11/20/2012
cornea1
Good afternoon
Herpes simplex keratitis11/20/2012
cornea2
Pathogenesis
Herpes Simplex Virus( HSV ) is enveloped with a cuboidal capsule & double-stranded DNA genome .HSV-1 primarily causes infections above the waist that may affect the face , lips , and eyes, whereas HSV-2 causes venereally acquired infection (genital herpes ).Rarely ,HSV-2 may be transmitted to the eye through infected secretions, either venereally or at birth (ophthalmia neonatorum).
HSV transmission is facilitated in conditions of crowding and poor hygiene.
11/20/2012
cornea
3
Primary infection
Primary infection usually occurs by droplet transmission, or by direct inoculation .Due to protection bestowed by maternal antibodies, it is uncommon during the first six months of life.
Children may develop blepharoconjunctivitis, which is usually benign and self limited.
11/20/2012
cornea
4
Recurrent infection
After primary infection, the virus is carried to the sensory ganglia for that dermatome(e.g. trigeminal ganglion),where a latent infection is established. Stimuli such as fever , hormonal change, ultraviolet radiation ,trauma and trigeminal injury may cause a clinical reactivation, when the virus replicates and is transported in the sensory axons to the periphery, where there is recurrent disease.11/20/2012
cornea5
Epithelial keratitis
11/20/2012
cornea
6
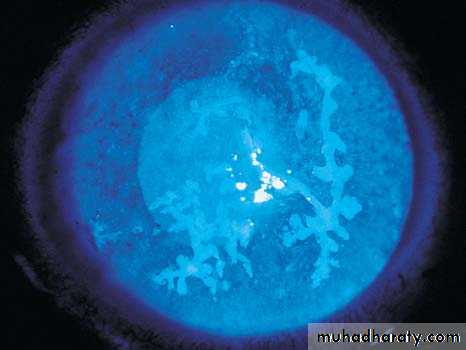
Herpetic Epithelial Keratitis
HSV dendritesHSV dendrites with fluorescein stain

11/20/2012
cornea7
Diagnosis
Presentation: may be at any age, with mild discomfort, watering and blurred vision.Signs:
Opaque epithelial cells arranged in a
1- Central desquamation results in a linear-branching (dendritic) ulcer, most frequently located centrally.
2- The ends of the ulcer have characteristic terminal bud and the bed of the ulcer stains well with fluorescein .
3- Corneal sensation is reduced.
course punctuate or stellate pattern.
11/20/2012
cornea
8
Herpes simplex epithelial keratitis
Dendritic ulcer with terminal bulbStains with fluorescein
May enlarge to become geographic
Acyclovir 3% ointment x 5 daily
Trifluorothymidine 1% drops 2-hourly
Debridement if non-compliant
Treatment


11/20/2012
9Topical steroid treatment may allow progressive enlargement of the ulcer to
geographic or " amoeboid" configuration.
11/20/2012
cornea10
Culture: can be taken by debridement of the ulcer. this relies on cytopathic effect in tissue culture, which can be used to distinguish HSV-1from HSV-2
PCR is also available.
11/20/2012
cornea11
Treatment
Topical antiviral agents most frequently used are trifluorothymidine, acyclovir and vidarabine .Acyclovir 3% ointment is used five times daily, it acts preferentially on virus laden epithelial cells.Acyclovir penetrates intact corneal epithelium and stroma ,achieving therapeutic level in the aqueous humour and can therefore be used to treat stromal herpetic keratitis.
11/20/2012
cornea12
Debridement may be used for dendritic but not geographic ulcers.
The corneal surface is wiped with sterile cellulose sponge. An antiviral agent must be used in conjunction to prevent recurrence.
11/20/2012
cornea13
Herpes Zoster Ophthalmicus (HZO)
11/20/2012cornea
14
Pathogenesis
The varicella-zoster virus ( VZV) causes chickenpox (varicella) and shingles herpes zoster).VZV and HSV belong to the same subfamily of herpes virus group and are morphologically identical but antigenically different.
11/20/2012
cornea
15
After the initial attack of chickenpox, the virus travels in a retrograde manner to the dorsal root and cranial nerve sensory ganglia, where it can remain dormant for decades. From there, it can reactivate after VZV-specific cellular immunity has faded, to cause shingles.
11/20/2012
cornea16
Risk of ocular involvement:
Involvement of the external nasal nerve (Hutchinson Sign) ,which supplies the side of the tip, the side & root of the nose , correlate significantly with subsequent development of ocular inflammation & corneal denervation because it is the terminal branch of the nasociliary nerve.11/20/2012
cornea17
Herpes Zoster Ophthalmicus (HZO ) occur most frequently in the sixth and seventh decades .In the elderly, the signs & symptoms are more sever and lasts longer
Patients with AIDS also tend to have more sever disease.
11/20/2012cornea
18
ِAcute Systemic Disease
Clinical FeaturesA prodromal phase: lasting 3-5 days with tiredness, fever, malaise and headache precedes the appearance of the rash.
11/20/2012
cornea
19
Skin lesions appears initially as a painful erythema with a maculopapular rash. Within 24 hours, groups of vesicles appears ,and those become confluent over 2-4 days.
11/20/2012
cornea
20
Herpes zoster Ophthalmicus
Iritis in 40% of casesWithin 3 weeks of onset of rash
Particularly if external nasal
branch involved Hutchinson sign
Small-medium KP
Iris atrophy - 20%


