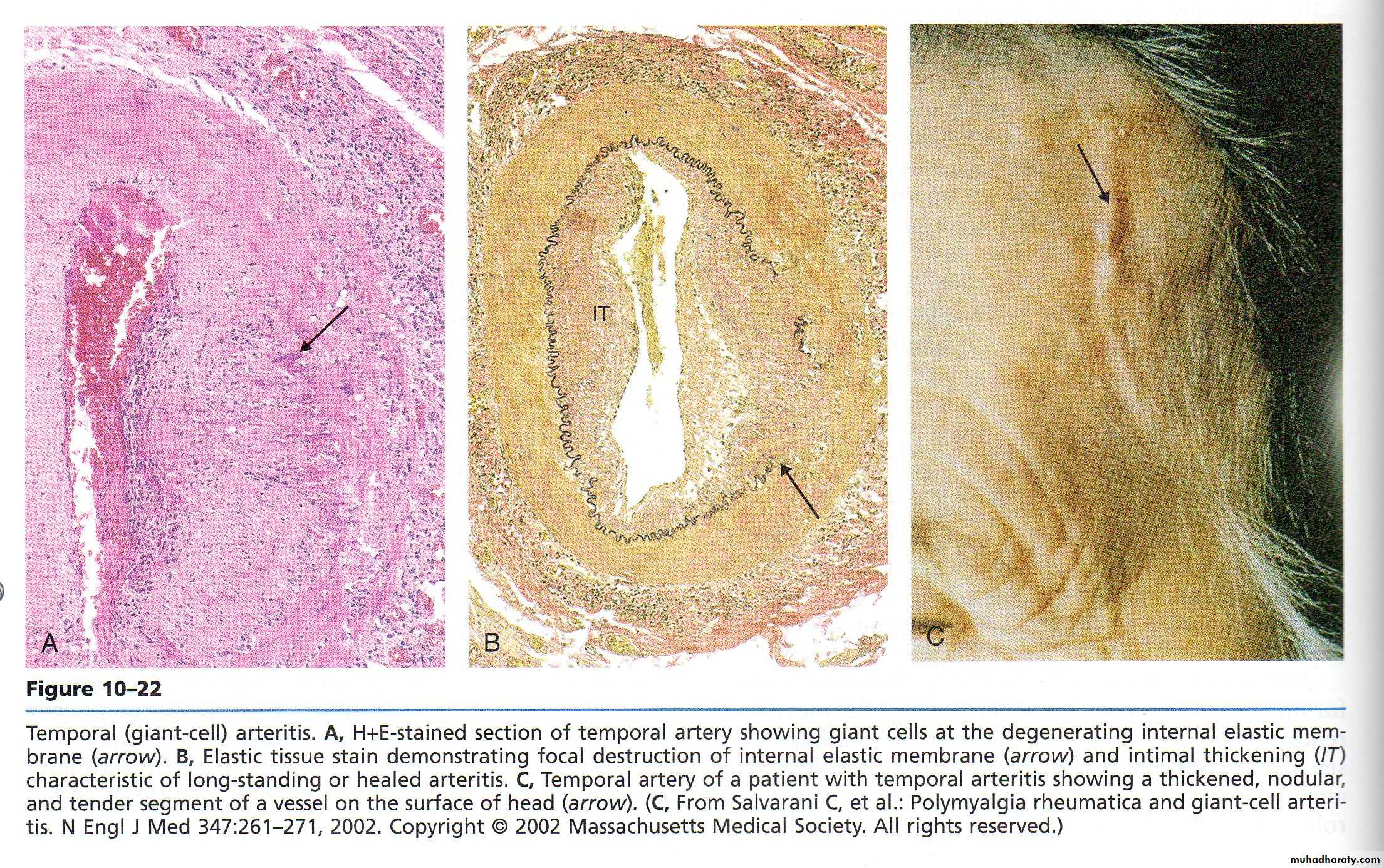
Giant cell arteritis
“Temporal arteritis”
Granulomatous large-vessel vasculitis
Older than 50 years
Headache ( ‘‘sinus’’ headache )
Fever, jaw or tongue claudication, and scalp tenderness
Polymyalgia rheumatica ( 40-50%)
Blindness from optic nerve ischemia (15- 20%) ,diplopia and ptosis
Life-threatening aortic rupture or dissection
Giant cell arteritis
Nodularity, tenderness or absent pulsations of the temporal arteries and other involved vesselsESR usually increased.
Temporal artery biopsy (TAB) : granulomatous inflammation of the media and adventitia, with histiocytes and mononuclear cells, giant cells, irregular fragmentation of the internal elastic lamina. positive 60-80%
Contralateral TAB if first biopsy negative
Prednisone at 40 to 60 mg/d
Takayasu arteritis
Granulomatous large-vessel vasculitis
Affects aorta, its main branches, and pulmonary a.
Predominantly in young women
Headaches and dizziness
Vascular hypoperfusion :limb claudication, double vision
Glucocorticoids
Wegener granulomatosis
Granulomatous, necrotizing, small and medium vesselInvolves upper,lower airways, and kidneys
Any age (40-55 yrs.) Men and women equally
Upper airways symptoms (recurrent or nonresolving sinusitis, nosebleeds, nasal crusting
Sinus pain, epistaxis, persistent otitis media, saddle nose deformity subglottic stenosis.
Single or multiple cavitating/noncavitating nodules or diffuse alveolar hemorrhage
Wegener granulomatosis
Microscopic hematuria, proteinuria, and rapidly progressive RFSkin rash, migratory arthritis
Ocular involvement (scleritis, corneal ulceration)
Mononeuritis multiplex or CNS involvement
Risk of venous thrombosis (DVT,PE) mechanism unclear
ANCA ( 96%)
Lung biopsy yield 91% of cases
Renal biopsy:focal, segmental necrotizing, crescentic glomerulonephritis with few to no immune complexes
Microscopic polyangiitis
Nongranulomatous necrotizing small-vessel vasculitis,few or no immune deposits
More common in male , average age of onset is 50 years
Persistent cough with or without hemoptysis
Kidneys (79%), joints (65- 72%), skin (44- 58%),
Pulmonary pathology shows capillaritis
Renal histology is similar to WG
Severe disease (lung, kidney, or nerve)
Churg-Strauss syndrome
asthma, fever, hypereosinophilia, systemic vasculitisall ages but rare in children and adolescents and occurs equally between sexes
recurrent allergic rhinitis, difficult-to-treat asthma, nonresolving ‘‘pneumonia’’/pulmonary infiltrates, or persistent eosinophilia
Peripheral eosinophilia (absolute eosinophil usually>1500)
Increased ESR,CRP, and IgE level
ANCA positive 50% of cases (predominantly MPO-pANCA)
Histology: eosinophilic tissue infiltrates, extravascular ‘‘allergic’’ granulomas, and small-vessel necrotizing vasculitis
Polyarteritis nodosa
medium-vessel diseaseIncidence 2- 9 per million annually
Men = women
constitutional symptoms, HT,musculoskeletal symptoms, symptoms from vasculitic involvement of nerves, GI tract , skin, heart, and nonglomerular renal vessels
suspected immunologic disease
Biopsy specimens : necrotizing inflammation involving medium-sized or small arteries,with abundant neutrophils, fibrinoid changes, disruption of the internal elastic lamina
Angiographic changes : microaneurysms ,stenoses, occlusion
Polyarteritis nodosa
severe life-threatening disease ( GI tract, heart, or CNS system): 2 mkd oral CYC and glucocorticoids
non–life or non–organ-threatening : glucocorticoids alone
Plasma exchange in severe cases
5-year survival rate with treatment 80%
Relapses are infrequent (8- 19%)
PAN-like vasculitis ass. with viral inf. eg. HBV, HCV, HIV
Rx with glucocorticoids , antiviral treatment , and plasma exchange induced remission 81% , relapse 10%
If clinical improvement , immunosuppression should be withdrawn while continuing antiviral treatment
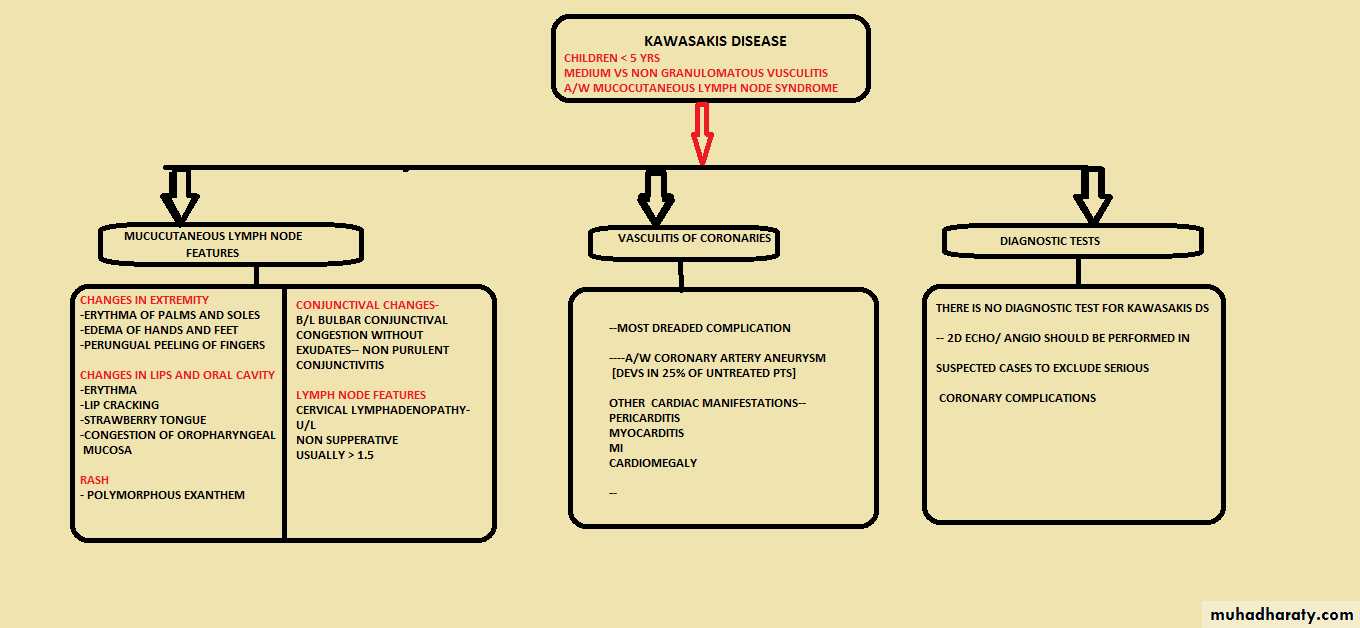
KAWASAKIS DISEASE
Henoch-SchÖnlein purpurasmall-vessel vasculitis
predominantly affects children
suspected drug allergy or immunologic condition