11/20/2012
cornea21
The vesicle often pass through a pastular phase before they crust and dry after 2-3 weeks. New crops of vesicles may appear in immunodeficient patients.
The rash has a dermatomal distribution and respect the midline, although inflammatory edema may cross the midline and give rise to the impression of bilateral involvement.
Skin lesion may leave extensive tissue destruction & depigmented scar.
11/20/2012
cornea22
The development of shingles in children or young adults(<50 years)should prompt a search for immunodeficiency or malignancy.
HIV infection should excluded .
11/20/2012
cornea
23
Treatment
Oral Acyclovir(800 mg five times daily for 3-7 days given within 72 hours of onset) is the treatment of choice.Patients presenting with new vesicles after 72 hours should also be treated to reduce the severity of acute HZO and the risk of post-herpetic neuralgia at six months.
11/20/2012
cornea
24
Intravenous Aciclovir(5-10 mg/kg t.i.d.) is only indicated for encephalitis. The duration of treatment should be extended for the elderly or immunosupressed patient.
Foscarnet is the drug of choice in acyclovir resistant patients.
11/20/2012
cornea25
Other oral antiviral agents : Valciclovir 1 g t.i.d. & famciclovir 750 mg daily.
Systemic steroids (prednisolone 40-60 mg per day) should be used in conjunction with systemic antiviral. They have a moderate effect at reducing acute pain and accelerating skin healing.Symptomatic treatment of skin lesions is by drying, antisepsis and cold compresses.
11/20/2012
cornea26
Acute ocular disease
Acute epithelial keratitis: develops in about 50% of patients within 2 days of onset of rash and resolve spontaneously a few days later. It is characterized by small, fine dendritic lesions, which in contrast to herpes simplex dendrites, have tapered ends without terminal buds.The lesion stain with fluorescein and rose bengal.
Treatment is with a topical antiviral.
11/20/2012
cornea27
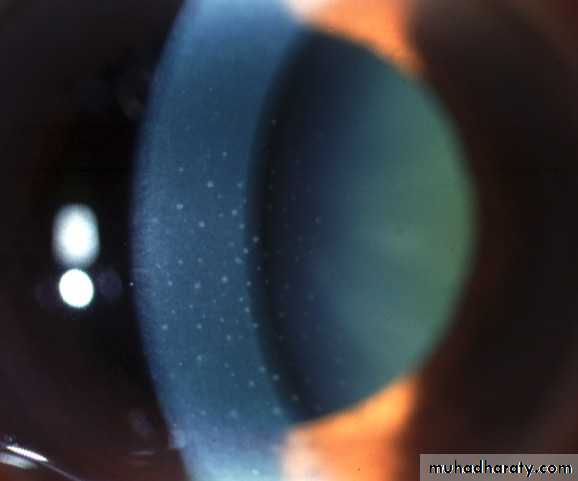
Herpes zoster keratitis
Develops in about 50% within
2 days of rash
Small, fine, dendritic or stellate epithelial lesions
Tapered ends without bulbs
Resolves within a few days
Develops in about 30% within
10 days of rash
Multiple, fine, granular deposits
just beneath Bowman membrane
Halo of stromal haze
Nummular keratitis
Acute epithelial keratitis
May become chronic
Treatment - topical steroids, if appropriate


11/20/2012
cornea28
Chronic Ocular Disease
Clinical features
Lid scarring may result in Ptosis, cicatritial entropion, Trichiasis , madarosis and notching of the lid margin.
Scleritis may become chronic and lead to patchy scleral atrophy.
Neurotrophic keratitis with reduced sensation. It may lead to sever ulceration , secondary bacterial infection & even perforation.
11/20/2012
cornea29
Post-herpetic neuralgia
Clinical featuresPost-herpetic neuralgia is pain that persist after the rash has healed usually defined as an interval of three months. Pain may be constant or intermittent , worse at night & aggravated by minor stimuli , touch and heat. It generally improves slowly with time. Neuralgia may lead to depression and impair the quality of life.
11/20/2012
cornea
30
Treatment
Cold compress , topical capsaicin or local anesthetic (lidocaine 5%)cream may be effective.Simple analgesics such as paracetamol up to 4 g daily.
Stronger analgesics such as codeine
Amitriptylin 10-25 mg at night, increase gradually to 75 mg daily if appropriate.
Carbamazepine 400 mg daily for lancinating pain.
11/20/2012
cornea
31
Relapsing Phase
In the relapsing phase, lesions may reappear years after acute disease & lid scarring may be the only diagnostic clue.Reactivation of keratitis.
Episcleritis , Scleritis or iritis can occur. Low-dose topical steroid (Fluorometholone 0.1% daily) is effective after the acute event has been controlled .
11/20/2012
cornea32
11/20/2012
cornea33
11/20/2012
cornea34
MCQ sample:
Herpetic epithelial keratitis characterized by:A- central corneal lesion
B- dendrites characterized by terminal bulbsC- tends to be peripheral & multifocal lesions
D- corneal senation is reduced
11/20/2012
cornea
35
11/20/2012
cornea36

Thank you