Purpura (100%), arthritis (82%), abdominal pain (63%), GI bleeding (33%), and nephritis (40%)
Complication : intussusception
Recurrence occurs in up to 40% ( mostly first 3 months)
tissue Bx : leukocytoclastic vasculitis with IgA deposition in blood vessel walls
Typically self-limited
Thrombo Angiitis Obliterans (Buerger Disease):
Segmental thrombosing acute and chronic inflammation of medium-sized and small arteries principally tibial and radial arteries with secondarily involvement of the adjacent veins and nerves. Starts in patients younger than 35 years in most of the cases.
There is strong relationship to cigarette smoking, due to rather
Direct toxicity, or
Hypersensitivity to some tobacco products.
Morphology, sharply segmental transmural acute and chronic arteritis accompanied by thrombosis.

Primary Raynaud Phenomenon:
Paroxysmal pallor or cyanosis of the digits of the hands or feet and infrequently the tips of the nose or ears owing to cold-induced vasoconstriction of the digital arteries, precapillary arterioles and cutaneouse artero-venous shunts. Median age is 14 years. The course is benign.Secondary Raynaud Phenomenon:
Arterial insufficiency of the extremities caused by various conditions including SLE, systemic sclerosis, atherosclerosis or Burger disease.Veins and Lymphatics:
Varicose Veins:Abnormally dilated, tortous veins produced by prolonged increased intraluminal pressure and loss of vessel wall support. The superficial veins of the legs are the main sites of involvement. People at risk are:
1. Occupations with long period of standings.
2. People older than 50 years.
3. Obese individuals.
4. Women with multiple pregnancies.
5. Familial tendency (wall weakness).
Morphology, the dilated veins are tortous, elongated and scarred, with thrombosis.
Clinical course,
leg edema with stasis dermatitis. No embolism. Apart from legs, varices occur also at the lower end of esophagus and ano-rectum (hemorrhoids).

Thrombophlebitis and phlebothombosis:
In 90% of cases deep veins of the legs are involved. Predisposing factors are:• Cardiac failure.
• Neoplasia.
• Pregnancy.
• Obesity.
• Postoperative state.
• Prolonged bed rest.
• Genetic hypercoagulability syndromes.
Clinically pain may be elicited by pressure over affected veins. Pain on dorsiflexion (Homer sign). Pulmonary embolism is a common and serious sequelae,-
Superior and Inferior Vena Caval Syndromes:
They are secondaries to compression or invasions by tumors.Tumors of Vessels:
Benign tumors and tumor-like conditions:
• Hemangiomas; Capillary. Cavernous. Pyogenic granuloma.
• Lymphangiomas; Capillary. Cavernous.
• Glomus tumor.
• Vascular ectasias.
• Reactive vascular proliferations.
Intermediate grade neoplasms:
• Kaposi sarcoma.
• Hemangioendothelioma.
Malignant neoplasms:
• Angiosarcoma.
• Hemangiopericytoma.
• Morphological patterns of vascular tumors
• Classically, benign vascular neoplasms are composed of well-formed vascular channels lined by ECs,.• Frankly malignant tumors show few or poorly developed vascular channels with solid, cellular, anaplastic endothelial proliferation.
• A few entities fall into an intermediate group.
